(UroToday.com) The 2025 EAU annual meeting featured a session on managing metastatic castration resistant prostate cancer (mCRPC) after triplet therapy for metastatic hormone sensitive prostate cancer (mHPSC) and a presentation by Dr. Christopher Sweeney discussing his algorithm for decision making in mCRPC.
For first line mCRPC therapy, the decision must be based on a personalized approach. For those that have a biomarker “detected” (exome PTEN, RB1, p53, BRCA1/2, CDK12, PALB2, and PSMA PET) mCRPC, the following personalized treatment approach should be used: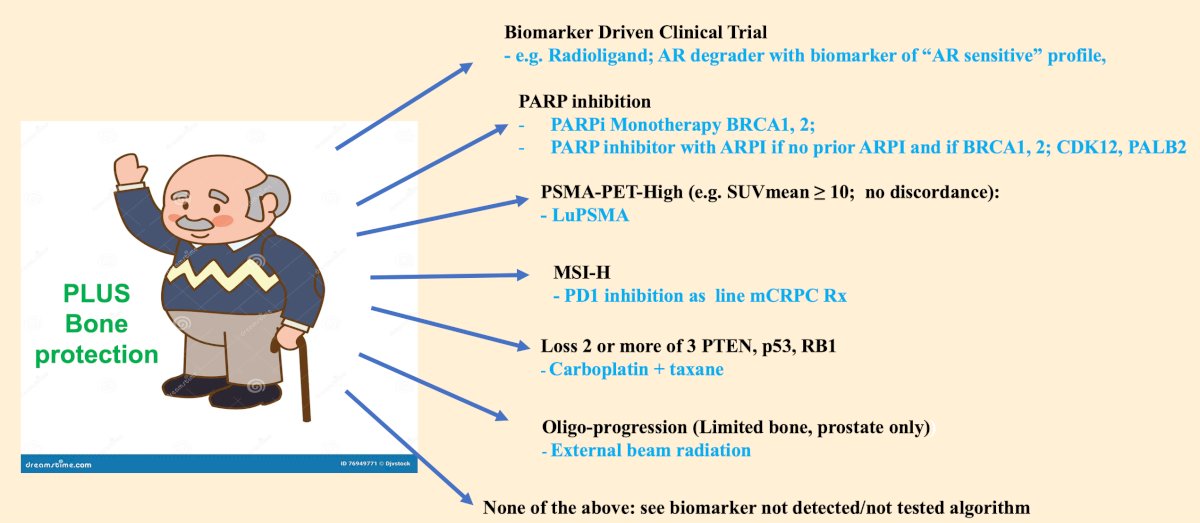
For those with a biomarker “not detected/unknown/not tested” mCRPC (or after biomarker directed therapy), the following personalized treatment approach should be used: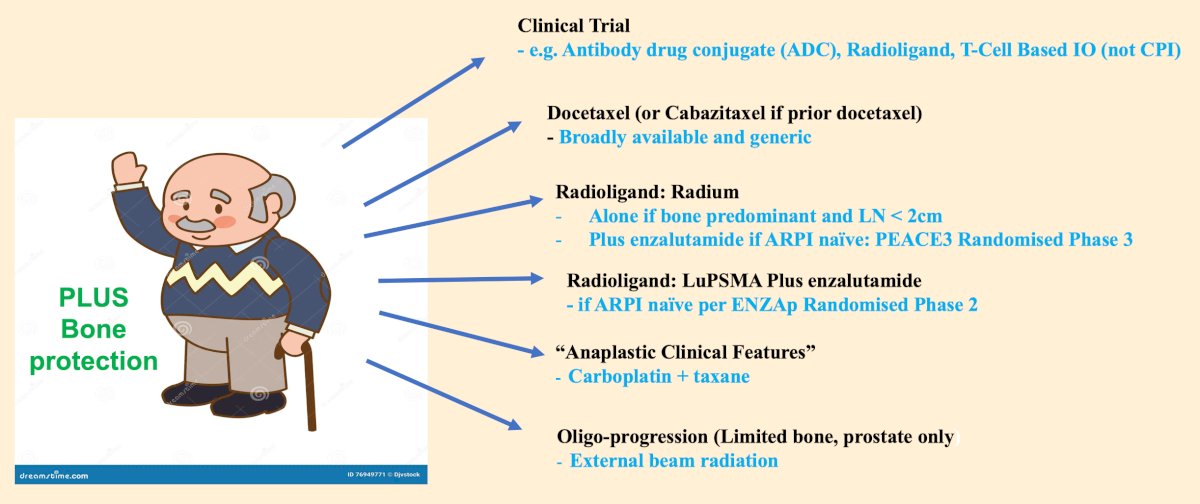
For LuPSMA radioligand therapy, previous work from TheraP1 and VISION2 has assessed the value of SUVmean on overall survival. For patients with SUVmean > 10 and treated with LuPSMA, the median overall survival is ~21 months (approximately 30% of patients enrolled), and without LuPSMA treatment overall survival is ~15 months. For patients with SUVmean < 10 and treated with LuPSMA, the median overall survival is ~14 months (approximately 70% of patients enrolled), and without LuPSMA treatment overall survival is ~12 months:![For LuPSMA radioligand therapy, previous work from TheraP [1] and VISION [2] has assessed the value of SUVmean on overall survival. For patients with SUVmean > 10 and treated with LuPSMA, the median overall survival is ~21 months (approximately 30% of patients enrolled) and without LuPSMA treatment overall survival is ~15 months. For patients with SUVmean < 10 and treated with LuPSMA, the median overall survival is ~14 months (approximately 70% of patients enrolled) and without LuPSMA treatment overall survival is ~12 months](/images/com-doc-importer/200-eau-2025/eau-2025-my-algorithm-for-decision-making-in-mcrpc/image-2.jpg)
Dr. Sweeney notes that the 70% of patients with SUVmean <10 are getting a relatively inactive therapy and may miss out on a more active therapy (ie. BRCA and PARP inhibitors) if they progress and are not able to be treated secondary to clinical decline. With regard to PARP inhibition, the benefit is limited to key mutations, given that PARP inhibition actively depends on the DDR pathway. These key mutations are BRCA2, BRCA1, CDK12, and PALB2, with little benefit for ATM and CHEK2 mutations: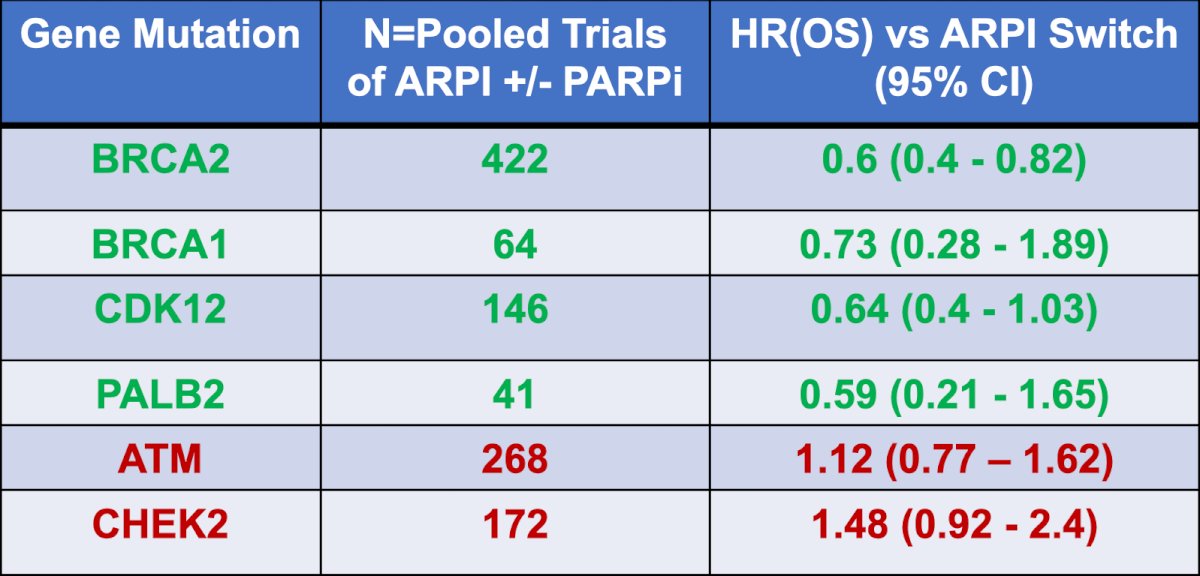
Data from PROpel3 and TALAPRO-24 have shown that a PARP inhibitor plus an androgen receptor pathway inhibitor has a clear benefit associated with some mutations. The following table shows the gene mutation, treatment, and overall survival benefit:![Date from PROpel [3] and TALAPRO-2 [4] have shown that a PARP inhibitor plus an androgen receptor pathway inhibitor has a clear benefit associated with some mutations. The following table shows the gene mutation, treatment and overall survival benefit:](/images/com-doc-importer/200-eau-2025/eau-2025-my-algorithm-for-decision-making-in-mcrpc/image-4.jpg)
Dr. Sweeney notes that there is some associated toxicity with PARP inhibitors, in particular a notably high rate (42%) of blood transfusions in TALAPRO-2, and an unclear rate in the use of PARP inhibitors at the time of progression, especially in patients with BRCA mutation. Although rare, an MMRd mutation should be considered for PD1 inhibition, with the aim to access this option via a disease agnostic approval. Although toxicity goes up and efficacy goes down in the real world, the data is still encouraging: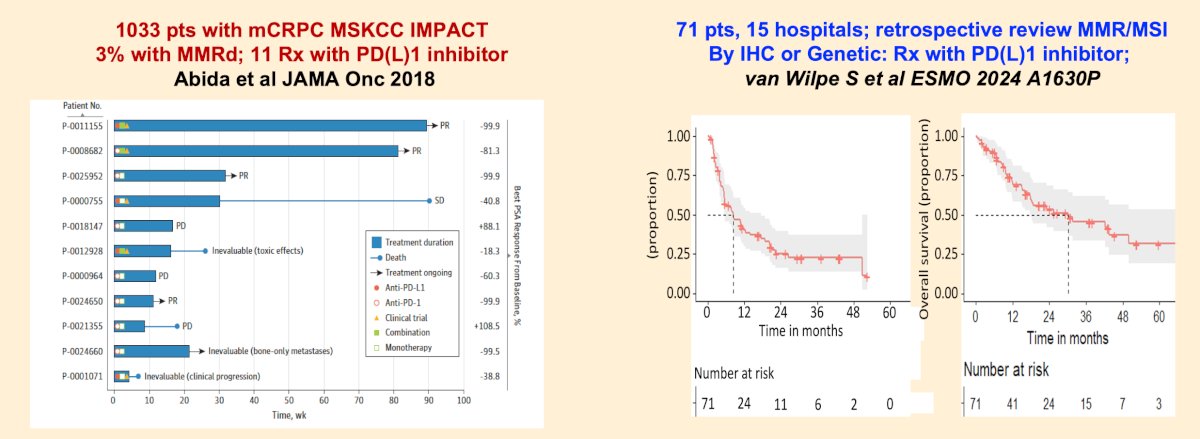
Previously, a phase 1-2 trial assessed whether adding carboplatin to cabazitaxel would improve the outcomes of men with metastatic castration-resistant prostate cancer.5 Among 160 patients in the phase 2 portion of the trial (n = 79 cabazitaxel; n = 81 cabazitaxel + carboplatin), at a median follow-up of 31.0 months (IQR 20.5-37.1), this combination improved the median progression-free survival from 4.5 months (95% CI 3.5-5.7) to 7.3 months (95% CI 5.5-8.2; HR 0.69, 95% CI 0.50-0.95, p = 0.018). Dr. Sweeney emphasized that a “molecular signature” of anaplastic mCRPC (loss of 2 of 3 of PTEN, RB, p53) showed benefit with cabazitaxel + carboplatin: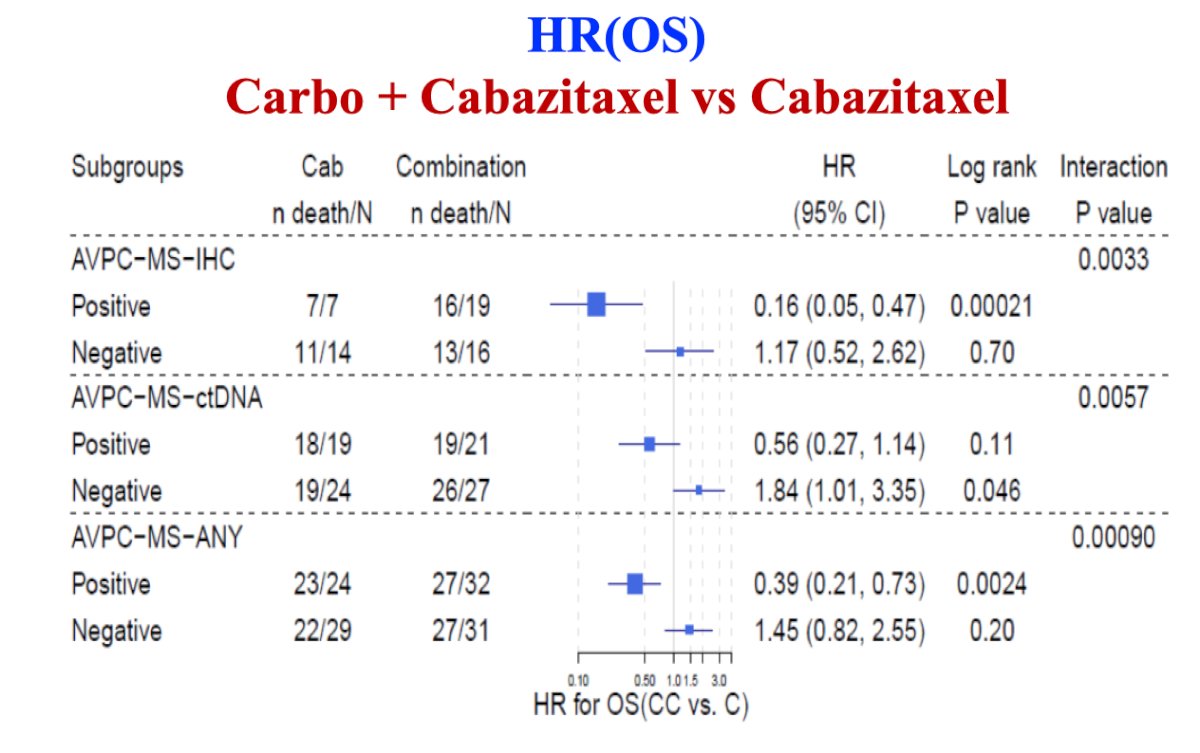
For patients that are biomarker negative or unknown, Dr. Sweeney recommends first line consideration of radium-223 + enzalutamide based on data from PEACE-3, or enzalutamide + LuPSMA for poor risk mCRPC based on data from ENZA-p:6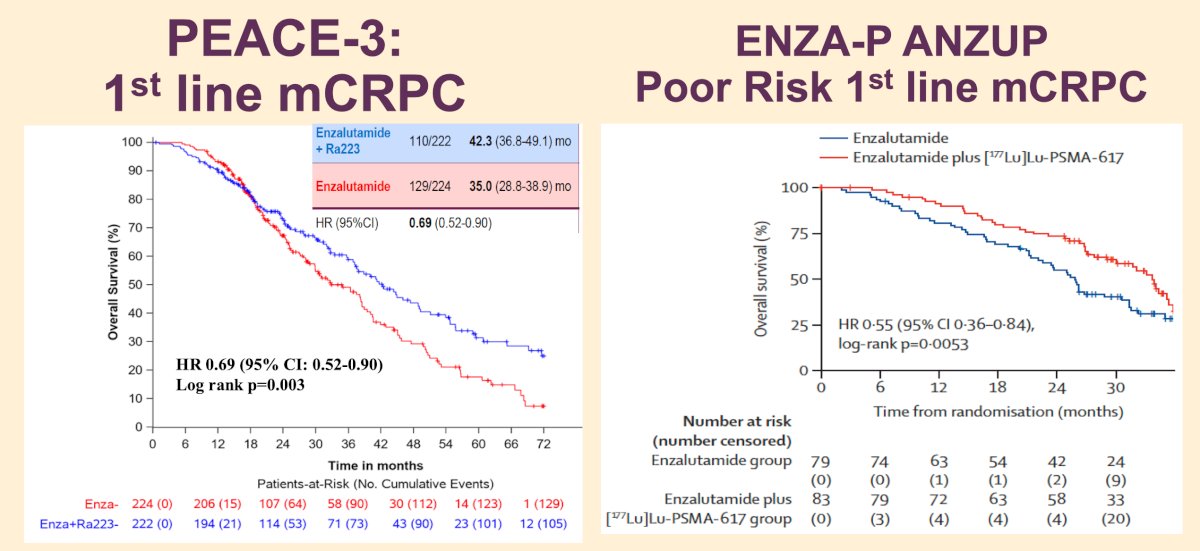
RAPSON, an open-label multicenter randomized trial of radium-223 -> docetaxel versus docetaxel -> radium-223 sequence in mCRPC was initially presented at ESMO 2024 and may also be an option in biomarker negative or unknown mCRPC. In this trial, 70 patients were initially randomized 1:1 to receive radium-223 or docetaxel as first treatment followed by docetaxel or radium-223, respectively, at the progression: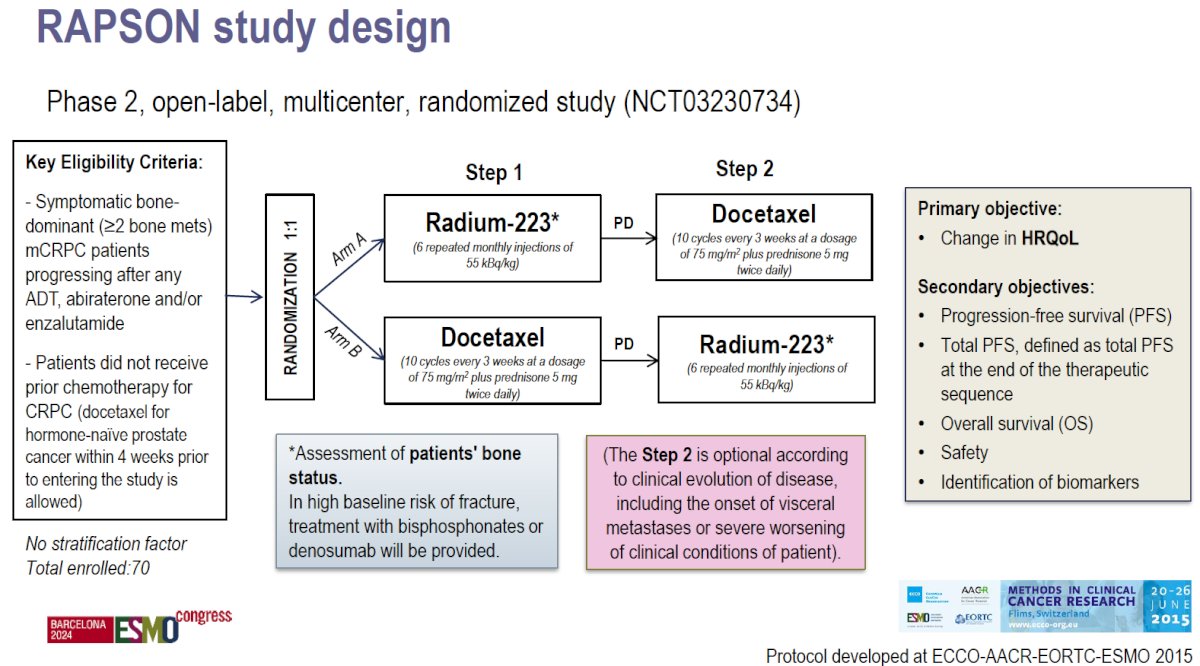
Efficacy results reported no difference in progression-free survival and overall survival between radium-223 and docetaxel evaluated only for step 1 as only 14 patients completed step 2 so far: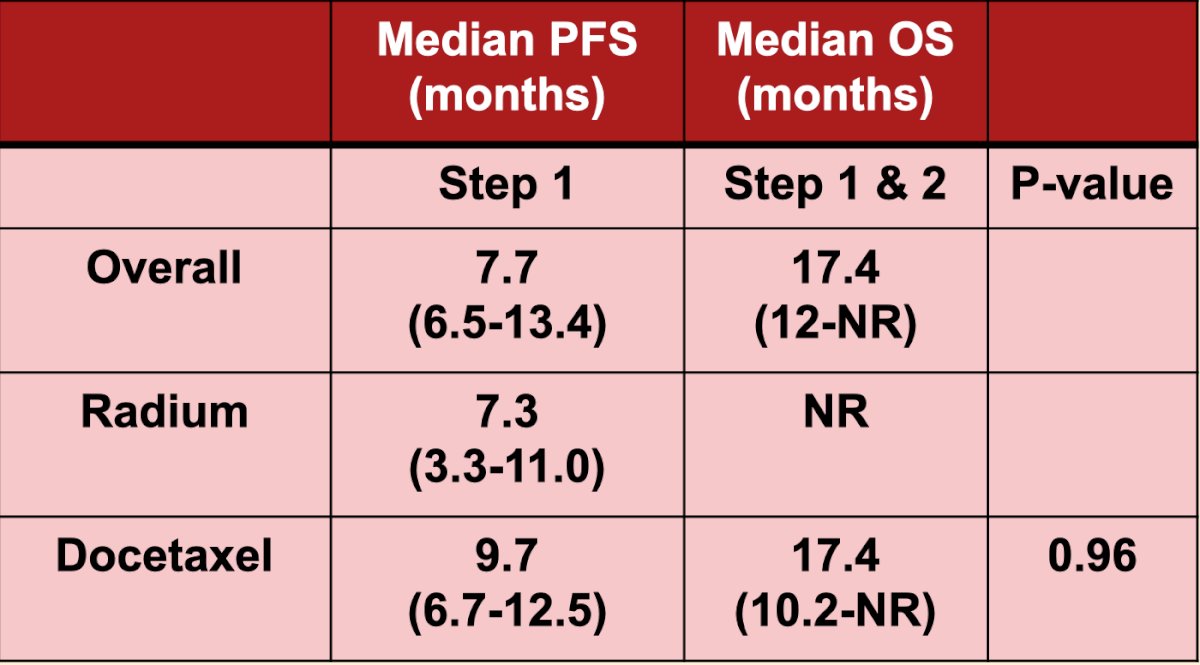
Dr. Sweeney notes that some of these patients likely have BRCA or tumor suppressor mutations and still had an overall survival benefit, with the hypothesis that efficacy may be higher in patients without a BRCA or tumor suppressor gene mutation.
Dr. Sweeney emphasized that his algorithm for treating mCRPC does not include abiraterone or ‘amide after ‘amide. He notes that abiraterone or enzalutamide after ADT alone have hazard ratios for overall survival ranging from 0.70-0.80 and median overall survival of 3 years. However, there is variable AR dependence of metastatic prostate cancer after ADT + androgen receptor pathway inhibitors, as evidenced for enzalutamide and abiraterone switch: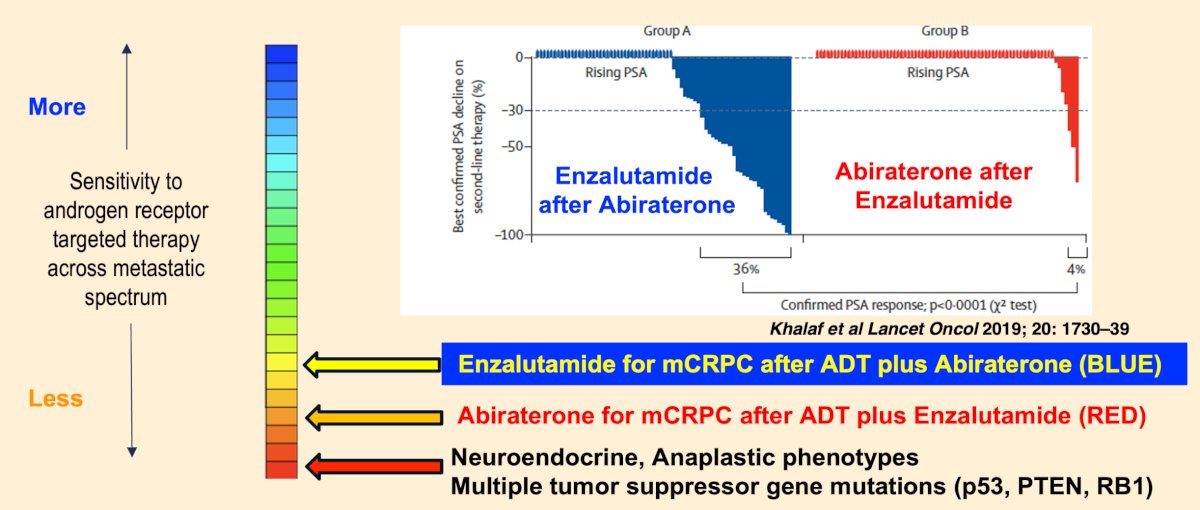
He cautions that just because it is seen to be “used” in real world evidence datasets or as a control arm of a trial does not mean it is a good treatment option.
Dr. Sweeney concluded his presentation discussing his algorithm for decision making in mCRPC with the following take home points:
- Many treatment options have emerged
- There is no single treatment that is best for all patients
- We should profile tumors as best we can to define the best first line mCRPC treatment option for each patient with personalized medicine
- The most benefit is with the first line treatment and many do not get to the next line of treatment
- Treatment beyond the first line is a bonus
- A personalized approach should be taken for every cancer patient
Presented by: Christopher Sweeney, MBBS, South Australian Immunogenomics Cancer Institute, University of Adelaide, Adelaide, Australia
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the European Association of Urology (EAU) 2025 Annual Meeting, Madrid, Spain, Fri, Mar 21 – Mon, Mar 24, 2025.
References:
- Hofman MS, Emmett L, Sandhu S, et al. Overall survival with [177Lu]Lu-PSMA-617 versus cabazitaxel in metastatic castration-resistant prostate cancer (TheraP): Secondary outcomes of a randomized, open-label, phase 2 trial. Lancet Oncol. 2024 Jan;25(1):99-107.
- Kuo PH, Morris MJ, Hesterman J, et al. Quantitative 68Ga-PSMA-11 PET and Clinical Outcomes in Metastatic Castration-resistant prostate cancer following 177Lu-PSMA-617 (VISION Trial). Radiology. 2024 Aug;312(2):e233460.
- Saad F, Clarke NW, Oya M, et al. Olaparib plus abiraterone versus placebo plus abiraterone in metastatic castration-resistant prostate cancer (PROpel): final prespecified overall survival results of a randomized, double-blind, phase 3 trial. Lancet Oncol. 2023 Oct;24(10):1094-1108.
- Agarwal N, Azad AA, Carles J, et al. Talazoparib plus enzalutamide in men with first-line metastatic castration-resistant prostate cancer (TALAPRO-2): A randomized, placebo-controlled, phase 3 trial. Lancet. 2023 Jul 22;402(10398):291-303.
- Corn PG, Heath EI, Zurita A, et al. Cabazitaxel plus carboplatin for the treatment of men with metastatic castration-resistant prostate cancers: A randomized, open-label, phase 1-2 trial. Lancet Oncol. 2019 Oct;20(10):1432-1443.
- Emmett L, Subramaniam S, Crumbaker M, et a. [177Lu]Lu-PSMA-617 plus enzalutamide in patients with metastatic castration-resistant prostate cancer (ENZA-p): An open-label, multicentre, randomized, phase 2 trial. Lancet Oncol. 2024 May;25(5):563-571.