(UroToday.com) The 2025 EAU annual meeting featured a session on managing metastatic castration resistant prostate cancer (mCRPC) after triplet therapy for metastatic hormone sensitive prostate cancer (mHPSC) and a presentation by Dr. Fred Saad discussing the utility of radium-223 alone or in combination. There are no phase 3 studies that have clearly demonstrated the best approach after triplet therapy, with available options including cabazitaxel, lutetium, PARP inhibitors +/- an androgen receptor pathway inhibitor (if BRCA or HRR mutation present), and radium-223 (as long as there is no visceral disease). Ideally, eligible patients will be exposed to all available options.
With regards to radium-223, Dr. Saad started by discussing the ALSYMPCA trial,1 with the following trial design:
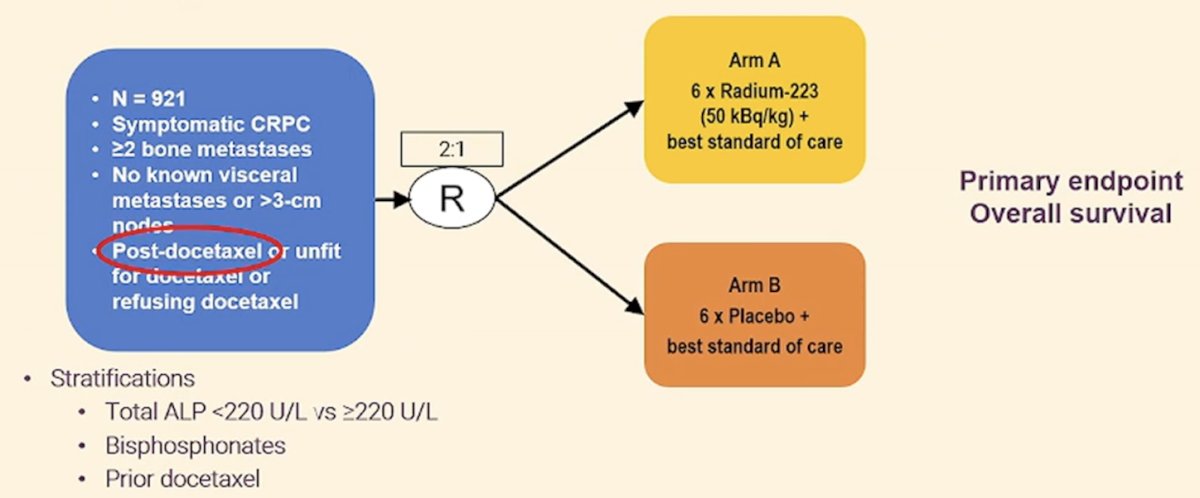
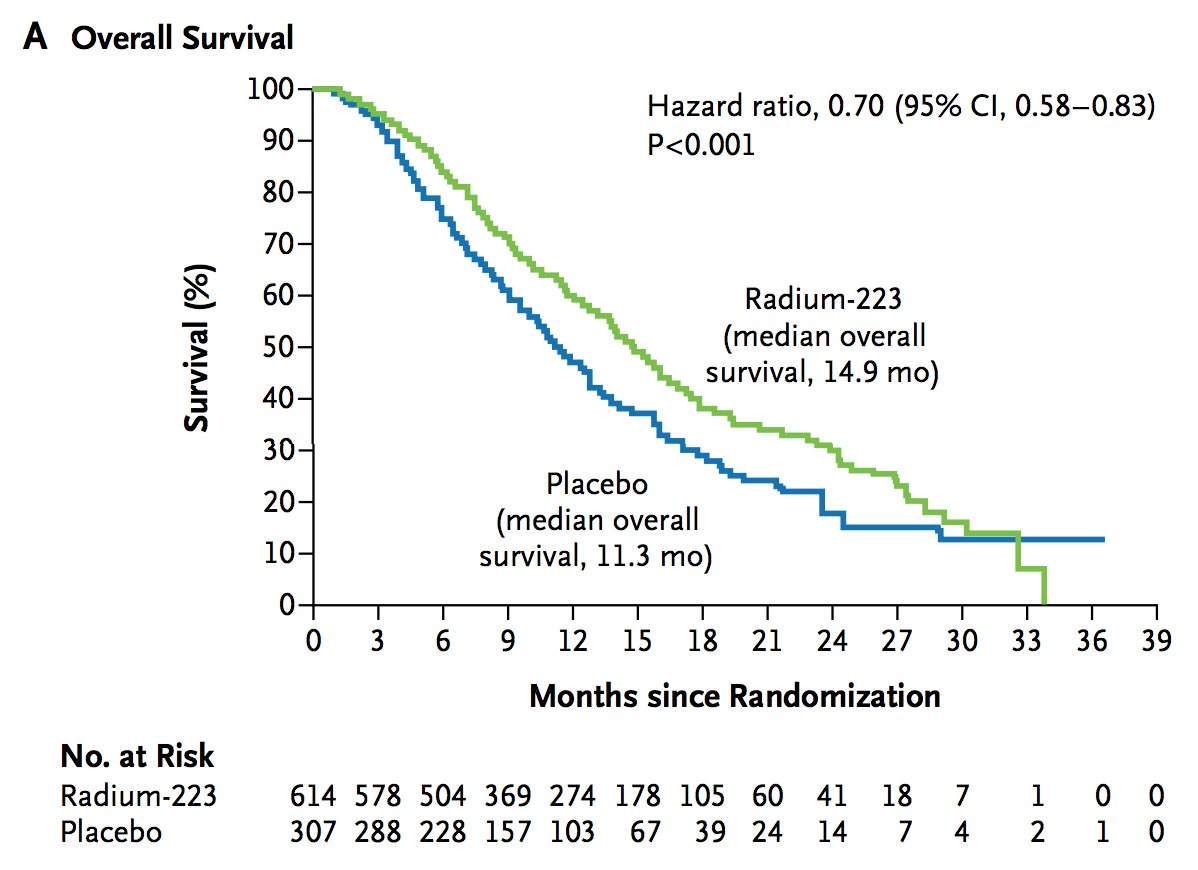
In ALSYMPCA, patients receiving radium-223 had significantly improved median overall survival (14.9 months) versus placebo (11.3 months; HR 0.70, 95% CI 0.58–0.83):
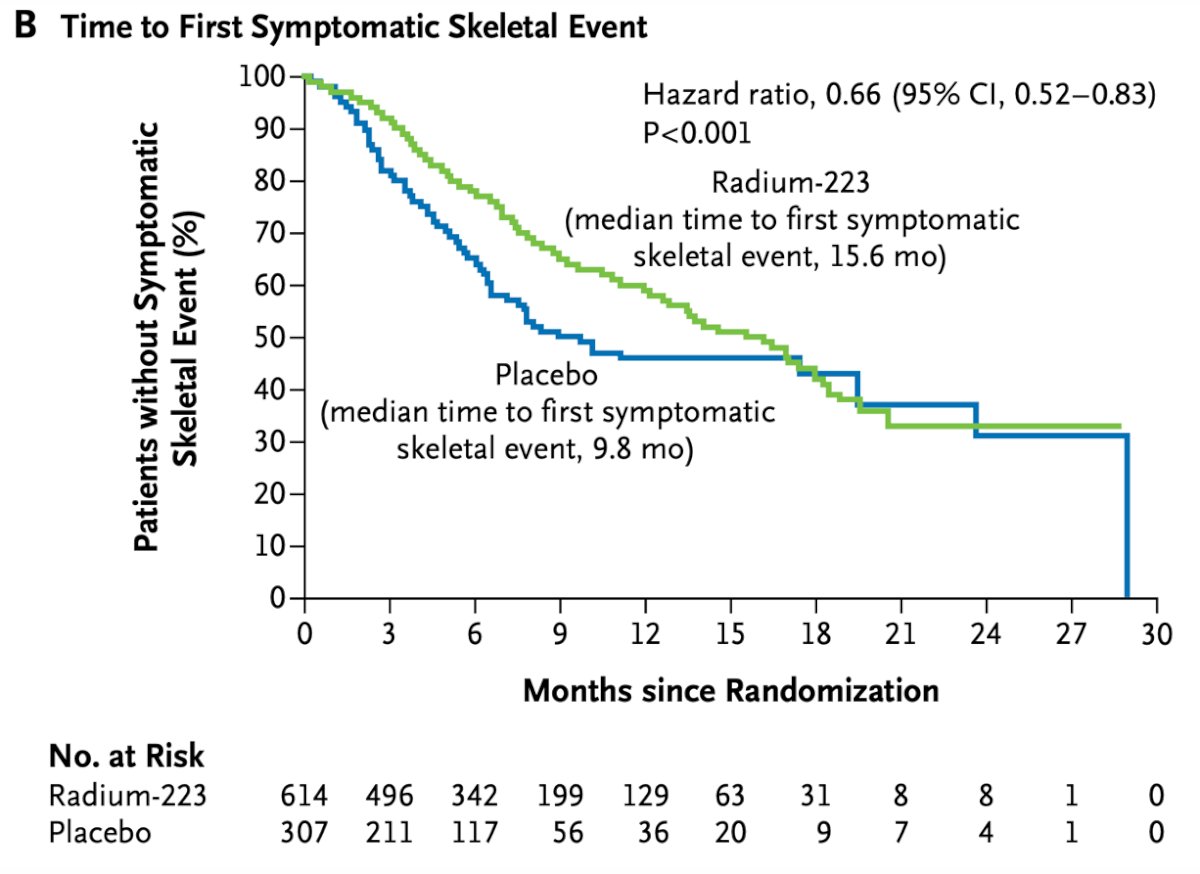
Use of radium-223 was also associated with significantly prolonged time to the first symptomatic skeletal event (15.6 versus 9.8 months, HR 0.66, 95% CI 0.52–0.83):
When considering the timing of radium-223 and docetaxel chemotherapy, Dr. Saad notes that it is important to consider a prespecified subgroup analysis from ALSYMPCA that was undertaken to assess the effect of previous docetaxel use on the efficacy and safety of radium-223.2 In this analysis, there were 526 (57%) of 921 randomly assigned patients that had received previous docetaxel treatment (352 in the radium-223 group and 174 in the placebo group) and 395 (43%) had not (262 in the radium-223 group and 133 in the placebo group). Radium-223 prolonged median overall survival compared with placebo, irrespective of previous docetaxel use (previous docetaxel use, HR 0.70, 95% CI 0.56-0.88; no previous docetaxel use, HR 0.69, 0.52-0.92).

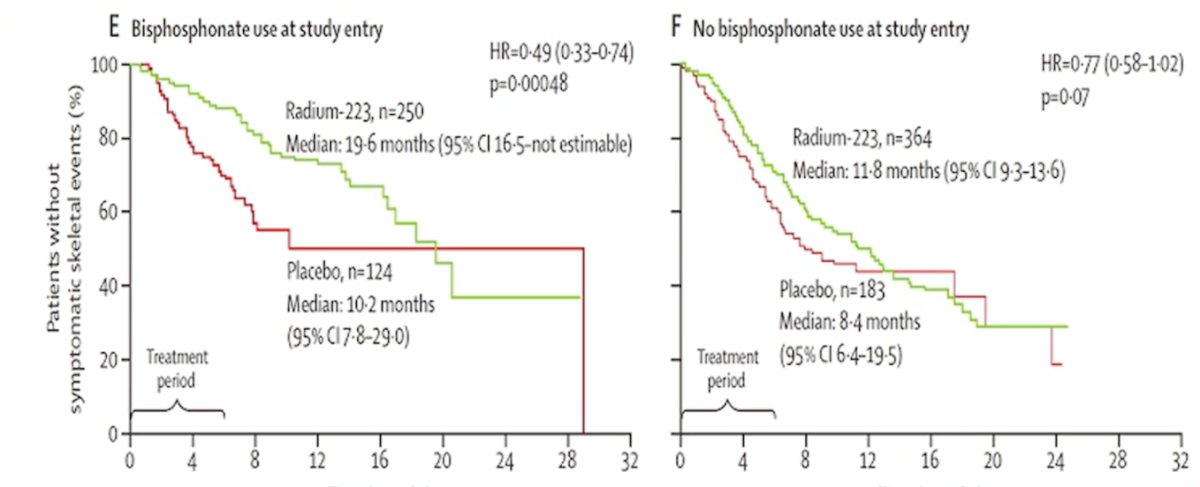
Dr. Saad also discussed the impact of radium-223 + bisphosphonate use at the time of entry based on additional analyses from the ALSYMPCA dataset,3 noting a substantial improvement in time to skeletal related events with the use of both agents:
Looking at more contemporary data, Dr. Saad notes that in 2016 his group looked at radium-223 and concomitant therapies in mCRPC patients as part of an international, early access, open-label, single-arm phase 3b trial.4 Among 839 patients, he notes that the majority of patients had prior docetaxel and ~50% had prior abiraterone or enzalutamide. In this analysis, the median overall survival was 16 months (95% CI 13 – NR):
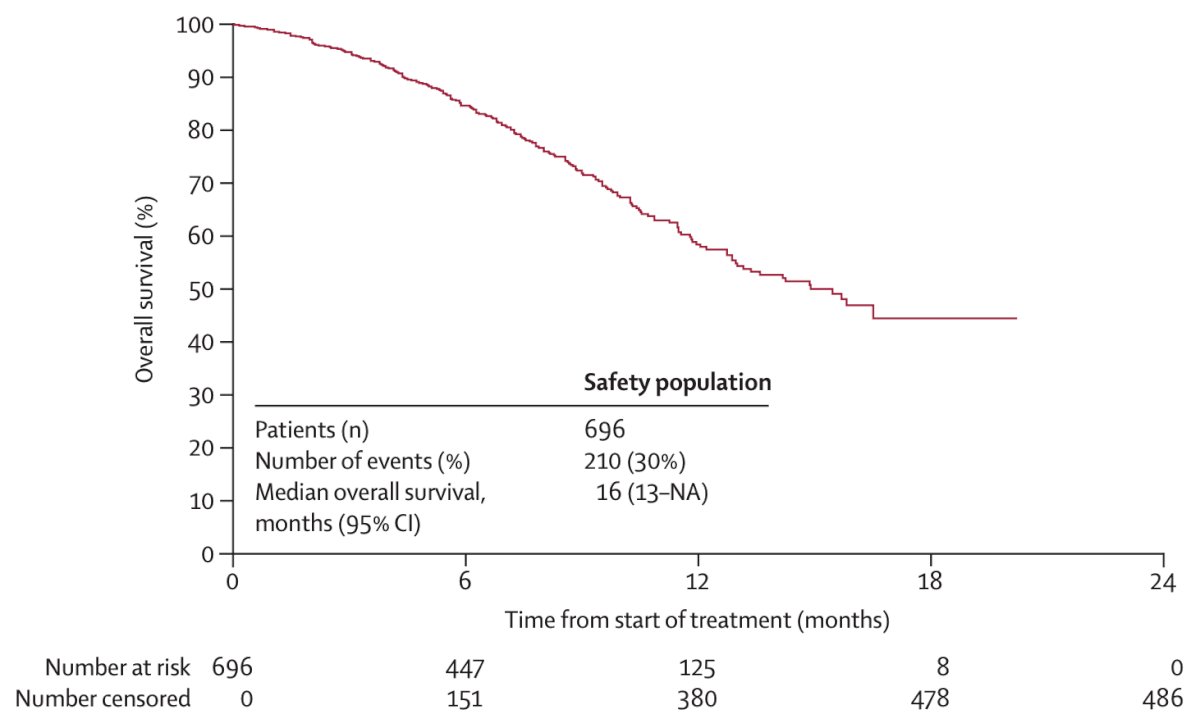
Moreover, in an exploratory analysis, median overall survival was longer for:
- Patients with baseline ALP less than the upper limit of normal (ULN; median NR, 95% CI 16 months-NR) vs ALP >= ULN (median 12 months, 95% CI 11-15)
- Patients with baseline hemoglobin levels >10 g/dL (median 17 months, 95% CI 14-NR) vs hemoglobin levels < 10 g/dL (median 10 months, 95% CI 8-14)
- Patients with a baseline ECOG performance status of 0 (median NR, 95% CI 17 months-NR) vs ECOG performance status of 1 (median 13 months, 95% CI 11-NR) vs ECOG performance status of >=2 (median 7 months, 95% CI 5-11)
- Patients with no reported baseline pain (median NR, 95% CI 16 months-NR) vs mild pain (median 14 months, 95% CI 13-NR) vs moderate-severe pain (median 11 months, 95% CI 9-13)
Overall survival was also significantly improved with radium-223 among those receiving prior abiraterone or enzalutamide, as well as in those receiving denosumab:

Next, Dr. Saad discussed PEACE-3, which was an international study in 446 patients with mCRPC and bone metastases randomized 1:1 to combination of enzalutamide and radium-223 versus enzalutamide alone:
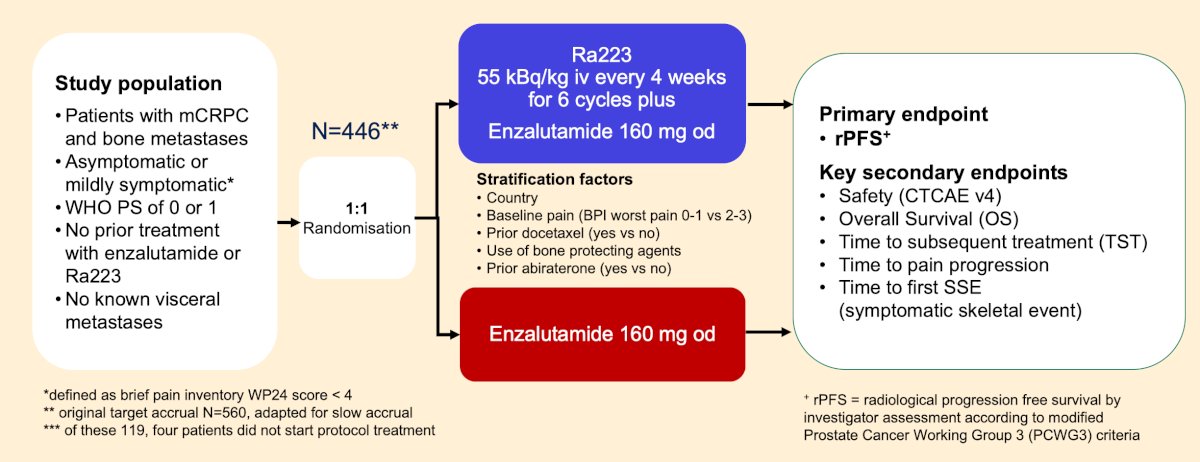
As of March 18, 2018, with 119 (27%) of 446 patients enrolled, an urgent safety letter made co-administration of zoledronic acid or denosumab obligatory. The trial demonstrated significant improvement in the primary endpoint of radiological progression-free survival: HR 0.69 (95% CI 0.54-0.87; p = 0.0009), with a median radiological progression-free survival of 16.4 (95% CI 13.8-19.2) months in the enzalutamide arm and 19.4 (95% CI 17.1-25.3) months in the enzalutamide and radium-223 arm:

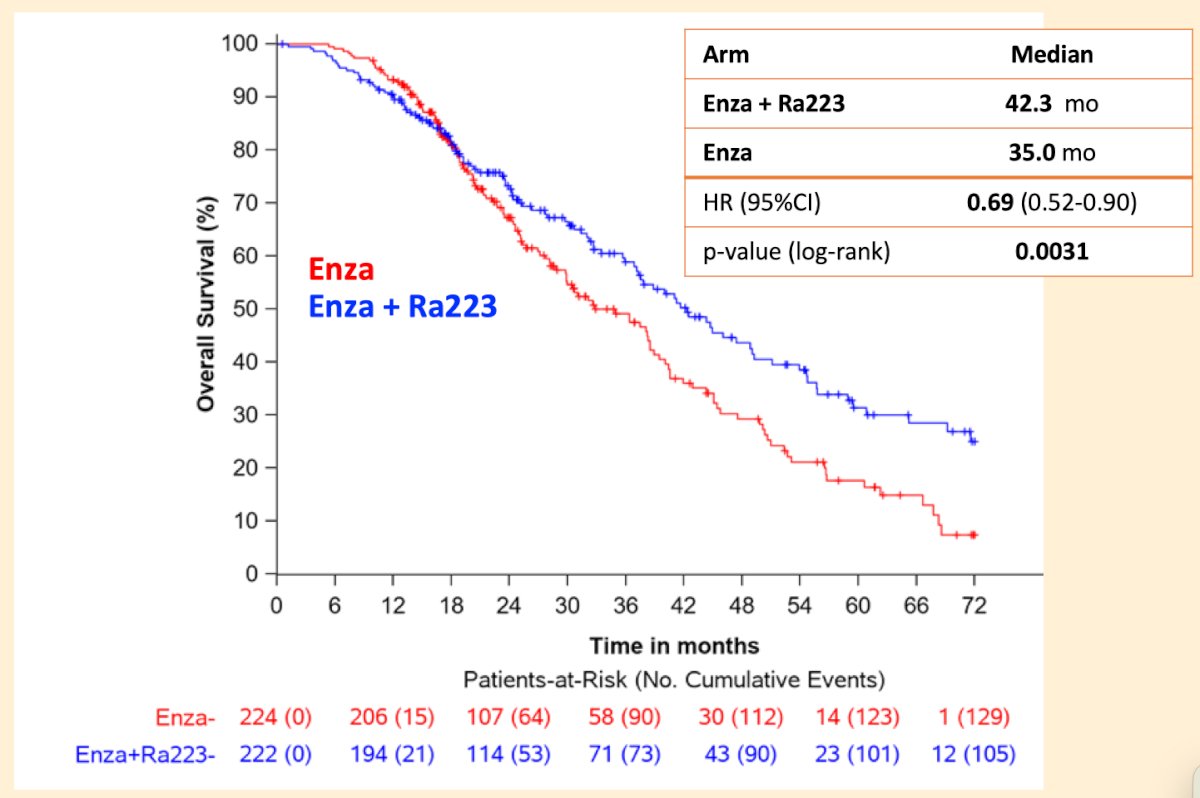
Additionally, the interim analysis (at 80% of events) showed that the key secondary endpoint of overall survival also favored the enzalutamide and radium-223 arm (HR 0.69, 95% CI 0.52-0.90, p = 0.0031):
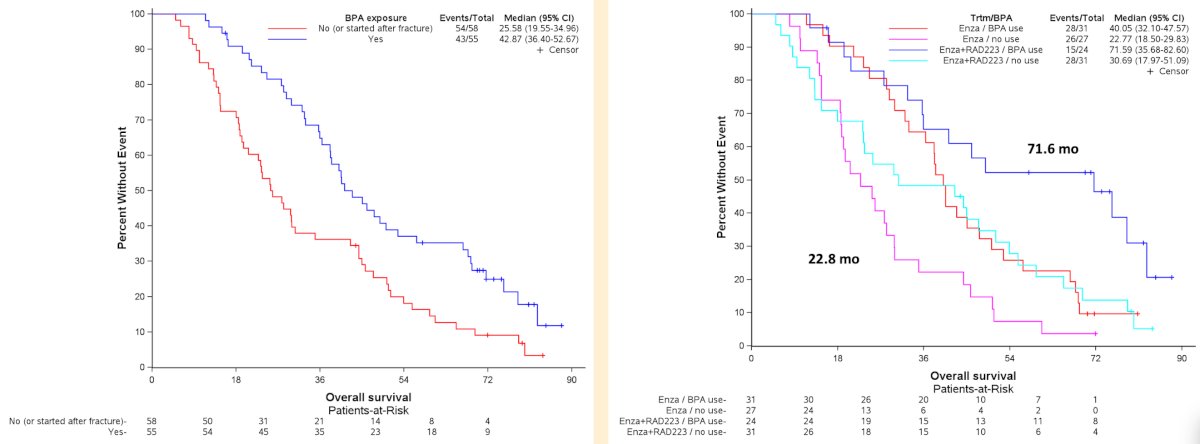
Presented earlier at EAU 2025, Dr. Saad discussed the impact of bone protecting agents in PEACE-3. In this analysis, median radiological progression-free survival was longer by 14 months from 13.24 months without to 26.91 months with bone protecting agents use (HR 0.60, 95% CI 0.39-0.93) and this difference was similar across both arms. Patients in the enzalutamide and radium-223 arm with bone protecting agents had a median radiological progression-free survival of 28.85 months versus only 12.9 months for those in the enzalutamide arm without bone protecting agents:
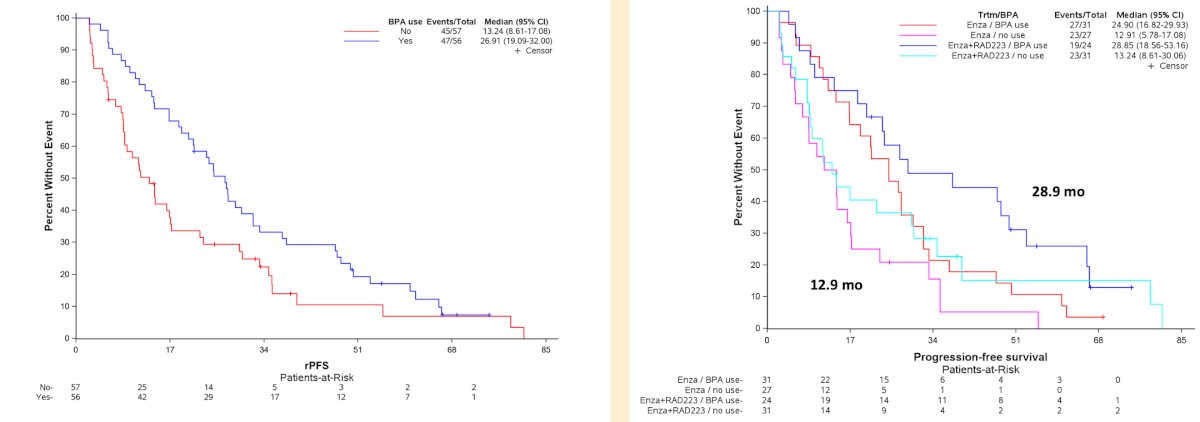
Median overall survival was longer by 17 months from 25.58 months without to 42.87 months with bone protecting agents use (HR 0.56, 95%CI 0.37-0.86). Again, this difference was notable between the enzalutamide and radium-223 arm with bone protecting agents and the enzalutamide arm without bone protecting agents with median overall survival of 71.59 months versus 22.77 months, respectively:
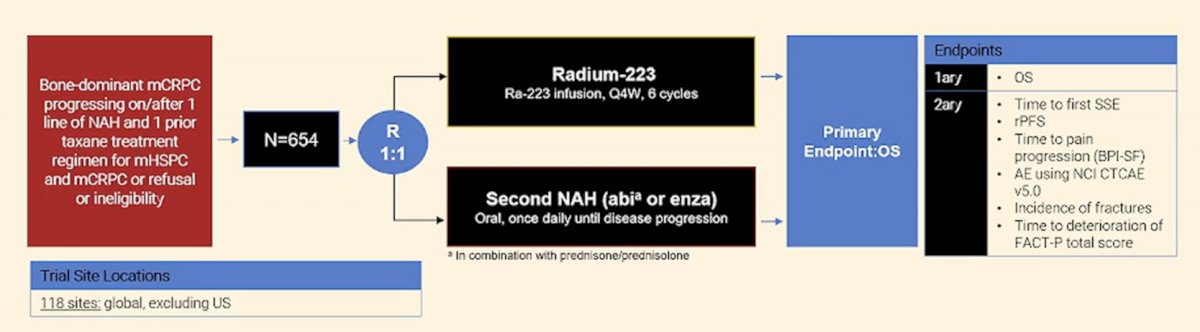
Finally, Dr. Saad discussed two ongoing trials assessing radium-223, first highlighting the RADIANT trial, which is a multicenter trial comparing radium-223 versus novel anti-hormonal therapy in bone-dominant mCRPC progressing on or after one line of novel anti-hormonal therapy + a taxane:
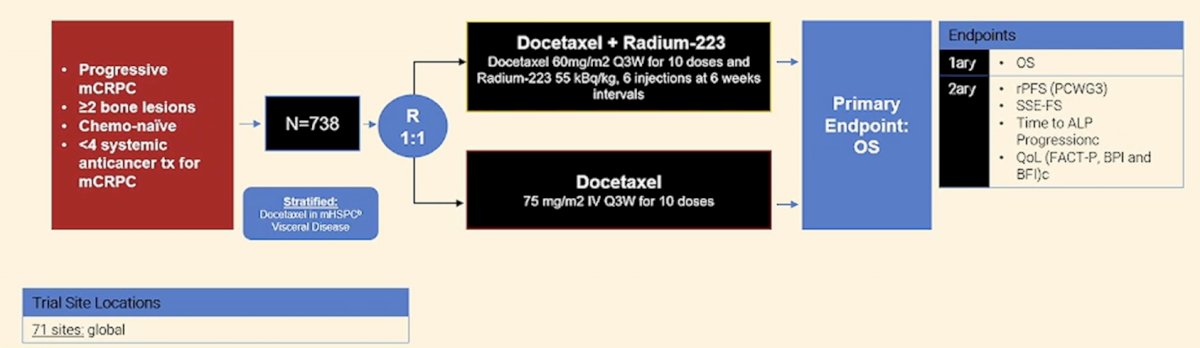
The second trial is the DORA trial, a randomized phase 3 trial comparing docetaxel versus docetaxel in combination with radium-223 in patients with chemotherapy naïve mCRPC:
Dr. Saad concluded his presentation by discussing the utility of radium-223 alone or in combination with the following take home points:
- Radium-223 (with a bone protecting agent) can be considered as a therapeutic option post triplet therapy as an alternate to taxane or lutetium for patients with bone predominant mCRPC with no visceral metastases
- Although no level 1 evidence, there is some evidence to suggest that combining radium and an androgen receptor pathway inhibitor (with a bone protecting agent) may provide added benefit over radium-223 alone
- This is likely to be much better than a simple androgen receptor pathway inhibitor switch
- If it is considered, data suggests that earlier use of radium may be more effective, with less pain, better ECOG performance status, higher hemoglobin, and lower ALP level
- Ongoing studies will address some of these unanswered questions
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain between March 21st and 24th 2025
References:
- Parker C, Nilsson S, Heinrich D, et al. Alpha emitter radium-223 and survival in metastatic prostate cancer. N Engl J Med 2013;369(3):213-223.
- Hoskin P, Sartor O, O’Suillivan JM, et al. Efficacy and safety of radium-223 dichloride in patients with castration-resistant prostate cancer and asymptomatic bone metastases, with or without previous docetaxel use: A prespecified subgroup analysis from the randomized, double-blind, phase 3 ALSYMPCA trial. Lancet Oncol. 2014 Nov;15(12):1397-1406.
- Sartor O, Coleman R, Nilsson S, et al. Effect of radium-223 dichloride on symptomatic skeletal events in patients with castration-resistant prostate cancer and bone metastases: Results from a phase 3, double-blind, randomized trial. Lancet Oncol. 2014 Jun;15(7):738-746.
- Saad F, Carles J, Gillessen S, et al. Radium-223 and concomitant therapies in patients with metastatic castration-resistant prostate cancer: An international, early access, open-label, single-arm phase 3b trial. Lancet Oncol. 2016 Sep;17(9):1306-1316.