(UroToday.com) The 2025 EAU annual meeting featured a game changer session and a presentation by Dr. Fred Saad discussing PSA response with darolutamide plus ADT in patients with metastatic hormone sensitive prostate cancer (mHSPC) in ARANOTE. In this phase 3 study, darolutamide + ADT reduced the risk of radiological progression or death by 46% (HR 0.54, 95% CI 0.41-0.71; p < 0.0001) versus placebo + ADT in patients with mHSPC.1 Notably, the incidence of treatment emergent adverse events was low and similar between the groups. Patients achieving an undetectable PSA (< 0.2 ng/mL) at any time had a better ECOG performance status, lower Gleason score, and lower baseline PSA values versus those who did not. At the EAU 2025 annual meeting, Dr. Saad and colleagues reported post-hoc analyses of ARANOTE correlating PSA response with outcomes overall and by baseline PSA level.
In this analysis, darolutamide resulted in a deep PSA response, with three times as many patients achieving an undetectable PSA (< 0.2 ng/mL) at any time versus those on placebo:

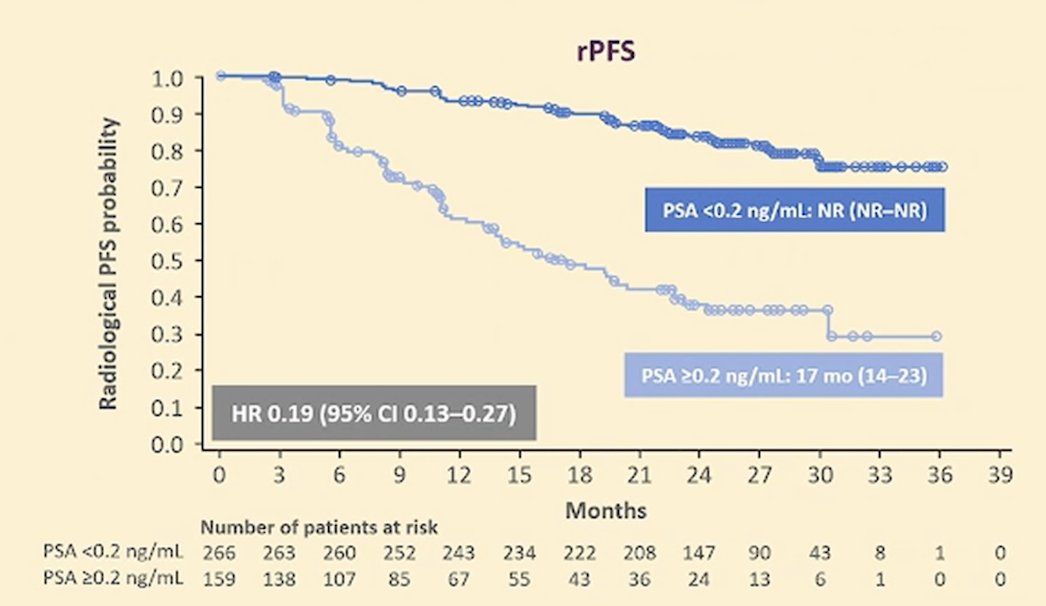
Additionally, patients on darolutamide who achieved an undetectable PSA had a lower risk of radiological progression or death compared to patients on darolutamide who did not achieve an undetectable PSA (HR 0.19, 95% CI 0.13-0.27):
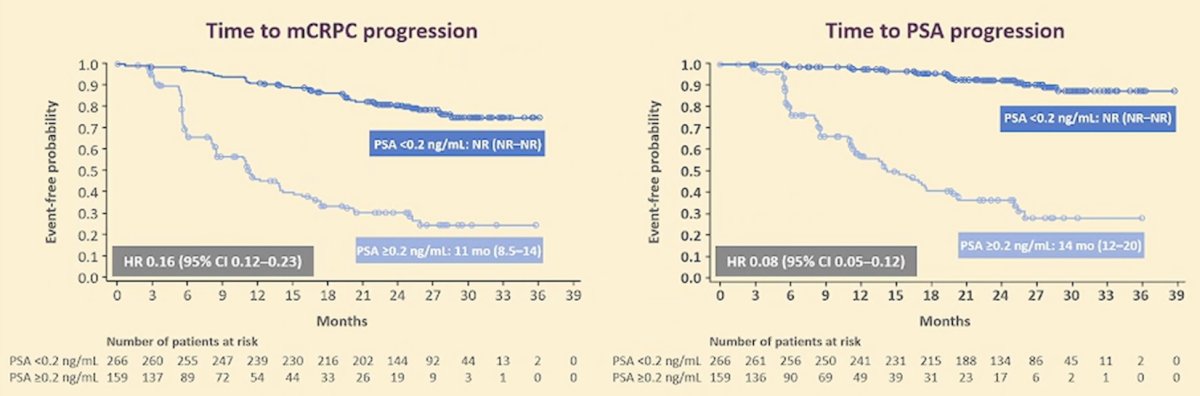
Patients on darolutamide who achieved an undetectable PSA also had a longer time to mCRPC (HR 0.16, 95% CI 0.12-0.23) and PSA progression (HR 0.08, 95% CI 0.05-0.12) compared to patients on darolutamide who did not achieve an undetectable PSA:
With regards to volume of disease, a higher proportion of patients achieved an undetectable PSA with darolutamide versus placebo in both the high volume and low volume subgroups (24 weeks, 36 weeks, 48 weeks, and any time):

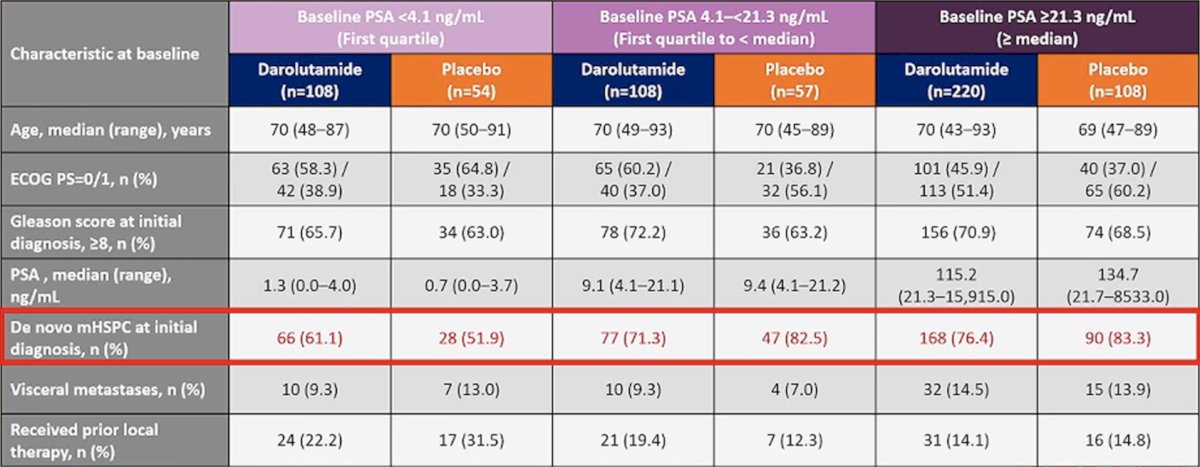
Of all randomized patients, the median baseline PSA was 21 ng/mL, which is much higher than previous androgen receptor pathway inhibitor + ADT trials in mHSPC. Of note, fewer patients with baseline PSA <4.1 ng/mL had de novo disease versus groups with baseline PSA >= 4.1 ng/mL:
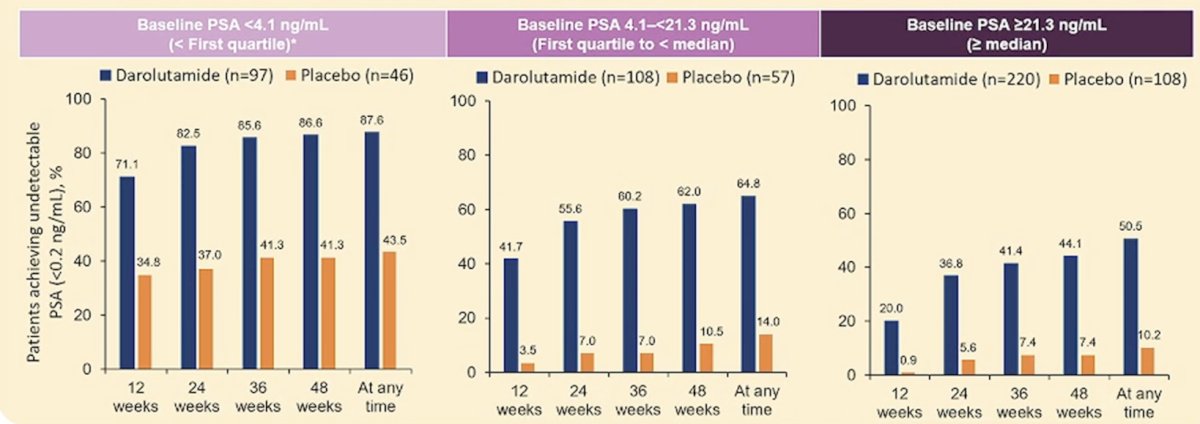
Regardless of baseline PSA, more patients on darolutamide versus placebo achieved an undetectable PSA at any time, with a greater proportion of patients with low baseline PSA achieving an undetectable PSA at any time (87.6% versus 43.5%):
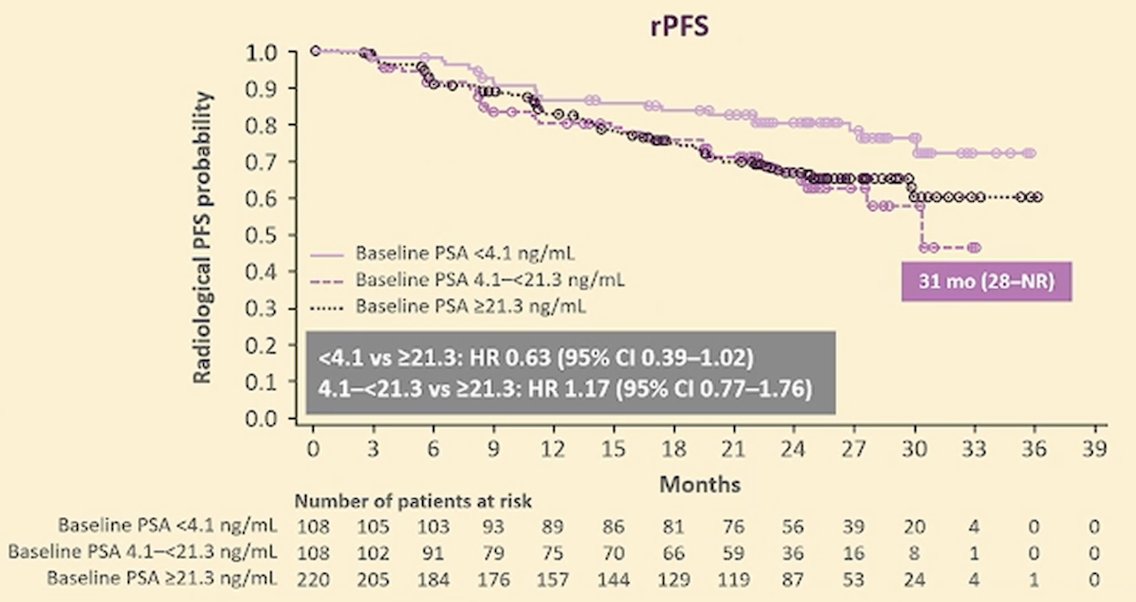
Patients on darolutamide with low baseline PSA (<4.1 ng/mL) had a lower risk of radiological progression or death versus patients with baseline PSA >= 21.3 ng/mL (HR 0.63, 95% CI 0.39-1.02):
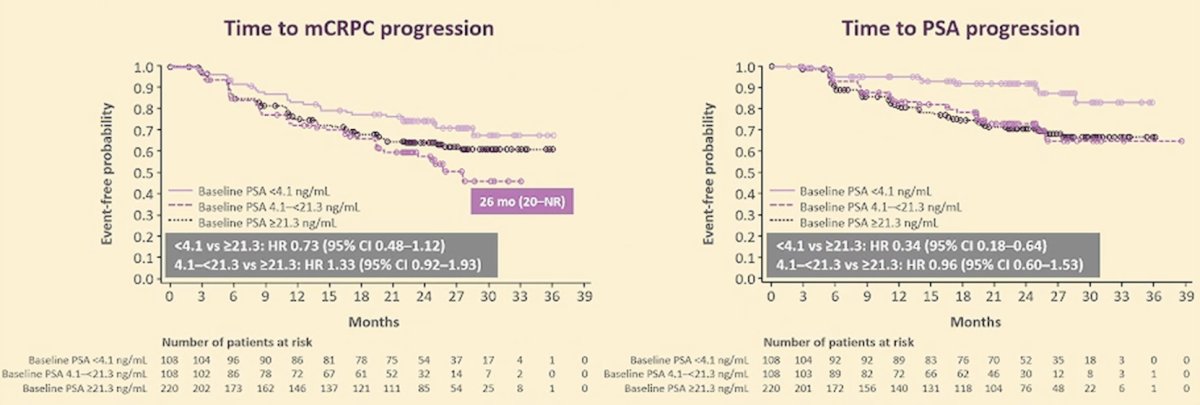
Additionally, patients on darolutamide with a low baseline PSA (<4.1 ng/mL) had a longer time to mCRPC (HR 0.73, 95% CI 0.48-1.12) and time to PSA progression (HR 0.34, 95% CI 0.18-0.64) versus patients with a baseline PSA >= 21.3 ng/mL:
Finally, the favorable safety profile of darolutamide was independent of baseline PSA:

Dr. Saad concluded his presentation by discussing PSA response with darolutamide plus ADT in patients with mHSPC in ARANOTE with the following take home points:
- Darolutamide provided deep and durable responses in the overall population and across baseline PSA subgroups
- Three times as many patients reached an undetectable PSA (< 0.2 ng/mL) versus the placebo arm
- Undetectable PSA was achieved in a greater proportion of patients regardless of baseline PSA
- Undetectable PSA with darolutamide correlated with clinical benefit in terms of radiological progression or death and longer time to mCRPC and PSA progression
- The safety profile of darolutamide was consistent across subgroups, regardless of PSA response and baseline PSA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain between March 21st and 24th 2025
Related content: PSA Responses with Darolutamide Plus ADT in the ARANOTE Trial - Fred Saad
References: