(UroToday.com) The 2025 EAU annual meeting featured a plenary session on optimizing the patient journey and a presentation by Dr. Sarah Psutka discussing the impact of exercise, personalized programs, and digital devices on prehabilitation. Dr. Psutka started her presentation by defining prehabilitation as a process of improving the functional capability of a patient prior to a surgical procedure/medical treatment so that the patient can withstand treatment-associated functional decline/physiologic insult. At the core of prehabilitation are several domains, including mental, nutritional, and physical. Resilience is defined as an individual’s ability to maintain psychological and physical functioning in the face of stressors. Thus, the hype is: “can we make our patients more resilient to the stresses of surgery with exercise prehabilitation?”
Dr. Psutka notes that “exercise as medicine” is part of comprehensive cancer care. For overall health, the aim is to meet the current exercise guidelines for adults: moderate aerobic exercise of at least 150-300 minutes per week, or vigorous aerobic exercise of at least 75-150 minutes per week. For either option, it should be combined with resistance exercise 2x per week. The following figure highlights how exercise helps during cancer treatment:

Dr. Psutka emphasized that for people during and following cancer treatment, research shows that even low/small amounts of exercise can still help with the following cancer treatment-related symptoms:
- Cancer-related fatigue
- Health related quality of life
- Physical function
- Anxiety
- Depression
- Sleep
- Lymphedema
- Bone health
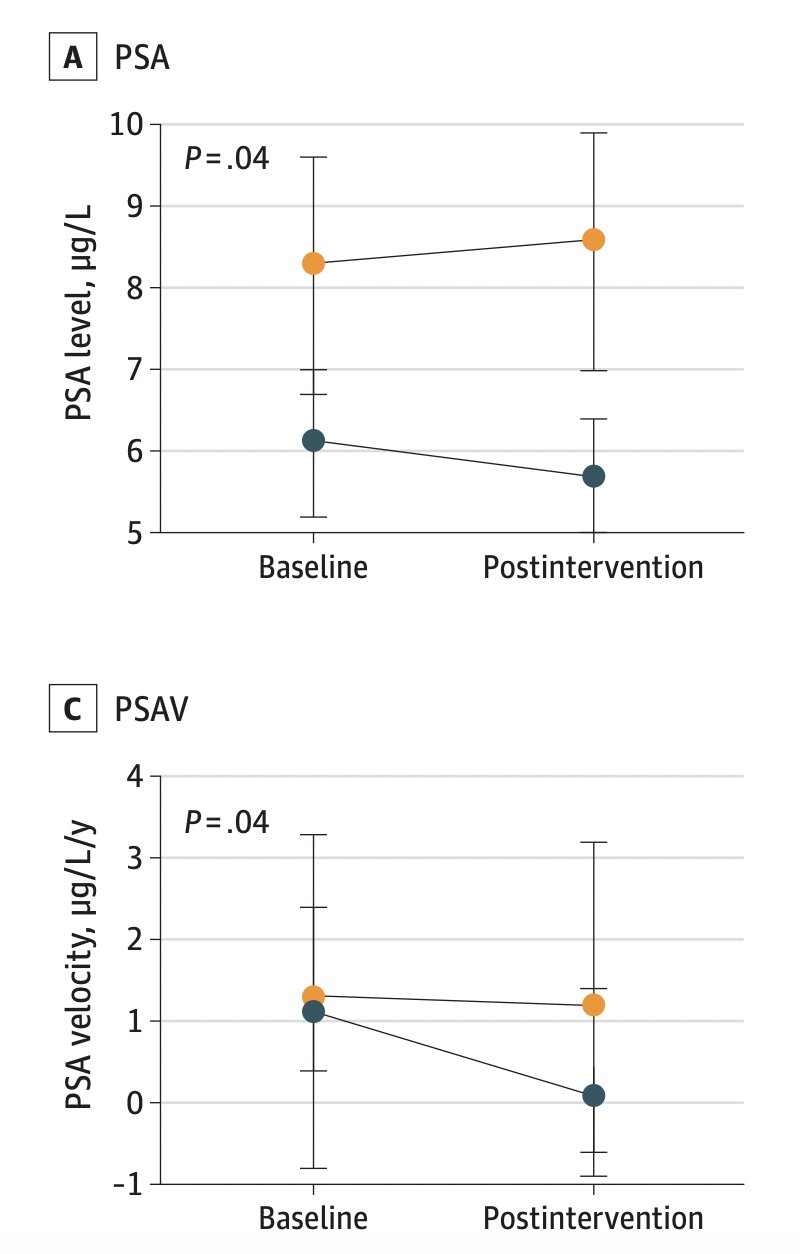
Despite all of the aforementioned benefits, there is limited uptake of prehabilitation in real life. Notably, only 7% of patients with cancer meet guideline recommendations, and 36% of adults with cancer report inactivity. So, can we get our patients to exercise before surgery, and does it help? The ERASE trial1 assessed the effects of exercise on cardiorespiratory fitness and biochemical progression in men with localized prostate cancer undergoing active surveillance. In this trial, 52 male patients were randomized to either the high intensity interval training (n = 26) or usual care (n = 26) groups. Men in the intervention arm had improvements in cardiopulmonary fitness, as well as decreased PSA level, PSA velocity, and LNCaP cell growth:
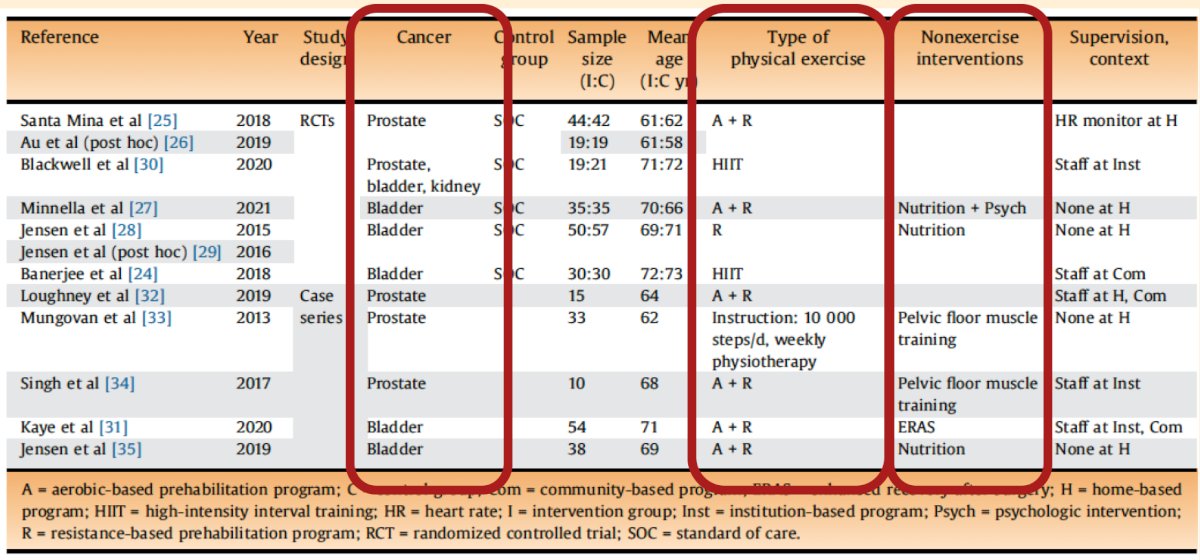
In 2022, Dr. Psutka’s group performed a systematic review of the literature assessing prehabilitation.2 Among 10 unique studies and 2 associated post hoc analyses, they found that prehabilitation studies were safe, patients were able to successfully complete exercise, an intervention was feasible in presurgical populations, there was quality of life benefits, and there were improvement physical function parameters:
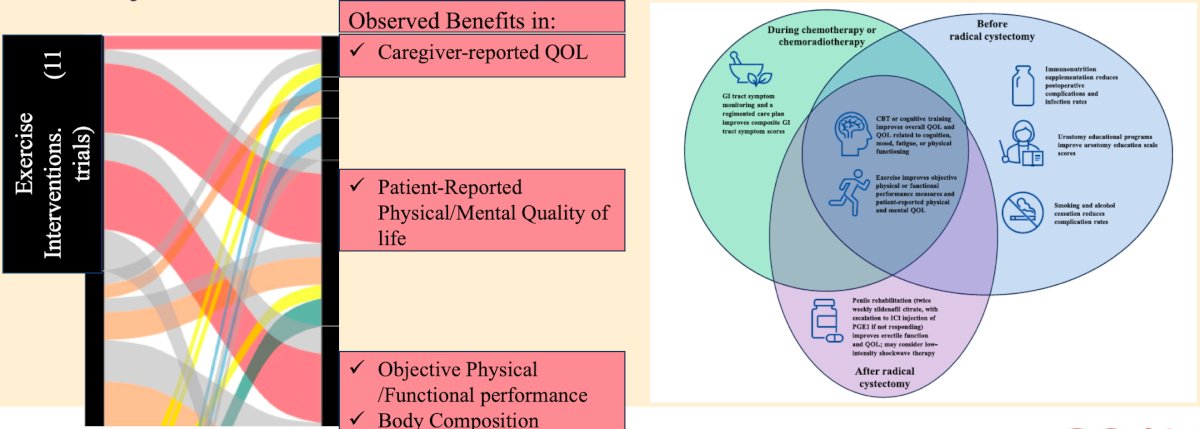
In an updated 2025 review from her group,3 there were 24 unique randomized clinical trials with 2,471 enrolled participants. Among these trials, 9 of 11 trials demonstrated statistically significant benefits with exercise interventions in the domains of caregiver-reported quality of life, patient-reported physical and mental domains of quality of life, and objective or functional assessments of physical performance:
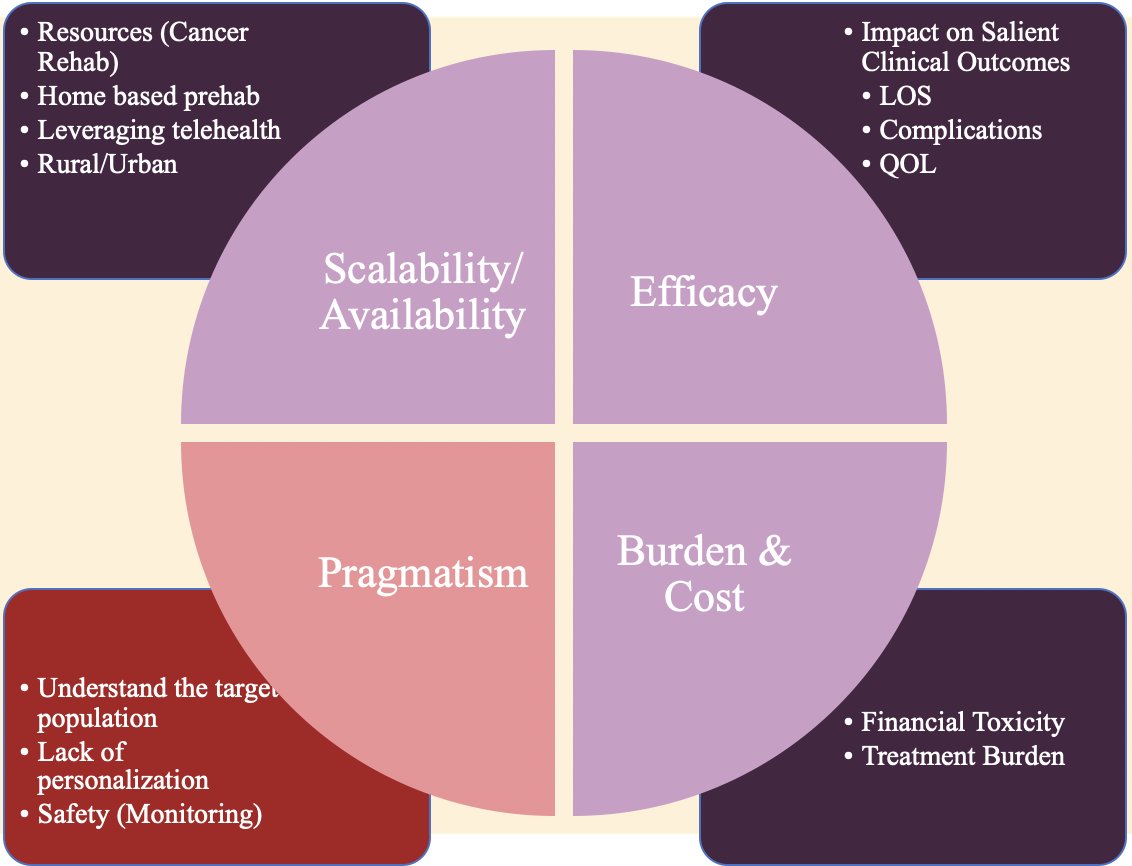
As part of their work, Dr. Psutka’s group has identified several early knowledge gaps in prehabilitation exercise science, namely scalability/availability, efficacy, pragmatism, and burden/cost:2
What are the barriers to exercise for patients with cancer and/or a major illness? This may include (i) a lack of exercise-related instruction from providers, (ii) a lack of exercise facilities, (iii) poor physical responsibilities, (iv) poor physical capacity, (v) treatment related debilitation, (vi) health conditions and comorbidities, and (vii) poor mental health. Several facilitators of exercise include:
- A holistic health care plan
- Professional and social support and encouragement
- Acknowledgement of health benefits
- Belief that exercise could influence the disease course
- Exercise type and guidance
- Communication channels
- Upcoming health care visits
For implementing a pragmatic prehabilitation program, Dr. Psutka uses the “P’s” of prehabilitation: personalized, pragmatic, preparation, and pacing. Regarding personalization, Dr. Psutka notes the importance of personalized exercise prescriptions, clearly delineating the kind of exercises, how often they should be done (frequency), how much should be done (dose), and the side effects to be aware of. The kinds of exercises used should feature general conditioning (ie. aerobic activity, resistance training, balance, flexibility) and impairment-specific strength training. The key is to learn exercises before experiencing post-operative pain and learning how to do these exercises safely. For pacing, patients need to be ‘energy-wise’, with the goal of low intensity interval training. Patients need to be able to do conditioning exercises on both good days and bad days.
As we look toward the future, Dr. Psutka emphasized that it is important to leverage technology to deliver prehabilitation. In a 2017 survey, 20% of urology patients owned an activity tracker, and 82% would be willing to use one to support their health and recovery. Additionally, there are opportunities to leverage artificial intelligence in how we deliver prehabilitation:
At the University of Washington, Dr. Psutka notes that they are running the “GetMoving Trial”, a phase I/II randomized controlled trial of home-based (p)rehabilitation ((P)REHAB) with ExerciseRx in patients with localized urothelial cancer undergoing surgery. The trial schema, interventions, and outcomes are listed as follows:

This trial is utilizing the ExerciseRx patient app at the University of Washington, which is informed by qualitative analysis of interviews with patient advocates, is directly integrated into the electronic medical record provider dashboard, and has novel sensing technology for home (p)rehabilitation.
Dr. Psutka’s opinion is that prehabilitation can be helpful for all patients, not just older patients, not just before surgery, not just for those who demonstrate frailty at baseline, and not just for patients with cancer. Her approach is that everyone gets some prehabilitation, which allows for patient engagement, reassigns the locus of control, and provides a positive focus. At the Fred Hutch Cancer Center, they are starting the EMPOWER trial, a phase II randomized controlled clinical trial evaluating a scalable, personalized home-based activity intervention with ExerciseRx in survivors with non muscle invasive bladder cancer.
Dr. Psutka concluded her presentation by discussing the impact of exercise, personalized programs, and digital devices on prehabilitation with the following take home points:
- Exercise is medicine: patients should exercise in preparation for surgery, as well as throughout their cancer care
- Make it personal: an exercise prehabilitation program must be pragmatic
- Leveraging technology: a program must be home-based, protect privacy, facilitate interaction with providers, be cost effective, and be modifiable
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain between March 21st and 24th 2025
Related content: Prehabilitation in Cancer Care: Personalized Exercise Programs for Better Outcomes - Sarah Psutka
References:
- Kang DW, Fairey AS, Boule NG, et al. Effects of Exercise on Cardiorespiratory Fitness and Biochemical Progression in Men with Localized Prostate Cancer Under Active Surveillance: The ERASE Randomized Clinical Trial. JAMA Oncol. 2021 Oct 1;7(10):1487-1495.
- Briggs LG, Reitblat C, Bain PA, et al. Prehabilitation exercise before urologic cancer surgery: A systematic and interdisciplinary review. Eur Urol. 2022 Feb;81(2):157-167.
- Briggs LG, Parke SC, Beck KL, et al. Prehabilitative/rehabilitative exercise, nutrition, and psychological support for bladder cancer: A scoping review of randomized clinical trials. Cancer. 2025 Jan 1;131(1):e35608.