(UroToday.com) The 2025 European Association of Urology (EAU) Annual Congress held in Madrid, Spain between March 21st and 24th 2025, was host to an ‘Advanced Prostate Cancer Consensus Conference (APCCC) Meets EAU’ thematic session. Drs. Alberto Briganti, Piet Ost, and Ursula Vogl presented the urologist, radiation oncologist, and medical oncologist perspectives on the management of a patient with high-risk, localized Grade Group 5 cT3bN0M0 prostate cancer.
Dr. Peter Ka-Fung Chiu began the session with a case presentation of a 66-year-old male with a past medical history of hypertension who presented with a PSA of 6.9 ng/ml and Prostate Health Index score of 86 (highest risk group). He had an MRI of the prostate performed which demonstrated:
- 40 ml prostate, 16 x 12 mm PIRADS 5 lesion at the right peripheral zone extending from the base to the apex
- Suspicious extraprostatic extension on the right side
- No obvious seminal vesicle invasion
He underwent a targeted + systematic fusion biopsy that demonstrated:
- Target lesion: ISUP Grade Group 5 disease
- Systematic cores:
- All right sided cores: ISUP Grade Group 4 disease
- All left side cores: Negative for malignancy
He underwent a staging 18F-PSMA PET/CT that was suspicious of seminal vesicle invasion. There was no evidence of lymph node enlargement or distant metastases. 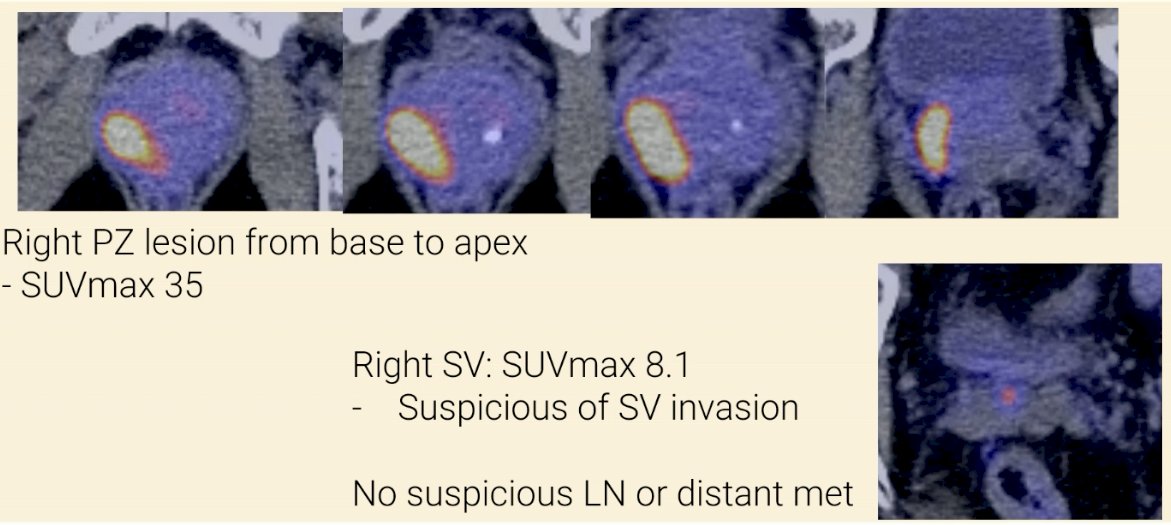
Using the 2023 Briganti nomogram for miN0M0 patients on PSMA PET, this patient was calculated to have a ~15% risk of pathologic lymph node involvement.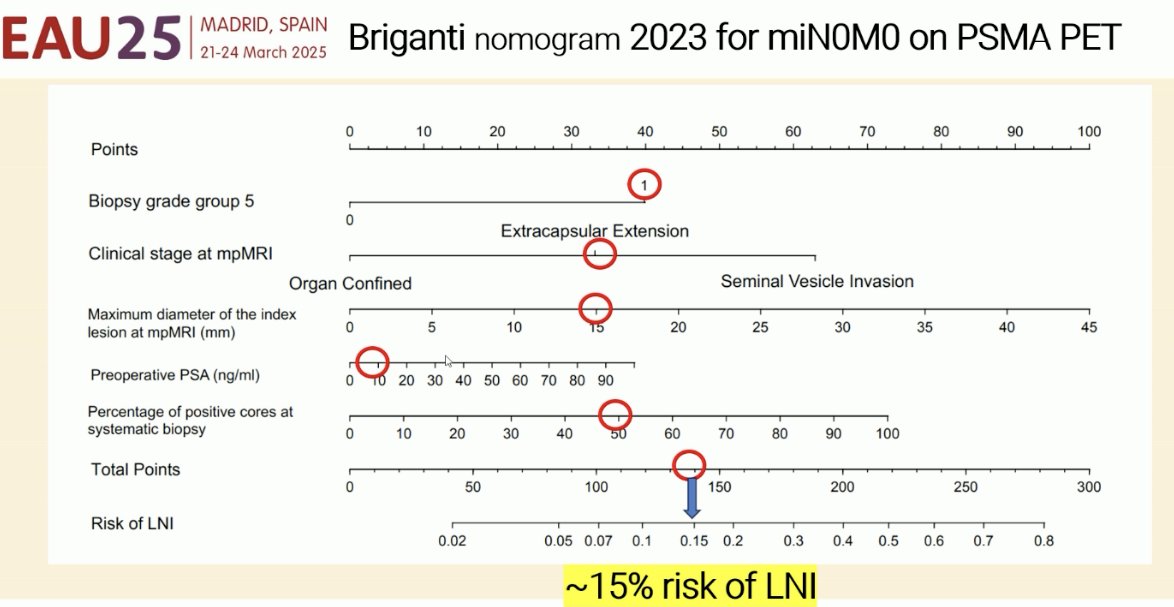
What is the best next step for this 66-year-old, ECOG 0 patient with Grade Group 5 cT3bN0M0 prostate cancer?
- Radical prostatectomy + extended pelvic lymph node dissection (ePLND)
- Radical radiotherapy with neoadjuvant and adjuvant ADT
- Other systemic treatment
Dr. Alberto Briganti began his argument in favor of radical prostatectomy + ePLND by noting that MRI and PSMA PET both have important limitations for the local staging of prostate cancer patients. While these modalities have excellent specificity for confirming the presence of seminal vesicle invasion, their sensitivity is limited even when used in combination: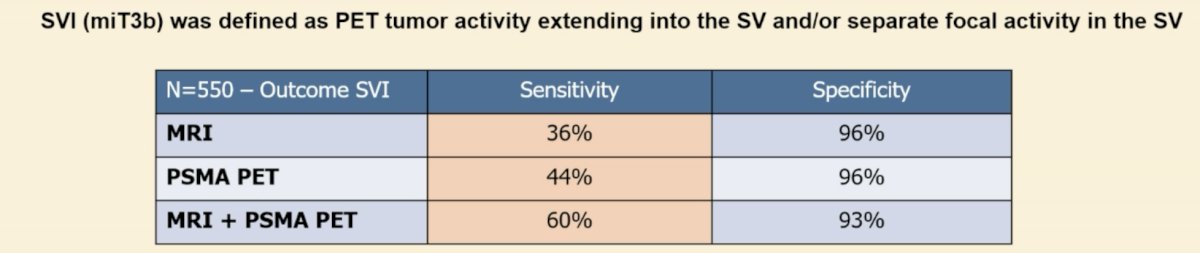
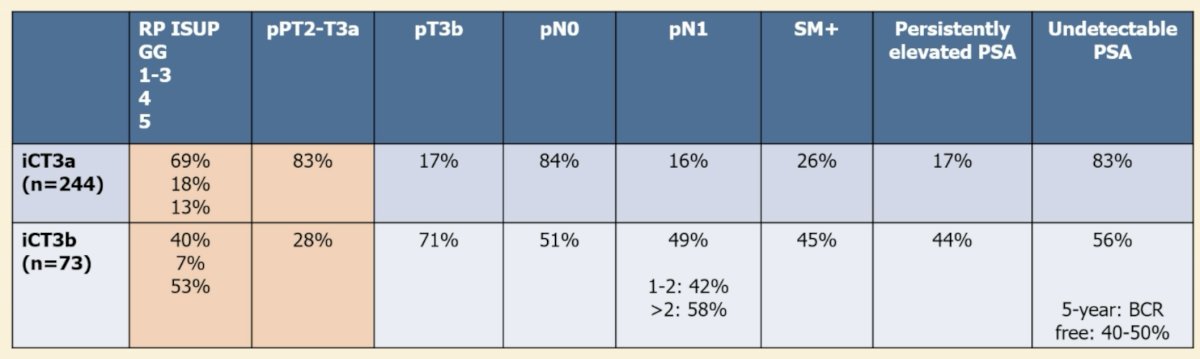
Why does local staging matter in this setting? Patients with evidence of seminal vesicle involvement on imaging (iT3b) have significantly worse prognoses compared to patients with evidence of cT3a disease on imaging (iT3a). The 5-year biochemical recurrence-free survival for iT3b patients is 56%, compared to 71% for iT3a patients (HR: 1.8, p=0.04).1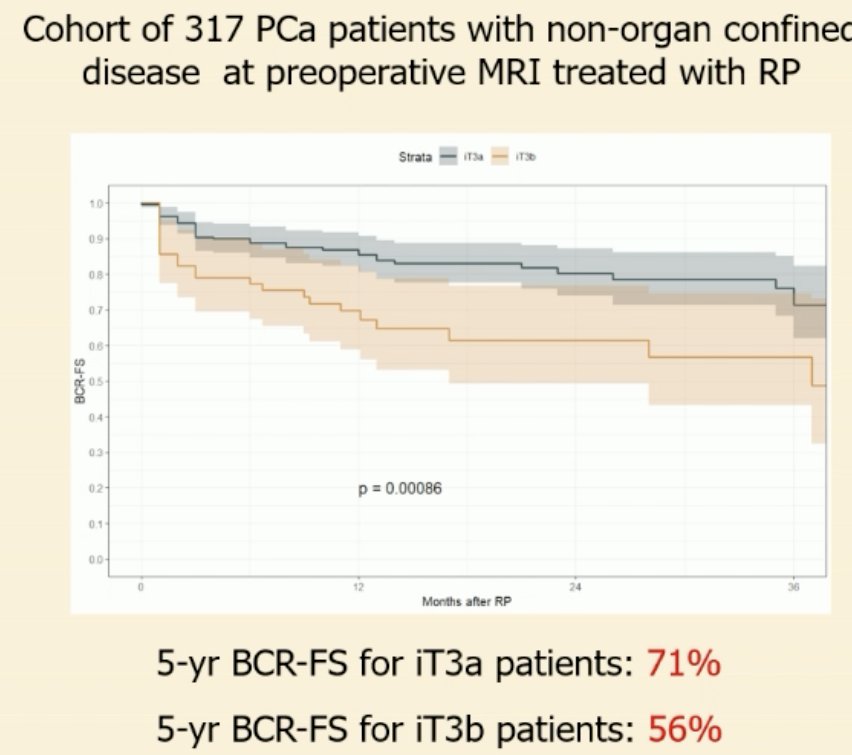
The EAU guidelines currently acknowledge that radical prostatectomy is an option for patients with cN+ disease, as part of multi-modal therapy.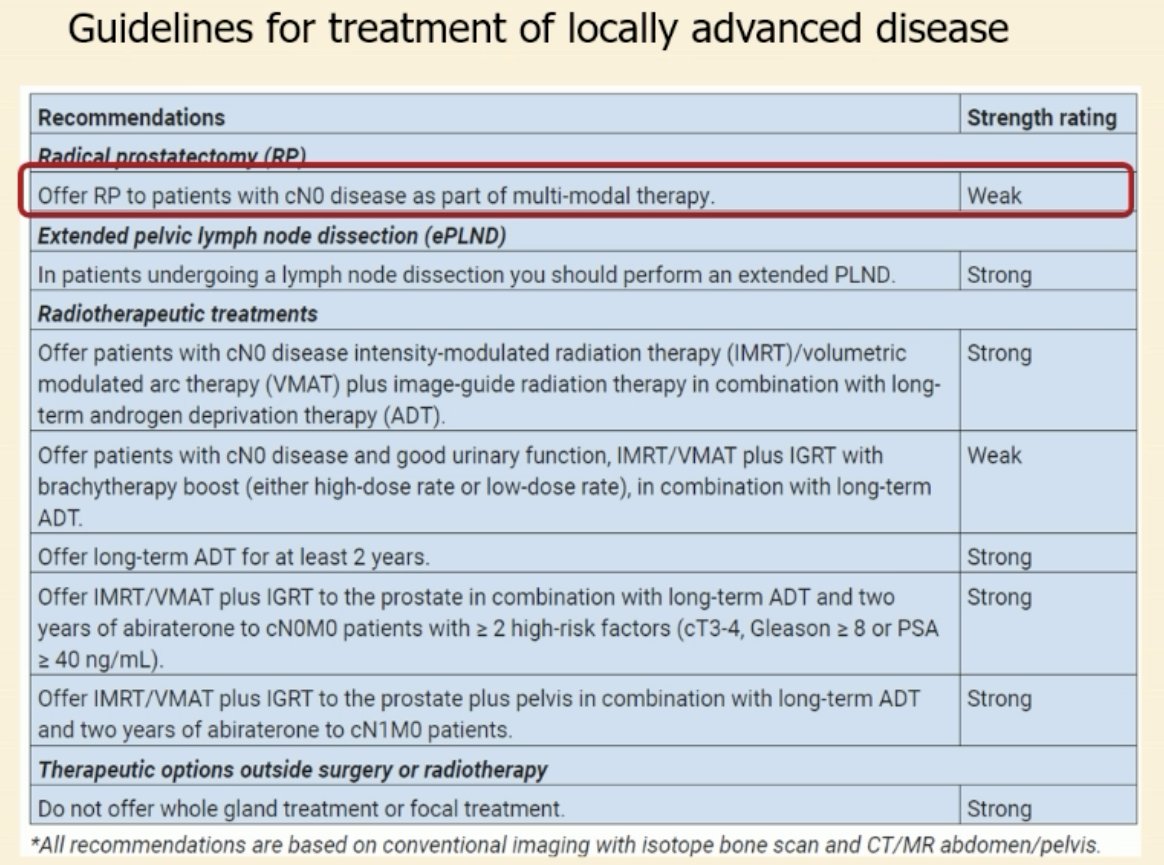
A common argument against radical prostatectomy in this setting is that most patients will require adjuvant/salvage pelvic radiotherapy either way. Dr. Briganti noted that historical data suggests that many such patients with cT3b prostate cancer are able to avoid adjuvant radiotherapy post-radical prostatectomy (>50%) and have excellent long-term survival outcomes.2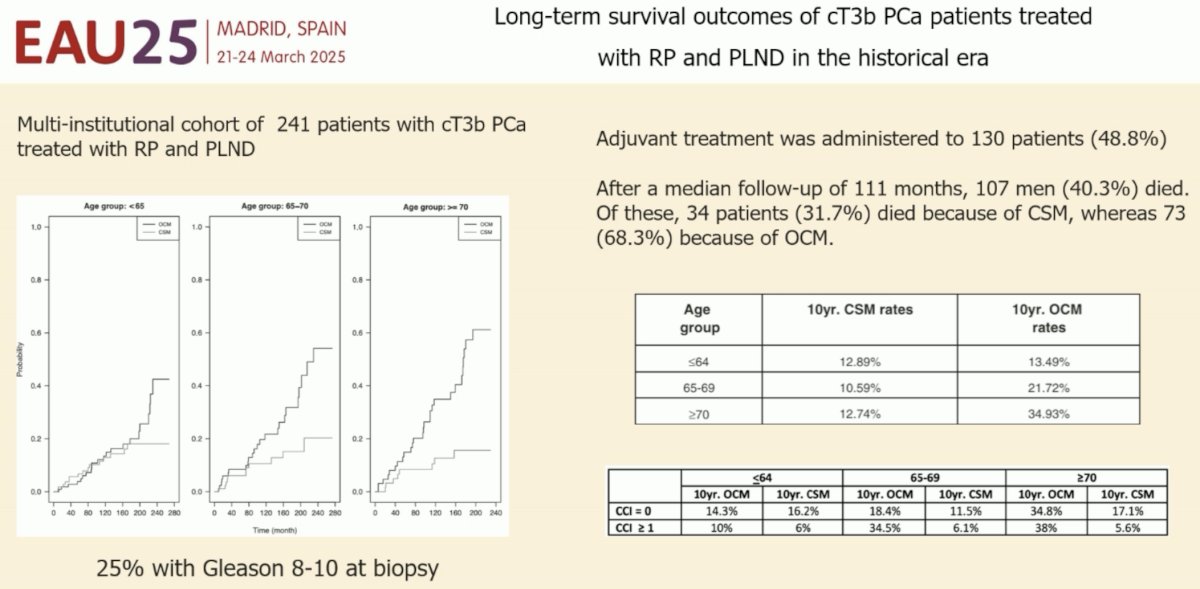
What proportion of patients with iT3b disease have pathologic nodal involvement? Unpublished data from Dr. Briganti’s group indicates that ~50% of iT3b patients are found to have pN1 disease. Of these 50% of patients, 42% of patients have only 1-2 involved lymph nodes. As such, ~75% of patients have either pN0 disease or pN+ disease with 1-2 positive nodes only that, in theory, could be addressed with an ePLND.
Another advantage of radical prostatectomy for this patient is that it provides accurate pathologic grading and staging information that may help guide a risk-adapted approach to adjuvant radiotherapy utilization, with adjuvant radiotherapy reserved for the high-risk patients.1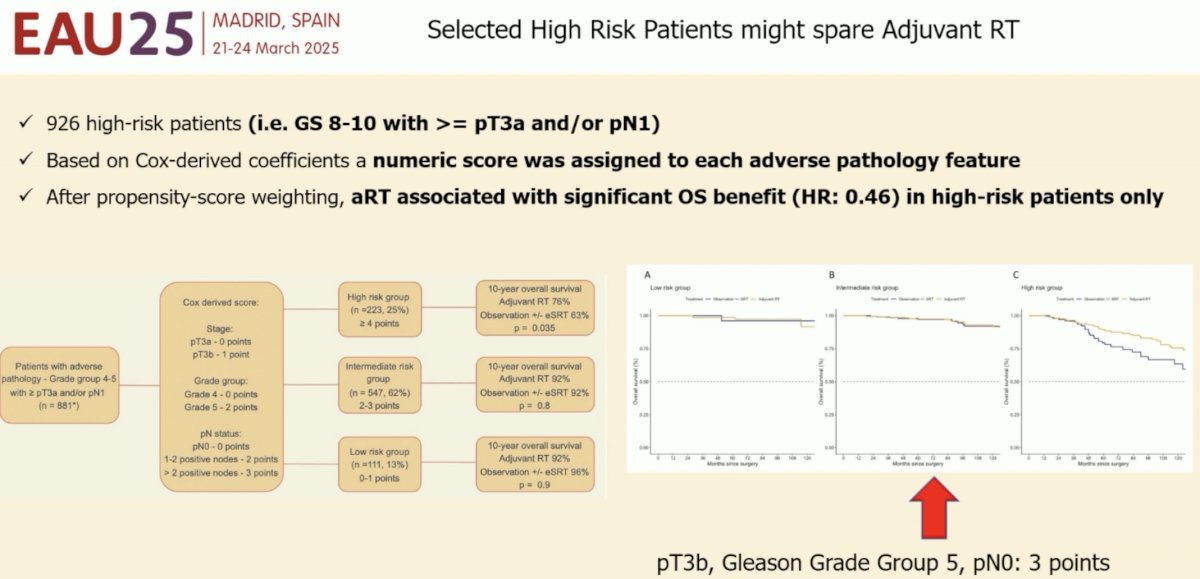
What is the role of ePLND in such a candidate patient? Extended follow-up of the MSKCC randomized trial of extended versus limited PLND suggests that ePLND reduces the incidence of distant metastases (HR: 0.75, p<0.001), and this benefit appears to be most significant in patients with pN1 disease (HR: 0.49, p<0.001).3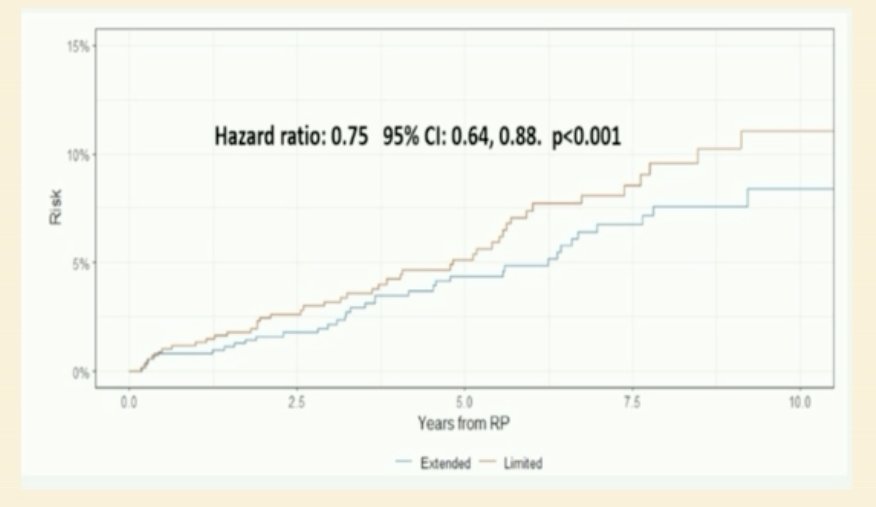
Dr. Briganti acknowledged that erectile dysfunction is a concern post-radical prostatectomy; however, he countered by noting that 18-36 months of ADT when combined with radiotherapy is also inevitably associated with erectile dysfunction. Urinary incontinence is also an important issue to counsel patients on; however, early and late continence outcomes are now significantly improved with robotic approaches.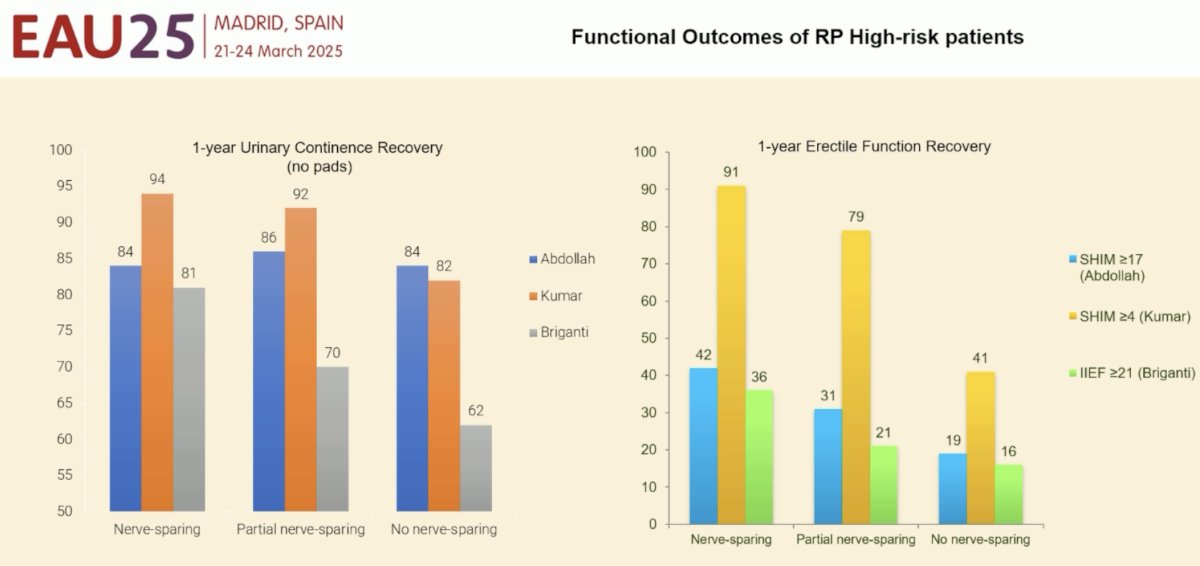
Dr. Briganti concluded as follows:
- Surgery is an option for iT3b disease
- To date, there is no formal comparison with radiotherapy + ADT +/- abiraterone
- Intensification is not always needed
- Surgery can be followed by tailored approaches
- One treatment does not fit all
Next, Dr. Piet Ost argued in favor of radiotherapy +/- combination systemic therapy in this setting. He noted that there are 4 important radiotherapy variables to consider:
- Dose
- Field
- Duration
- Combination with systemic therapy
Addressing the ‘field’ variable, do we need to include the pelvic nodes in the irradiation field or is the prostate alone sufficient? The NRG/RTOG 9413 trial was a 2 x 2 factorial study that evaluated the role of whole pelvic radiotherapy (versus prostate only), along with the timing of hormone therapy (neoadjuvant versus adjuvant). This phase III trial randomized 1,322 prostate cancer patients with conventional imaging-defined node negative disease and an estimated lymph node involvement risk of >15% to one of four treatment arms in a 1:1:1:1 fashion:
- Whole pelvic radiotherapy + neoadjuvant hormone suppression
- Prostate only radiotherapy + neoadjuvant hormone suppression
- Whole pelvic radiotherapy + adjuvant hormone suppression
- Prostate only radiotherapy + adjuvant hormone suppression.
The 10-year progression-free survival estimates favored the whole pelvic irradiation + neoadjuvant hormone arm (28.4% versus 19–24% for other arms).4 Dr. Ost noted that these results established the importance of pelvic nodal irradiation for these higher risk patients.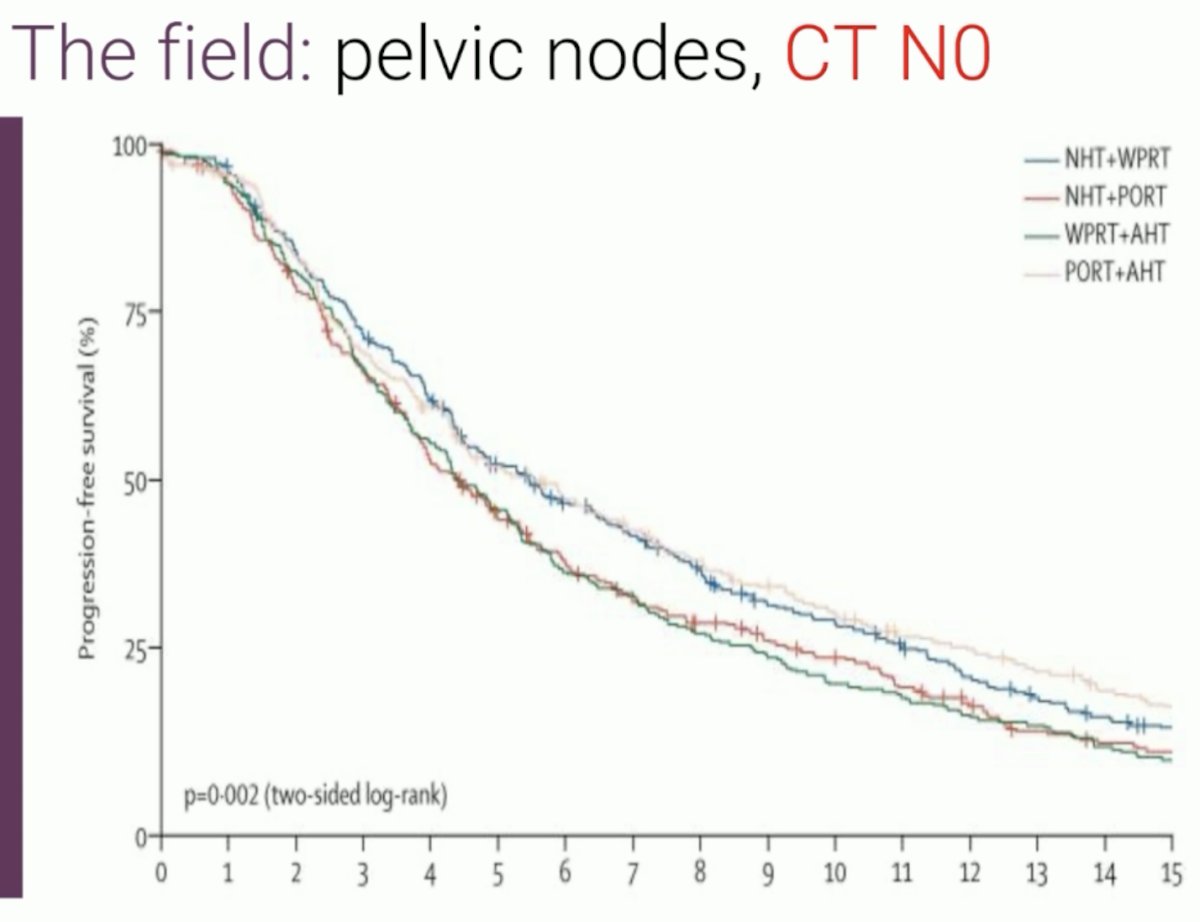
What about patients with node-negative disease on PSMA PET imaging? Do these patients also need pelvic irradiation? POP-RT is a phase III trial that randomized 224 prostate cancer patients with PSMA PET-defined node negative disease and an estimated nodal risk ≥ 20% to either prostate-only radiation therapy (68 Gy in 25 fractions) or whole pelvic radiotherapy (68 Gy in 25 fractions to the prostate plus 50 Gy to the pelvic nodes, including common iliacs). All patients received image-guided, intensity-modulated radiotherapy and a minimum of two years of androgen deprivation therapy. Over a median follow-up of 68 months, the 5-year biochemical failure-free survival was superior in the whole pelvis arm (95% versus 81.2%; HR: 0.23; p<0.001), as well as 5-year disease-free (89.5% versus 77.2%; HR: 0.40, p=0.002) and distant metastasis-free survivals (95.9% versus 89.2%; HR: 0.35, p=0.01). There were no significant differences in 5-year overall survival rates (92.5% versus 90.8%, HR: 0.92, p=0.93).5 As such, Dr. Ost argued that whole pelvis radiotherapy is indicated for higher risk patients, even in the setting of PSMA PET node negative disease.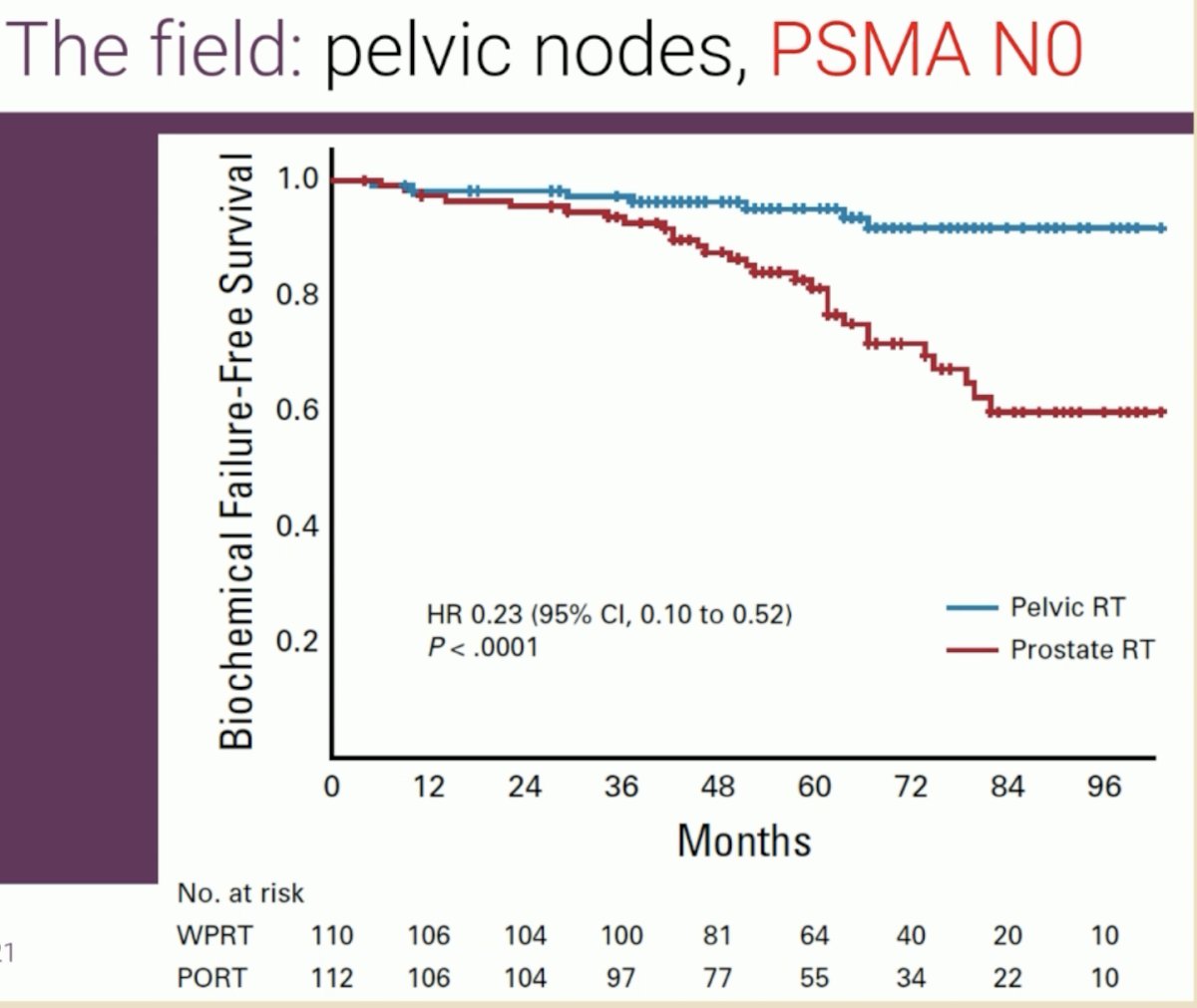
What about the duration of systemic therapy? Should these patients receive 6 months or 18–36 months of ADT? An individual patient data meta-analysis published by Kishan et al. in 2022 demonstrated that long-term ADT improves 10-year metastasis-free survival rates, compared to short-term ADT (55% versus 47%; HR: 0.84, p<0.0001).6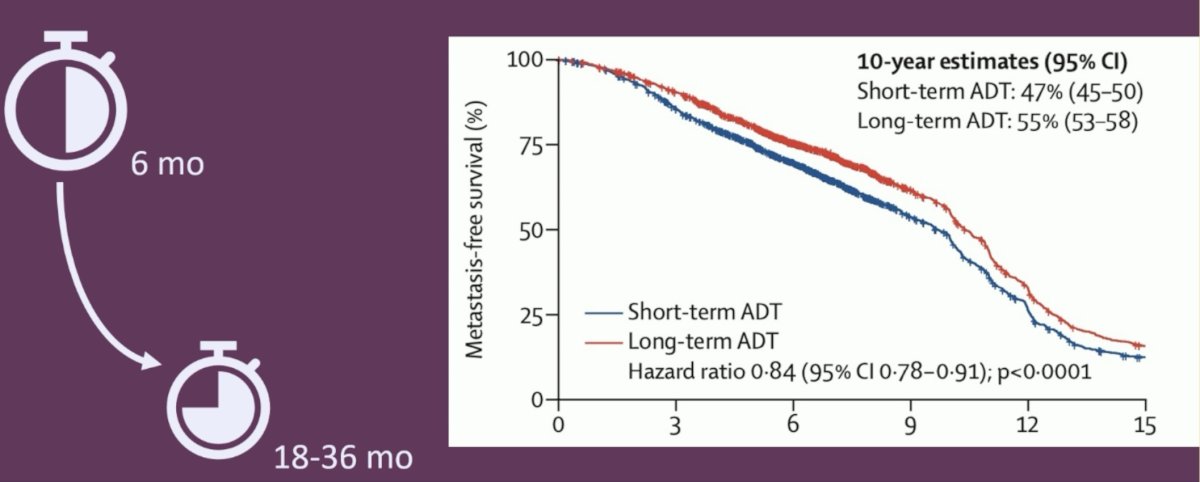
What about systemic therapy intensification with an androgen receptor pathway inhibitor (ARPI)? In 2022, the combined results of two phase III trials (STAMPEDE arms G and J) were published in The Lancet in 2022.7 These arms of the STAMPEDE trial were designed to assess the benefit of ARPI addition to standard of care treatment for men with high-risk non-metastatic prostate cancer, as per conventional imaging, defined as:
- Node positive, OR
- If node negative:
- High-risk, defined by at least two of the following:
- cT3-4
- Gleason Score 8-10
- PSA ≥40 ng/mL
- High-risk, defined by at least two of the following:
The addition of abiraterone +/- enzalutamide to radiotherapy + ADT was associated with improved metastasis-free survival (HR: 0.53, 95% CI: 0.44–0.64, p<0.000). Secondary outcomes of overall survival (HR: 0.60, 95% CI: 0.48–0.73), prostate cancer-specific survival (HR: 0.49, 95% CI: 0.37–0.65), biochemical failure-free survival (HR: 0.39, 95% CI: 0.33–0.47), and progression-free survival (HR: 0.44, 95% CI: 0.36–0.54) were all superior with the addition of abiraterone +/- enzalutamide to radiotherapy + ADT.
Dr. Ost concluded his argument in favor of radiotherapy in this setting as follows:
- Pelvic radiotherapy improves outcomes for select PSMA negative high-risk patients
- Long-term ADT improves outcomes over short-term ADT
- The combination of ADT + an ARPI improves outcomes for patients with a combination of high-risk features
Next, Dr. Ursula Vogl provided the medical oncologist perspective, focusing on the importance of systemic therapy intensification with abiraterone acetate for patients meeting the STAMPEDE high risk eligibility criteria.
She noted the importance of local staging with MRI/PSMA PET in the case example, as node-negative patients with evidence of cT3 disease on imaging may meet one of the high-risk criteria outlined in the STAMPEDE eligibility criteria (cT3-4). While clinical staging is, by definition, reliant on physical examination findings, a consensus poll from the APCCC panel suggests that 92% of the experts believe that patients with evidence of cT3a disease on MRI, but cT2 on DRE, should be treated as cT3 disease. Additionally, it is important to obtain baseline testosterone levels prior to initiating ADT +/- abiraterone therapy to assess subsequent recovery of testosterone levels following treatment suspension.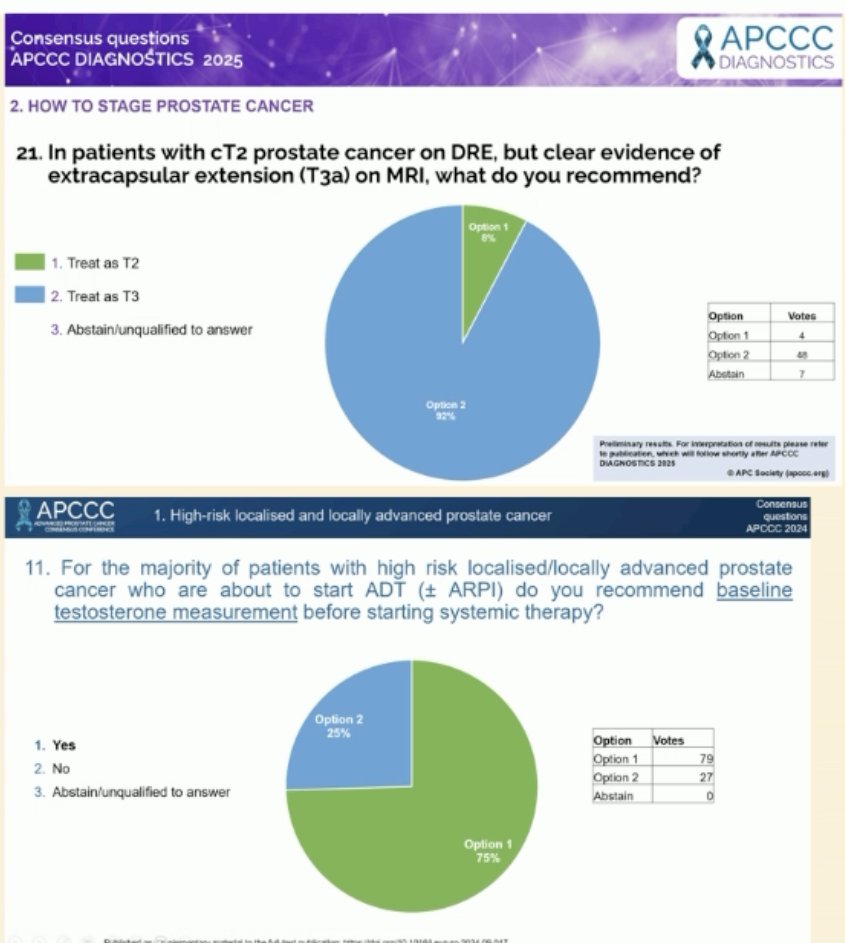
In the majority of patients with high-risk localized/locally advanced prostate cancer (STAMPEDE definition) with N0M0 on next-generation imaging, what is the recommended treatment? The majority of the APCCC panel (68%) reported that radiotherapy + long-term ADT + 2 years of abiraterone is the preferred approach in this setting:
Dr. Vogl also highlighted the data from the STAMPEDE abiraterone data published by Attard et al in 2022 emphasizing that careful patient selection for such systemic therapy intensification is crucial, requiring a fit and compliant patient who is well-screened for potential short and long-term toxicity.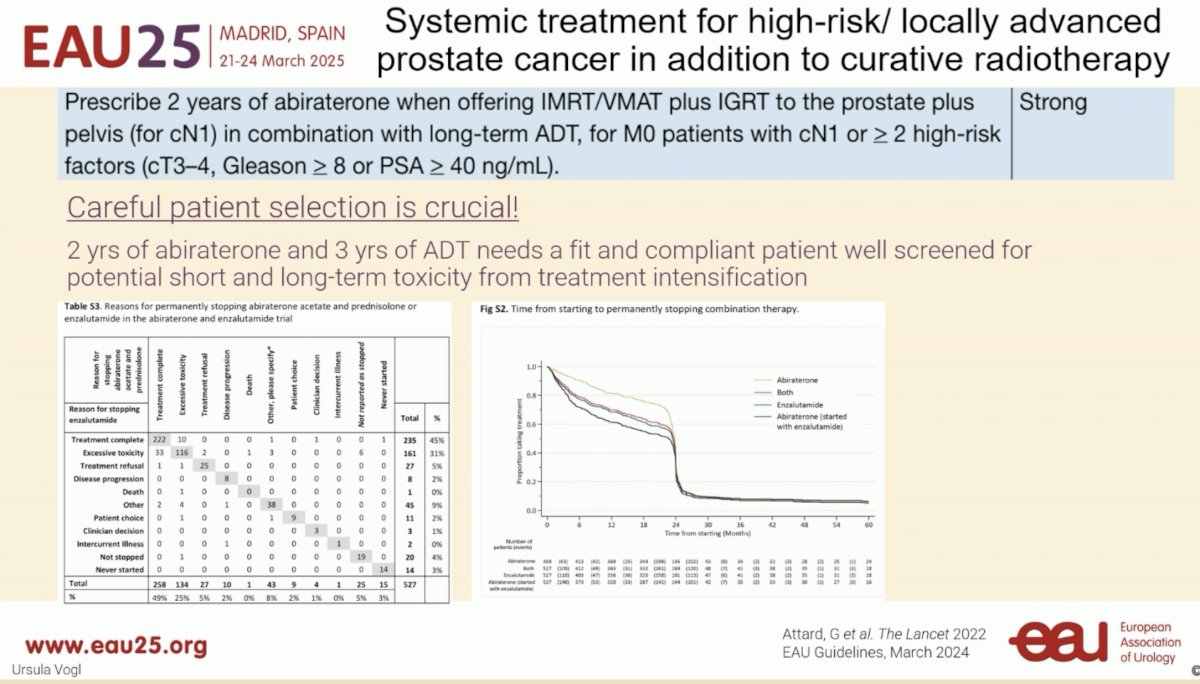
Dr. Vogl concluded as follows:
- Adding two years of abiraterone to three years of ADT in patients undergoing curative radiotherapy for high-risk/locally advanced prostate cancer (fulfilling STAMPEDE Attard et al. criteria) is the standard of care (EAU guidelines – strong recommendation)
- Careful patient selection is crucial – not every patient is a candidate for ‘maximum’ treatment
- Think about short- and long-term toxicity (bone health, cardiovascular, negative metabolic effects) and employ preventative measures
Presented by:
- Alberto Briganti, MD, Professor of Urology, Università Vita-Salute San Raffaele, Deputy Director, Urological Research Institute (URI) of IRCCS Ospedale Università Vita-Salute San Raffaele, Milan, Italy
- Piet Ost, MD, PhD, Associate Professor, Radiation Oncology, Faculty of Medicine and Health Sciences, University of Gent, Belgium
- Ursula Vogl, MD, MBA, Oncology Institute of Southern Oncology, Istituto Oncologico della Svizzera Italiana, Prostate Center of Southern Switzerland Bellinzona, Switzerland
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 European Association of Urology (EAU) Annual Congress held in Madrid, Spain between March 21st and 24th, 2025
References:- Mazzone E, Gandaglia G, Ploussard G, et al. Risk Stratification of Patients Candidate to Radical Prostatectomy Based on Clinical and Multiparametric Magnetic Resonance Imaging Parameters: Development and External Validation of Novel Risk Groups. Eur Urol. 2022; 81(2): 193-203.
- Moltzahn F, Karnes J, Gontero P, et al. Predicting prostate cancer-specific outcome after radical prostatectomy among men with very high-risk cT3b/4 PCa: a multi-institutional outcome study of 266 patients. Prostate Cancer Prostatic Dis. 2015; 18(1): 31-7.
- Touijer KA, Vertosick EA, Sjoberg DD, et al. Pelvic Lymph Node Dissection in Prostate Cancer: Update from a Randomized Clinical Trial of Limited Versus Extended Dissection. Eur Urol. 2025; 87(2): 253-60.
- Roach M, Moughan J, Lawton CA, et al. Sequence of hormonal therapy and radiotherapy field size in unfavourable, localised prostate cancer (NRG/RTOG 9413): long-term results of a randomised, phase 3 trial. Lancet Oncol. 2018; 19(11): 1504-15.
- Murthy V, Maitre P, Kannan S, et al. Prostate-Only Versus Whole-Pelvic Radiation Therapy in High-Risk and Very High-Risk Prostate Cancer (POP-RT): Outcomes From Phase III Randomized Controlled Trial. J Clin Oncol. 2021; 39(11): 1234-42.
- Kishan AU, Sun Y, Hartman H, et al. Androgen deprivation therapy use and duration with definitive radiotherapy for localised prostate cancer: an individual patient data meta-analysis. Lancet Oncol. 2022; 23(2): 304-16.
- Attard G, Murphy L, Clarke NW, et al. Abiraterone acetate and prednisolone with or without enzalutamide for high-risk non-metastatic prostate cancer: a meta-analysis of primary results from two randomised controlled phase 3 trials of the STAMPEDE platform protocol. Lancet. 2022; 399(10323): 447-60.