(UroToday.com) The 2025 European Association of Urology (EAU) Annual Congress held in Madrid, Spain between March 21st and 24th 2025, was host to an ‘Advanced Prostate Cancer Consensus Conference (APCCC) Meets EAU’ thematic session. Drs. Karim Fizazi and Bertrand Tombal discussed the pros and cons of de-escalation of systemic therapy in metastatic hormone-sensitive prostate cancer (mHSPC) patients with a deep response to androgen deprivation therapy (ADT) plus an androgen receptor pathway inhibitor (ARPI).
Dr. Peter Ka-Fung Chiu began the session with a case presentation of a 76-year-old male with a past medical history of hypertension and a minor stroke, with full functional recovery thereafter (ECOG performance status 1). He was found to have a serum PSA level of 3,987 ng/ml, and a prostate biopsy demonstrated Grade Group 5 prostatic adenocarcinoma in 10/12 cores. A bone scan demonstrated extensive bone lesions with ‘superscan’ findings: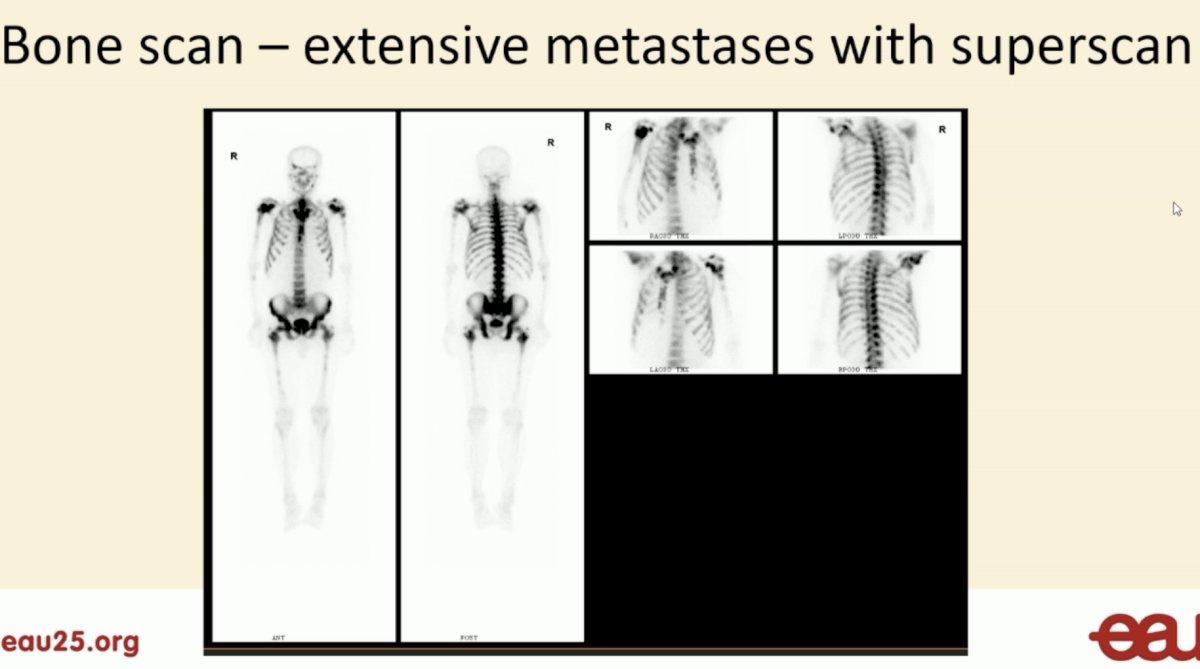
An 18F-PSMA PET/CT demonstrated evidence of extraprostatic extension, bilateral seminal vesicle involvement, and lymph node metastases (bilateral common iliac and para-aotric). He also had evidence of extensive bone metastases involving the:
- Skull base
- Bilateral humeri, clavicles, scapulae, and femurs
- Sternum
- Multiple ribs bilaterally
- All spinal levels
- Pelvis
He was started on doublet therapy with an LHRH agonist + abiraterone acetate/prednisolone with the following PSA response: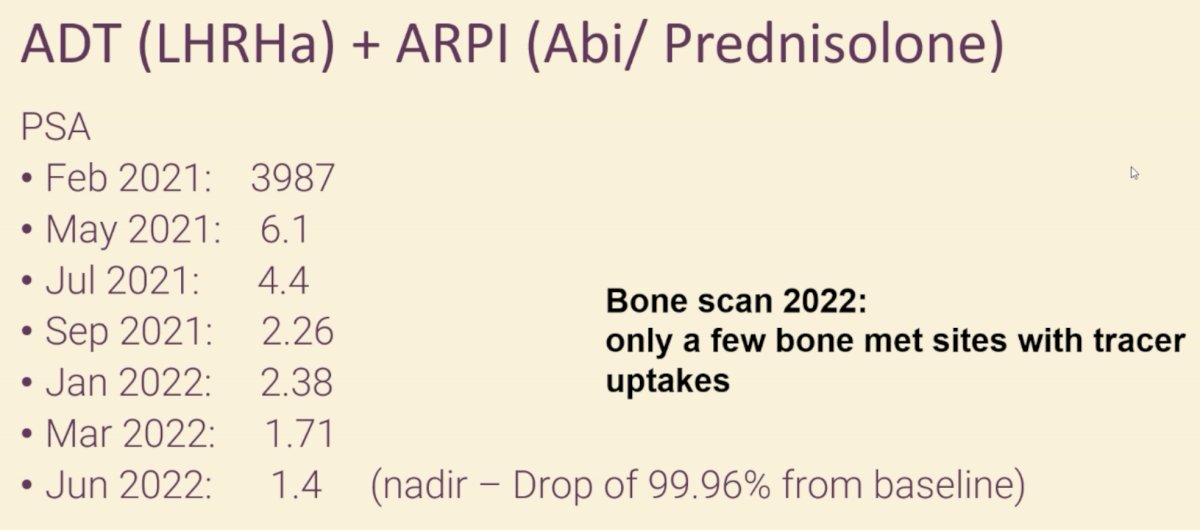
A subsequent bone scan in 2022 demonstrated only a few bone metastatic sites with tracer uptake. Is this patient a candidate for treatment de-escalation or should he be recommended for continued doublet therapy?
Dr. Karim Fizazi argued against treatment de-intensification in this patient. He noted that the historical standard for the treatment of conventional imaging-defined M1 patients has been life-long systemic treatment, which consisted of ADT alone. ADT has been shown to improve overall survival, although side effects remain a concern. Can we stop ADT in M1 patients and restart it when needed (i.e., intermittent ADT)?
One of the main arguments again treatment de-intensification and intermittent therapy is the oncogenic addiction of mCSPC to the androgen receptor. In other words, the vast majority of mCSPC cases are exquisitely hormone sensitive. And, thus, to maximize tumor lethality and patient survival, the androgen axis needs to be strongly targeted for a very long period. Dr. Fizazi noted that ‘in oncology, hitting the key cancer driver strongly and for a long period typically works’.
The Hussain SWOG non-inferiority phase III trial of continuous versus intermittent ADT randomized 1,535 mCSPC patients with 6 months PSA levels <4 ng/ml on ADT therapy to continuous versus intermittent therapy. This trial included patients with either de novo or recurrent M1 disease. At a median follow-up of 9.8 years, this trial failed to demonstrate that intermittent ADT was non-inferior to continuous ADT (median survival: 5.8 versus 5.1 years in favor of continuous ADT; HR: 1.10, 90% CI: 0.99–1.23), although there was a minor quality of life benefit with intermittent ADT.1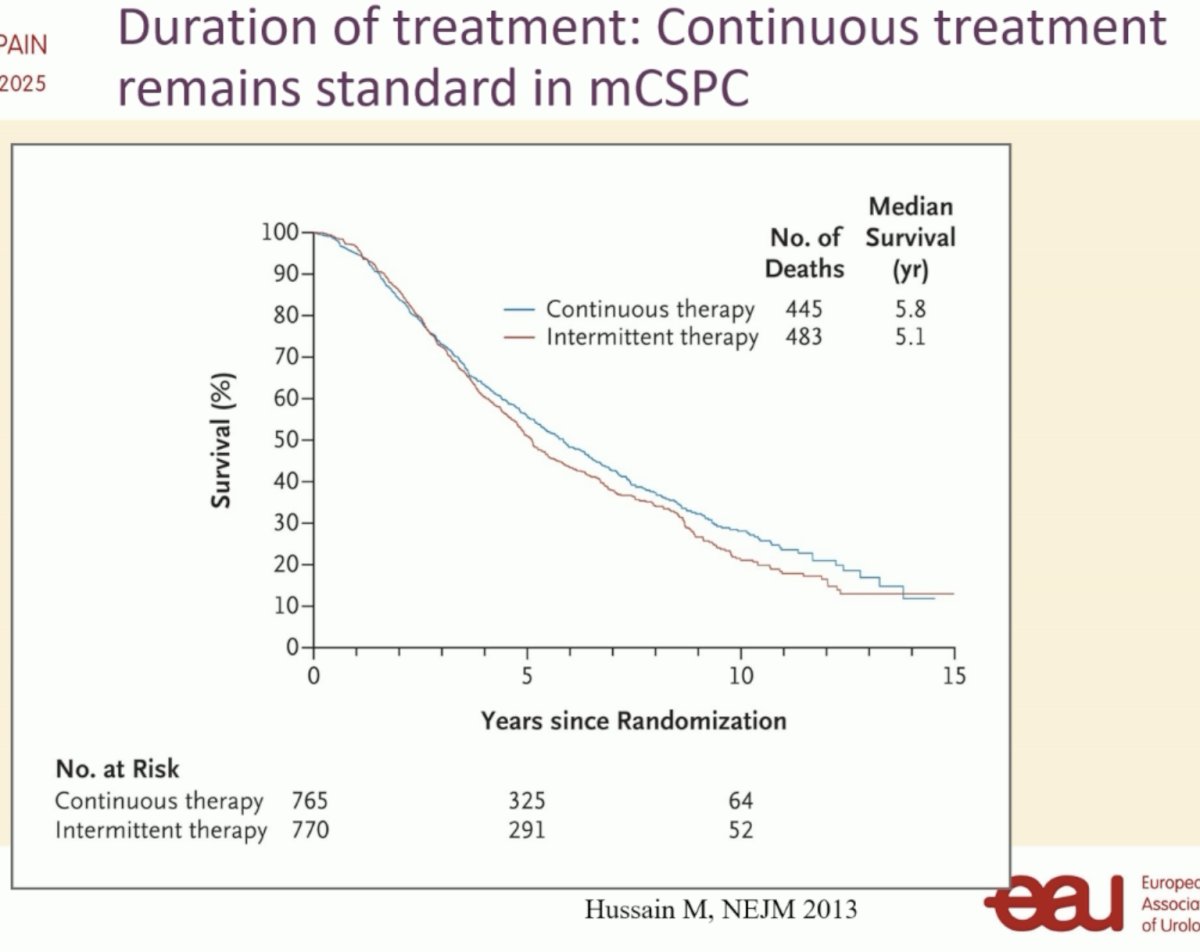
What about patients with a low disease burden? One may assume that these lower risk patients may have more favorable outcomes with intermittent therapy. However, subgroup analysis of the SWOG trial of patients with ‘minimal’ disease (i.e, lymph node only or bone limited to the pelvis/vertebral axis, without visceral metastases) demonstrated that the median survival difference between continuous and intermittent ADT was even larger (6.9 versus 5.4 years). As such, Dr. Fizazi stated that there may be a ‘potential harm of intermittent ADT in M1 patients’.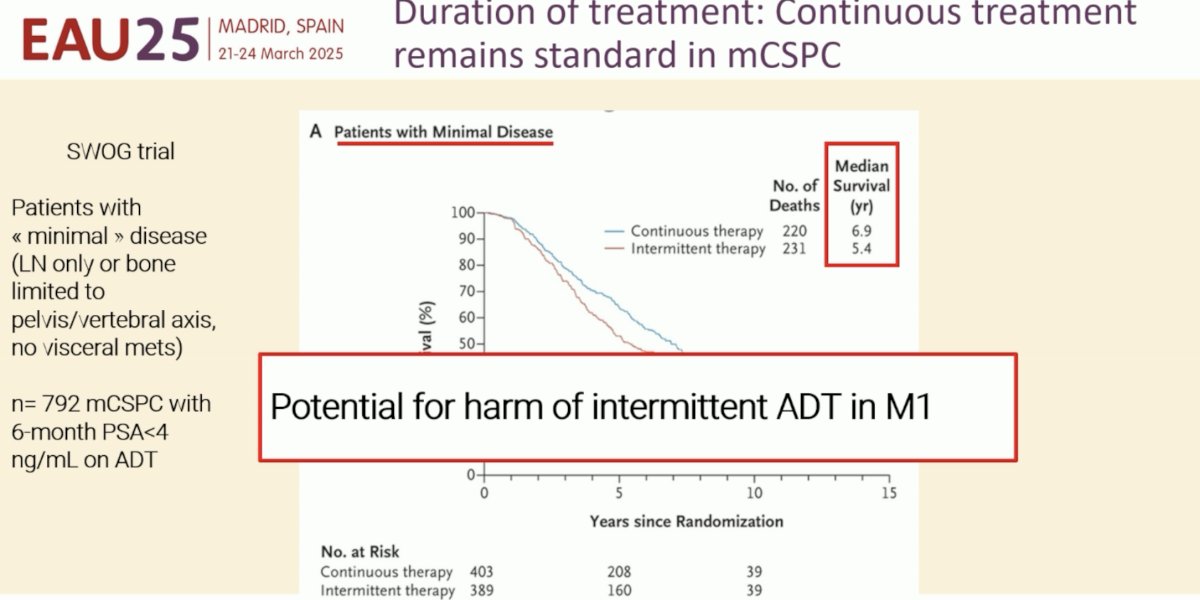
Drawing parallels from the high risk, localized space, longer treatment (e.g., long-term versus short-term ADT with radiotherapy) is associated with superior survival outcomes. This is also likely true in M1 patients.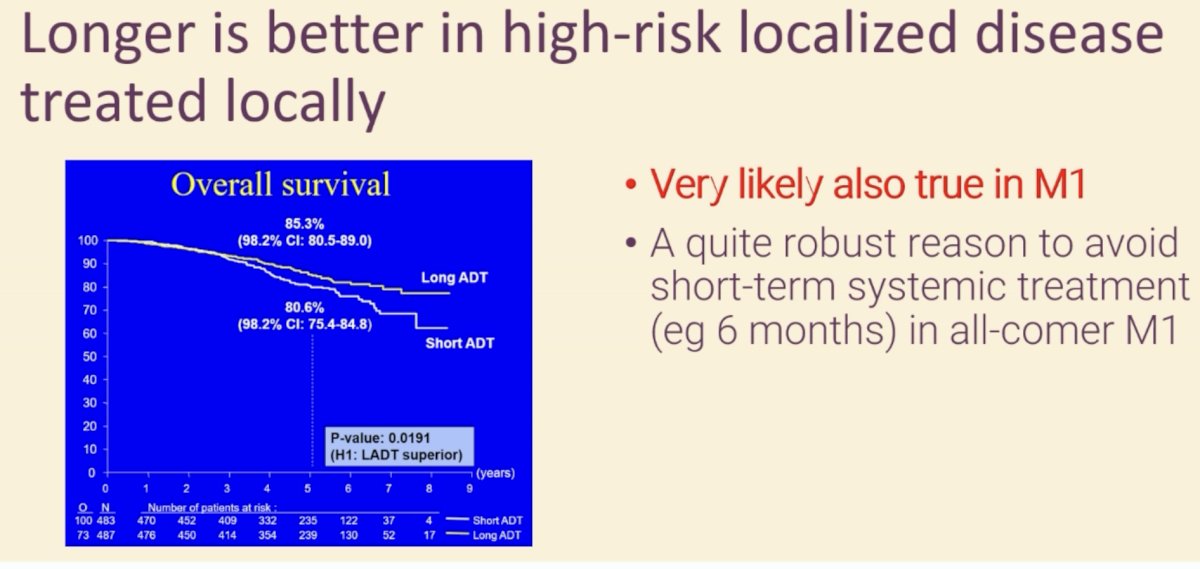
He pointed out that all recent successes in the M1 disease space have been with treatment intensification with doublet and triplet therapy. And, importantly, the majority de novo mCSPC patients die of their prostate cancer. Clearly, there is a need for even more active treatments.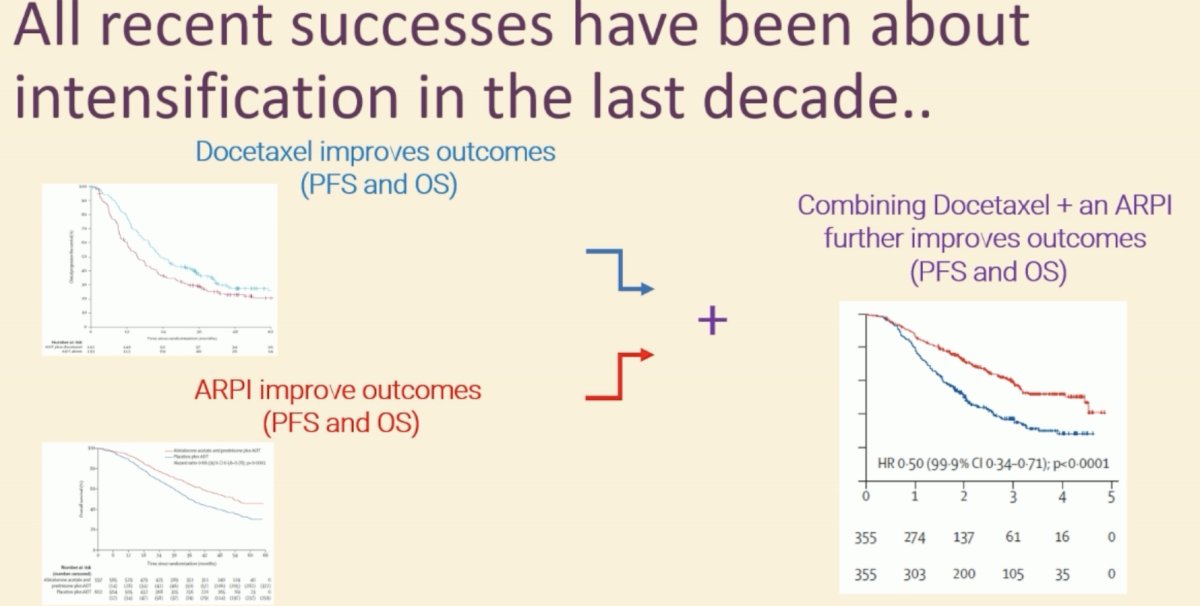
While the historical standard for M1 treatment has long been life-long systemic treatment, does this remain true in the current context of:
- Intensified systemic treatment + radiotherapy of the prostate?
- What about M1 disease identified on PSMA PET, as opposed to conventional imaging?
- Are there differences between recurrent and de novo M1 patients?
- How do we select excellent responders?
Clearly, volume and, most importantly, timing of M1 disease have important prognostic implications. Patients with de novo high-volume disease treated ADT alone have a median overall survival of only 3.6 years. Conversely, those with recurrent low volume disease have a corresponding survival of 7.7 years.3,4 If we account for contemporary systemic therapy options (doublet/triplet), the survival of these recurrent low volume M1 patients may be as high as 10 years. Accordingly, the appropriateness of systemic therapy de-escalation varies by M1 volume and timing.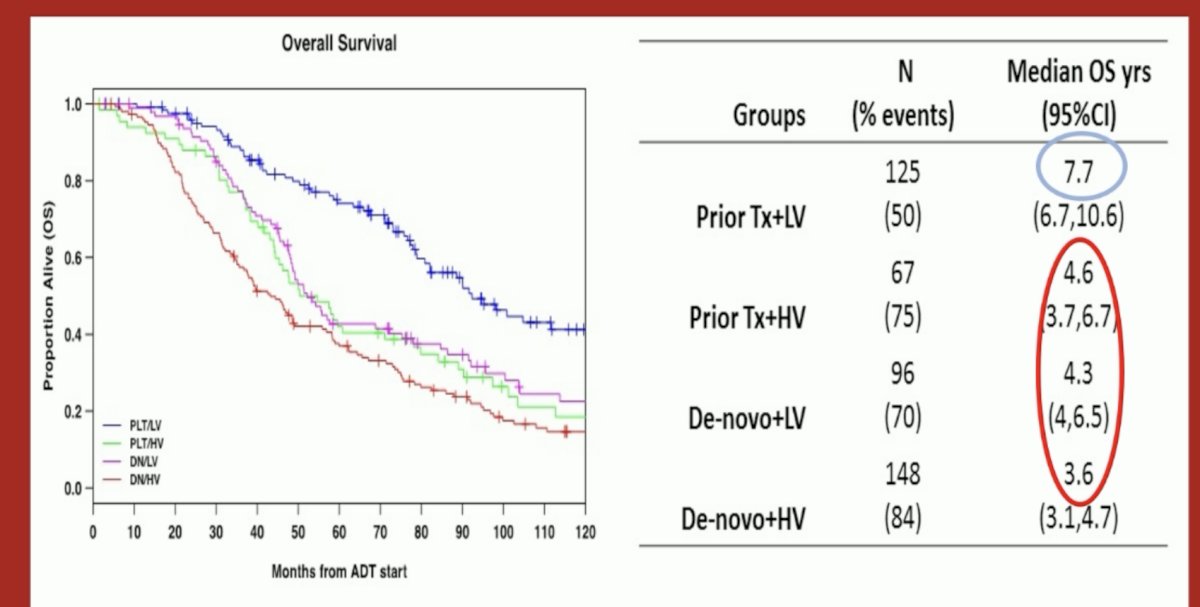
To date, the only reliable biomarker for treatment de-intensification is the serum PSA response. In the PEACE-1 trial, patients who achieved a serum PSA level of ≤0.2 ng/ml following 8 months of standard of care +/- abiraterone acetate/prednisone had superior overall survival outcomes, compared to those with 8 months PSA levels >0.2 ng/ml. As such, given that the patients in the case presentation had a PSA level of 1.4 ng/ml, Dr. Fizazi argued that he is not suitable for treatment de-intensification.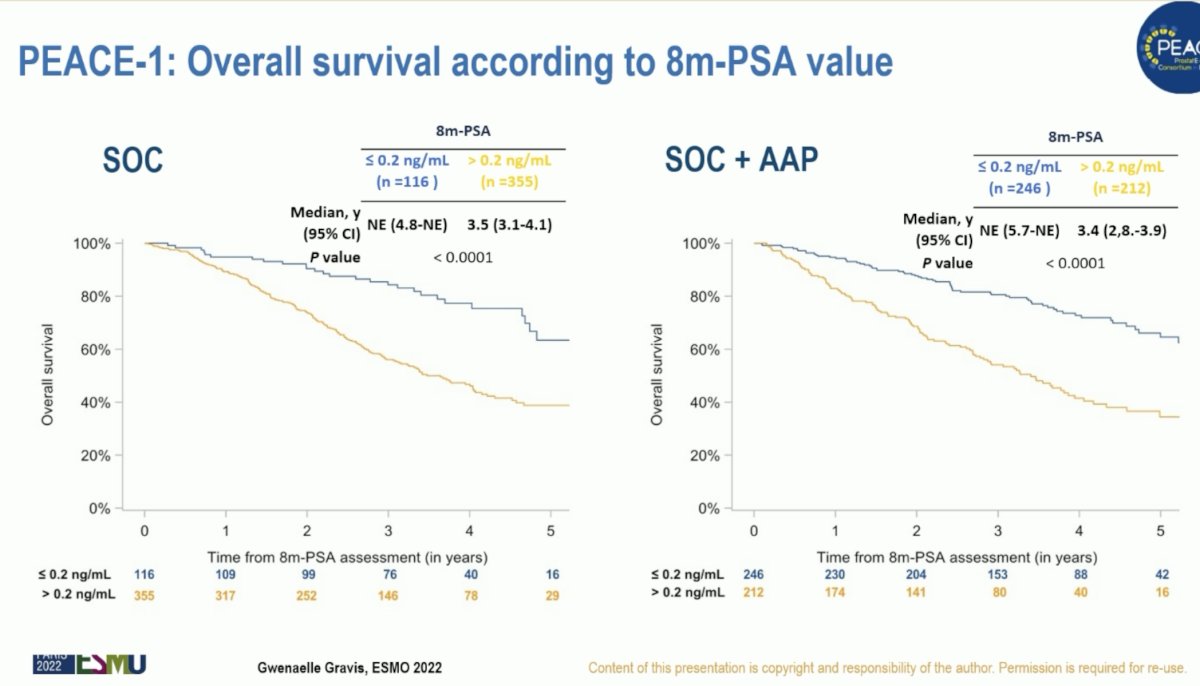
What is the current status of implementing treatment de-intensification in contemporary practice? Long-term follow-up of the GETUG 15 trial demonstrates that only 28% of long-term survivors discontinued ADT, with a median discontinuation period of 6 years, and 60% have not required re-initiation.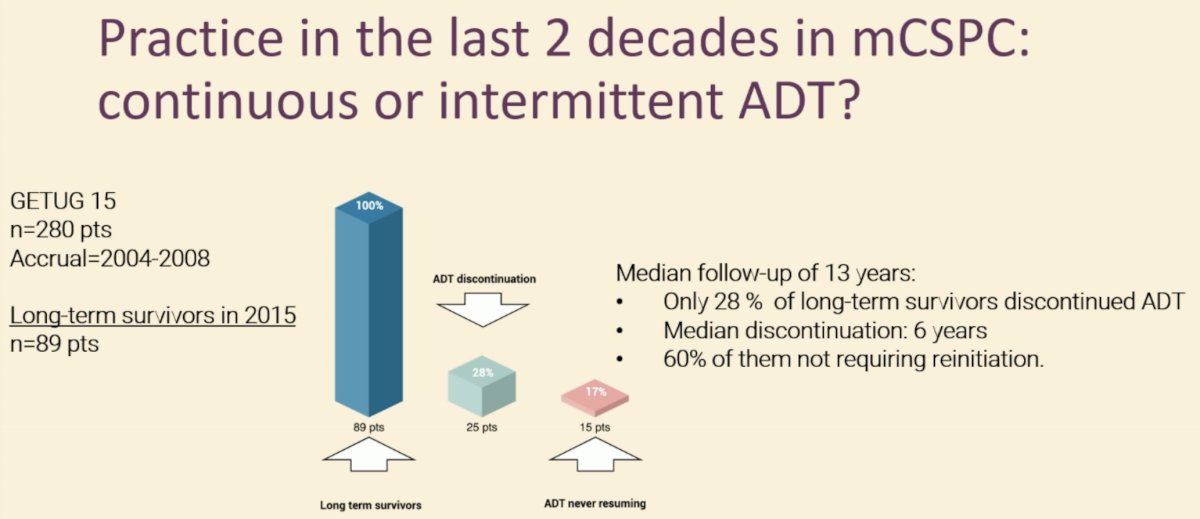
What do the experts say about treatment de-intensification? In an APCCC consensus poll, 47% of respondents stated that they would recommend continuous therapy for the majority of mHSPC patients with a deep remission with systemic therapy (e.g., PSA <0.2 ng/ml) and who do not experience side effects.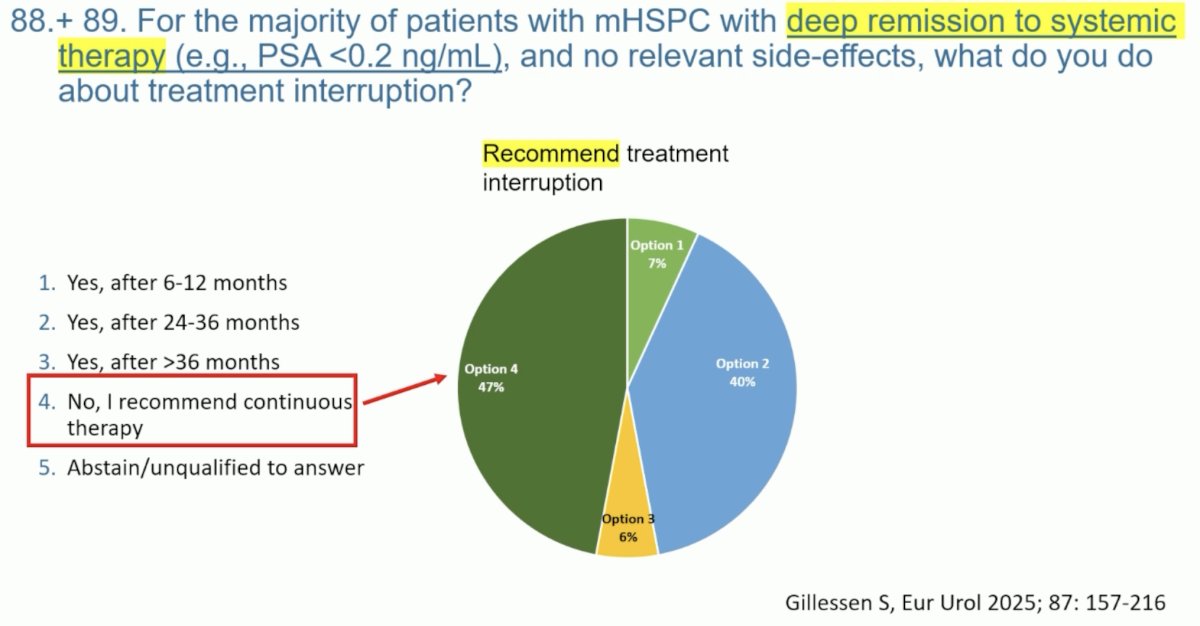
Ongoing trials are incorporating treatment de-intensification strategies for de novo M1 prostate cancer patients with good PSA responses:
Dr. Fizazi concluded his argument against treatment de-intensification as follows:
- The optimal duration of systemic treatment for mCSPC remains unknown
- Stopping should be considered as standard when systemic treatment becomes dangerous (e.g. acute cardiovascular event)
- In other situations, continuous treatment is standard. You may consider intermittent (only) if there are:
- Excellent responses (e.g., PSA <0.2 ng/mL)
- And duration is already ‘reasonable’ (2–3 years?)
- And in an informed and demanding patient
- Please favor participation in trials
- Hopefully biomarkers/AI will help in selection of treatment de-intensification candidates
Dr. Bertrand Tombal began his argument in favor of treatment de-intensification with the following quote from Mark Twain: “Too much of anything is bad”. Because of the nature of the trials, which are event-driven, and the relatively early readings, we know very little about the outcomes of the long-term survivors.
If we look at data from the PEACE-1 trial, ~60% of patients treated with triplet therapy are alive at 7 years.5 These patients are unlikely to die of their disease in the subsequent 1-2 years. As such, why can we not de-intensify treatment in these patients?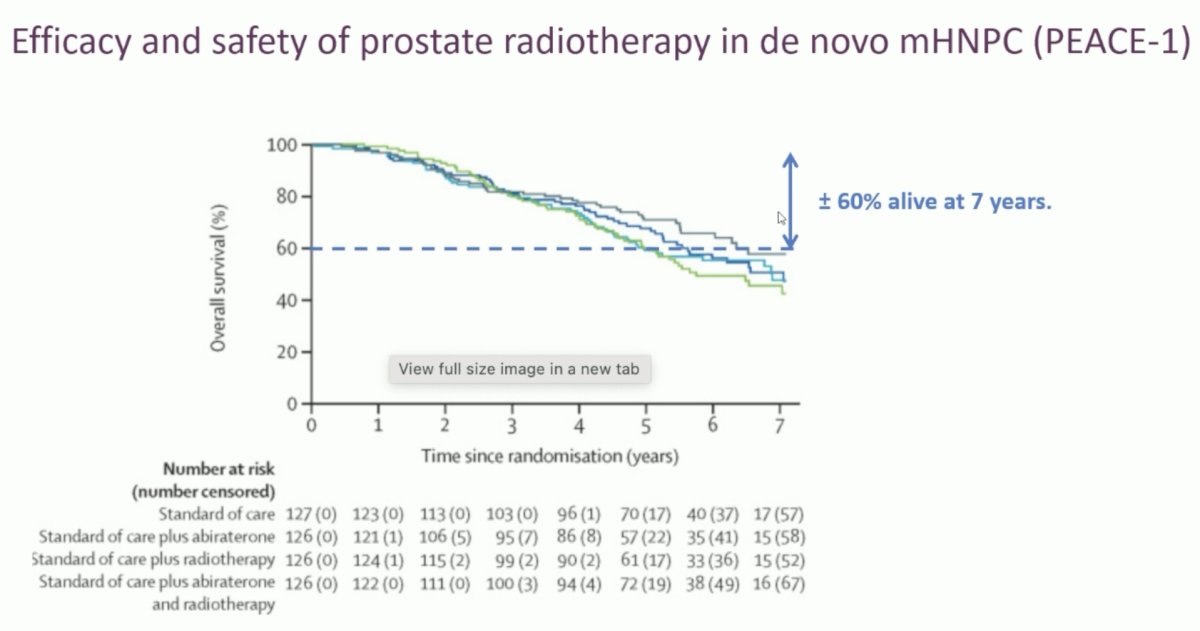
Similarly, in the ARASENS trial, ~70% of patients receiving triplet therapy were alive at 4-5 years and not all of them require life-long therapy.6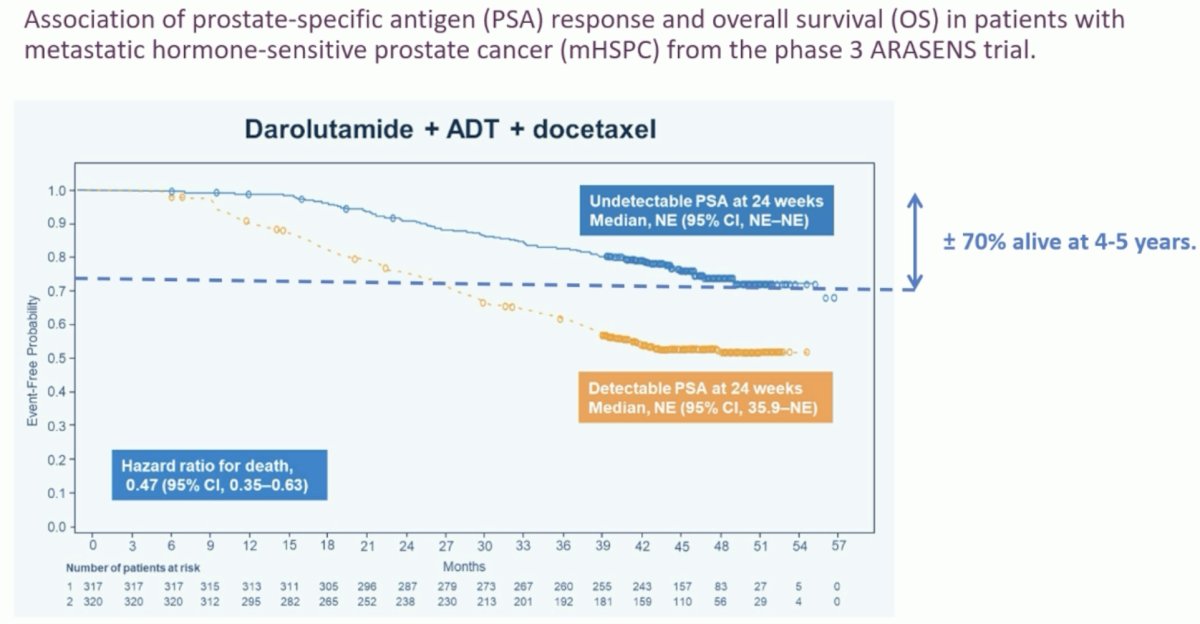
An ad hoc analysis of the TITAN trial of ADT +/- apalutamide for mCSPC patients has demonstrated that deep, rapid, and durable PSA declines with apalutamide + ADT (≥90% decline or PSA ≤0.2 ng/ml at 3 months of apalutamide treatment) are associated with longer survival and improved clinical outcomes.7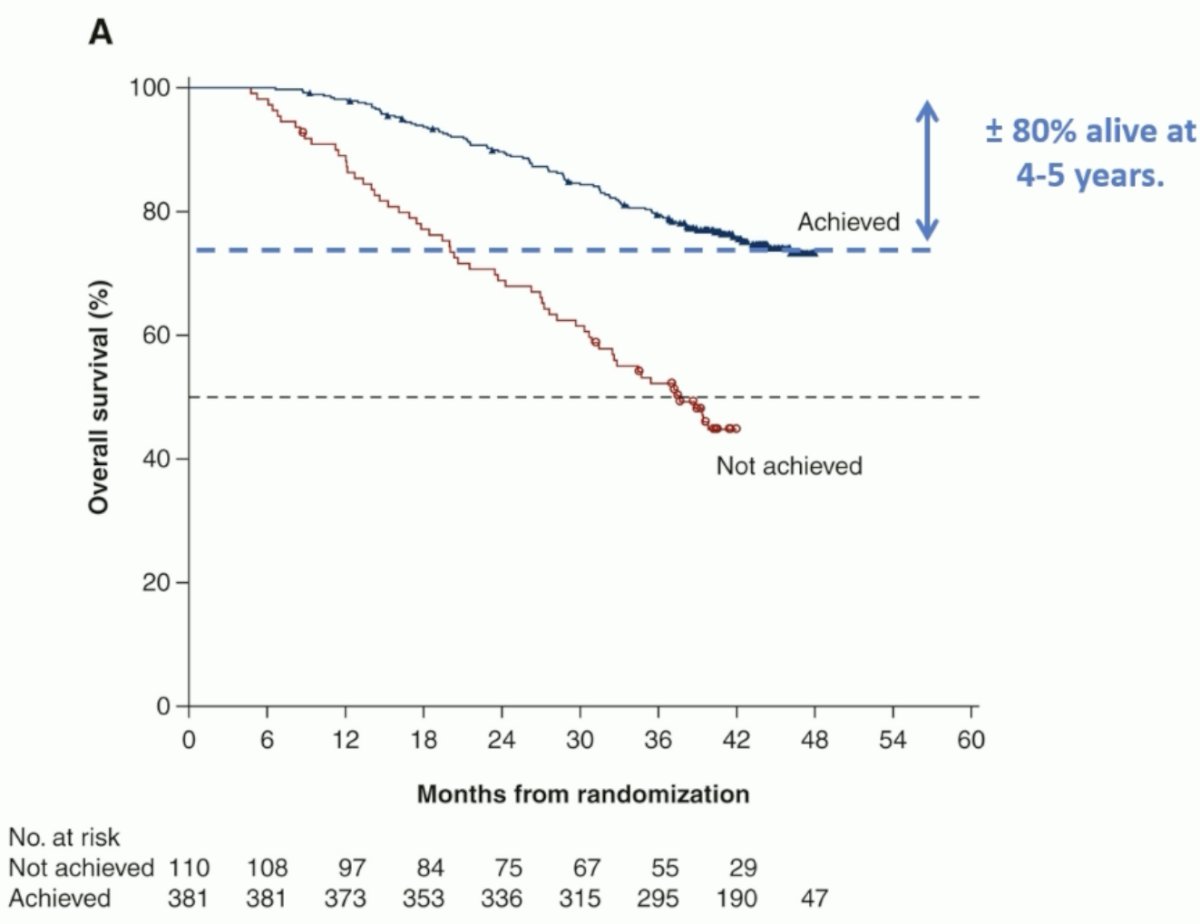
This is particularly relevant as the proportion of patients reaching a ‘low’ PSA level appears to be approximately 60% in mCSPC trials of doublet therapy and superior to those observed with ADT alone.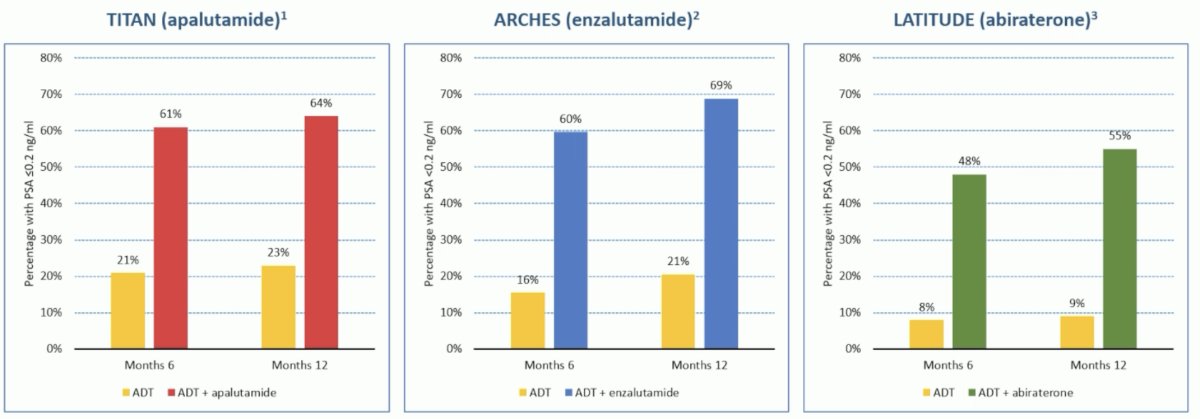
Another issue with continued treatment intensification is that with a longer duration of treatment, there is an increased risk of side effects, some of which have potentially lethal consequences. This has been demonstrated in all trials of doublet therapy, as seen below. Notably, these trials capture adverse events that occur during the study treatment period and for a short interval thereafter. Thus, these trials likely severely underestimate the adverse effect profile of these intensified regimens.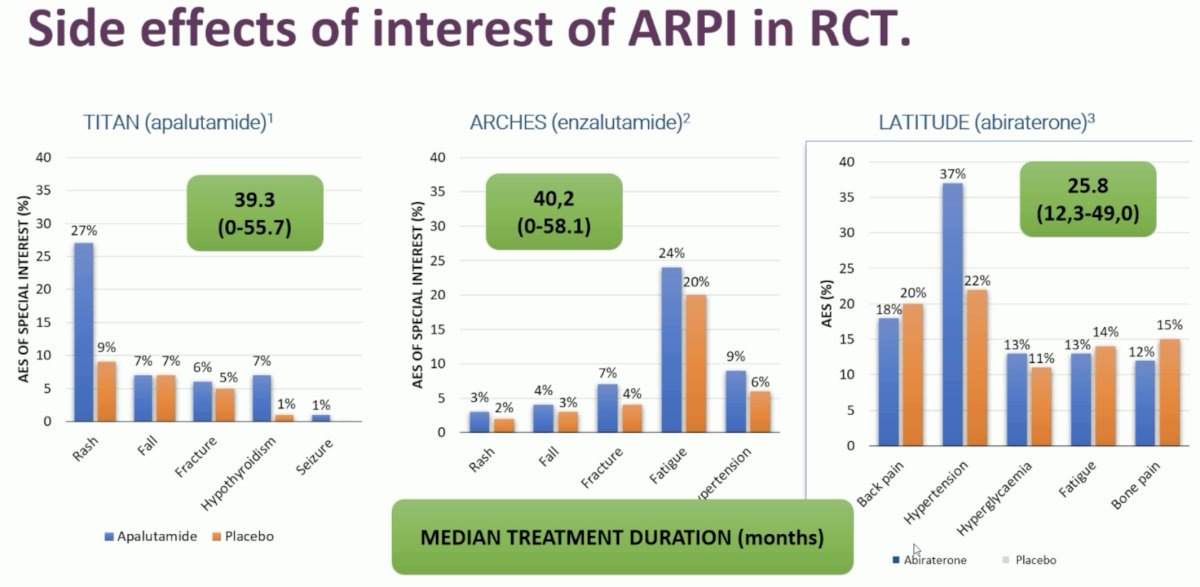
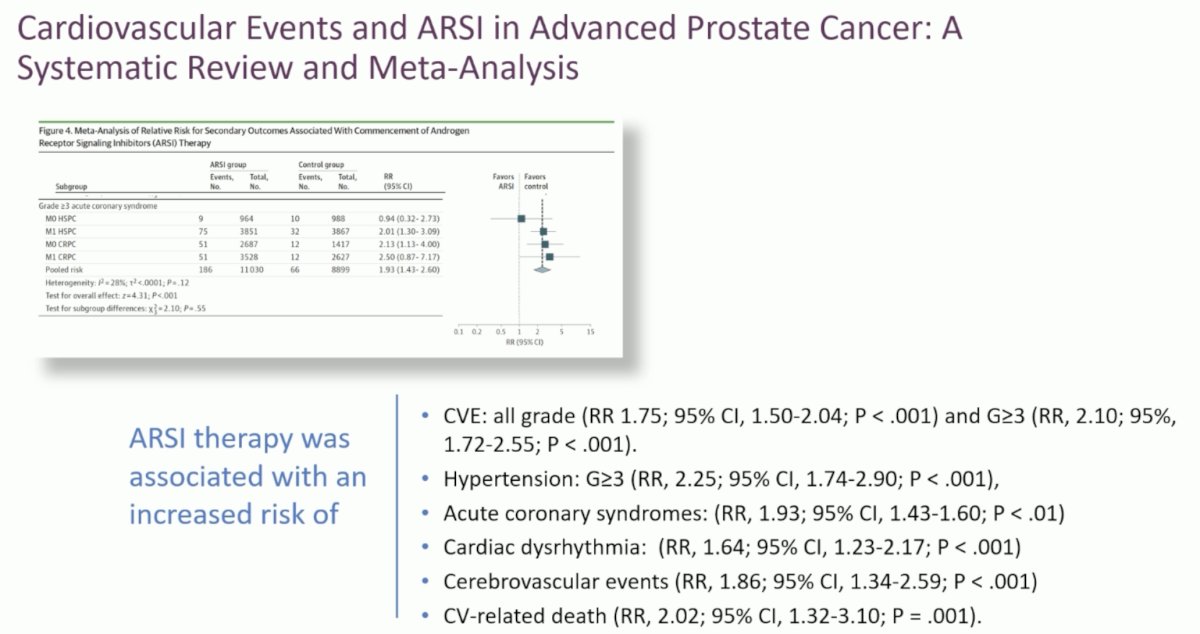
A 2024 systematic review and meta-analysis of pooled cardiovascular events in trials of androgen receptor signaling inhibitors for advanced prostate cancer demonstrated increased risks of:8
- All grade and grade ≥3 cardiovascular events (RRs: 1.75 and 2.1, respectively)
- Grade ≥3 hypertension (RR: 2.25)
- Acute coronary syndrome (RR: 1.93)
- Cardiac dysrhythmia (RR: 1.64)
- Cerebrovascular events (RR: 1.86)
- Cardiovascular-related death (RR: 2.02)
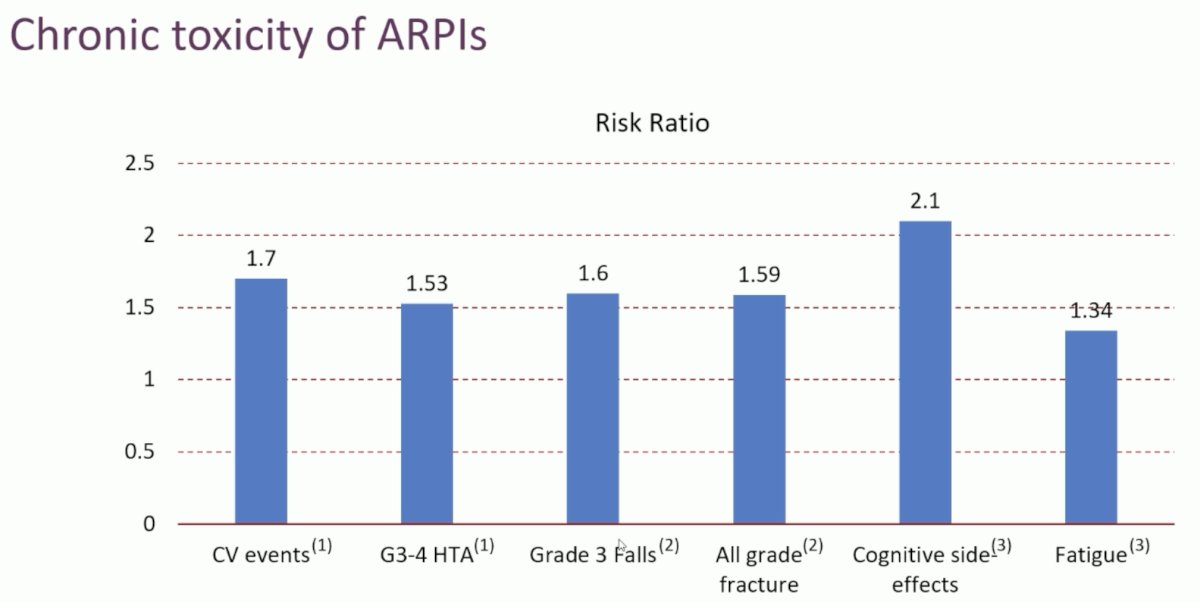
In the real-world, continued systemic therapy intensification is similarly associated with an increased risk of adverse events:

The concern here is that, in the long-term, the consequence of the side effects of continued systemic therapy intensification may outweigh its oncological benefits. When considering the final overall survival benefit, we need to weigh the patient’s comorbidities, amplitude of response, the cancer characteristics, and the efficacy of treatment.
In an individual patient data meta-analysis of five ARSI trials (LATITUDE, STAMPEDE A versus G, SWOG 1216, ENZAMET, and STAMPEDE A versus J), Fisher evaluated the effects of ARSIs by age group. Specifically, among patients receiving abiraterone therapy, a net overall survival benefit was observed for patients <75 years of age, but not those ≥75 years, despite the fact that a prostate cancer survival benefit was observed in patients ≥75 years. This net neutral benefit in this older subgroup likely reflects the increased mortality secondary to other causes, namely cardiovascular, in this abiraterone-treated elderly cohort.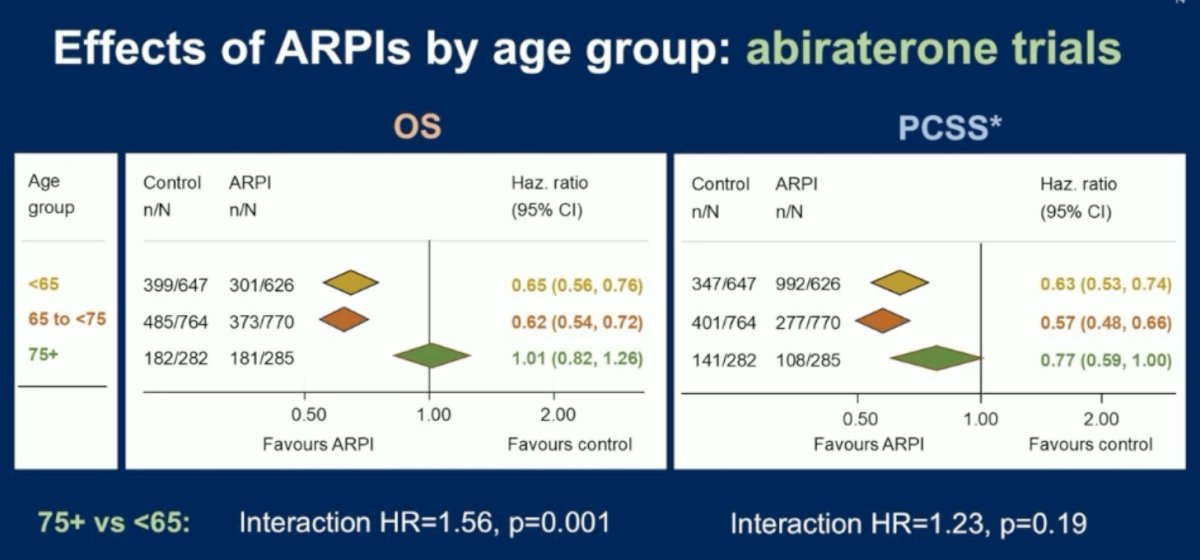
Dr. Tombal concluded as follows:
- A significant proportion of patients achieve a profound PSA response (≤0.2 ng/ml) after treatment with ADT and an ARPI
- Sub-analyses of the registration trials have consistently demonstrated that these patients have prolonged survival and, thus, prolonged exposure to treatment
- There is an opportunity to revisit the concept of intermittent treatment as a strategy to reduce side effects, improve HR-QoL, and limit costs
- This should be tested in clinical trials, properly assessing the risks and benefits of de-escalation
Presented by:
- Karim Fizazi, MD, PhD, Head of the Department of Cancer Medicine, Institute Gustave Roussy (IGR), Villejuif, France, Professor in Oncology, University of Paris, Paris, France
- Bertrand Tombal, MD, PhD, Chairman of the Department of Surgery and Full Professor of Urology at the Université Catholique de Louvain, Ottignies-Louvain-la-Neuve, Belgium
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 European Association of Urology (EAU) Annual Congress held in Madrid, Spain between March 21st and 24th, 2025
References:- Hussain M, Tangen CM, Berry DL, et al. Intermittent versus Continuous Androgen Deprivation in Prostate Cancer. N Engl J Med. 2013; 368: 1314-25.
- Bolla M, de Reijke TM, Van Tienhoven, et al. Duration of Androgen Suppression in the Treatment of Prostate Cancer. N Engl J Med. 2009; 360 :2516-27.
- Francini E, Gray KP, Xie W, et al. Time of metastatic disease presentation and volume of disease are prognostic for metastatic hormone sensitive prostate cancer (mHSPC). Prostate. 2018; 78(12): 889-95.
- Gravis G, Boher JM, Chen YH, et al. Burden of Metastatic Castrate Naive Prostate Cancer Patients, to Identify Men More Likely to Benefit from Early Docetaxel: Further Analyses of CHAARTED and GETUG-AFU15 Studies. Eur Urol. 2018; 73(6): 847-55.
- Fizazi K, Foulon S, Carles J, et al. Abiraterone plus prednisone added to androgen deprivation therapy and docetaxel in de novo metastatic castration-sensitive prostate cancer (PEACE-1): a multicentre, open-label, randomised, phase 3 study with a 2 × 2 factorial design. Lancet. 2022; 399(10336): 1695-707.
- Smith MR, Hussain M, Saad F, et al. Darolutamide and Survival in Metastatic, Hormone-Sensitive Prostate Cancer. N Engl J Med. 2022; 386: 1132-42.
- Chowdhury S, Bjartell A, Agarwal N, et al. Deep, rapid, and durable prostate-specific antigen decline with apalutamide plus androgen deprivation therapy is associated with longer survival and improved clinical outcomes in TITAN patients with metastatic castration-sensitive prostate cancer. Ann Oncol. 2023; 34(5): 477-85.
- El-Taji O, Taktak S, Jones C, et al. Cardiovascular Events and Androgen Receptor Signaling Inhibitors in Advanced Prostate Cancer: A Systematic Review and Meta-Analysis. JAMA Oncol. 2024; 10(7): 874-84.