(UroToday.com) The 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain was host to the session Progress and Controversies in oncological urology from the EAU Section of Oncological Urology. Dr. Elena Castro debated why ADT + ARPI is all that is needed for de novo low-volume metastatic hormone-sensitive prostate cancer.
Dr. Castro began her presentation by reviewing the case of a patient with locally advanced prostate cancer: cT3, PSA 4.8 ng/mL, ISUP Grade Group 5, and PI-RADS 5. While conventional imaging classified the patient as cN0M0, PSMA PET revealed two focal lesions, reclassifying the disease as miN0M1.

At the APCCC (Advanced Prostate Cancer Consensus Conference) last year, the panelists were asked what they recommend for patients with clinically high-risk localized or locally advanced prostate cancer and a single prostate-specific membrane antigen (PSMA) positron emission tomography (PET)-positive bone lesion without a correlate on the computed tomography component. Notably, 55% responded that they would confirm the presence of metastasis using another imaging technique or a biopsy:

Current evidence is based on conventional imaging, and there is no justification for treating PSMA PET-positive disease as metastatic in the absence of corresponding findings on conventional imaging. The EAU guidelines explicitly state that treatment decisions for metastatic prostate cancer rely on disease detected through bone scintigraphy and CT or MRI (Conventional imaging). It would be a mistake to assume that PSMA PET findings alone will lead to the same clinical outcomes.
Continuing with the case of our patient, he underwent radical prostatectomy but had a persistent PSA of 0.28 ng/mL post-surgery. A postoperative PSMA PET scan revealed focal uptakes at the pubis and left ischial tuberosity—findings consistent with the preoperative scan. Now, with evidence of metastatic disease, the focus shifts to treatment. The proposed approach includes whole pelvis radiotherapy (WPRT) and metastasis-directed therapy (MDT). However, Dr. Castro raised an important question: What is the evidence supporting the use of MDT in this setting?
The answer is that currently there is no solid evidence supporting MDT in this setting. A systematic review and meta-analysis evaluating MDT for oligometastatic prostate cancer found that most prospective data come from small phase 1/2 studies. Until the results of ongoing randomized phase 3 trials are available, MDT in the context of treatment intensification remains a promising but investigational approach with an uncertain impact on overall survival.
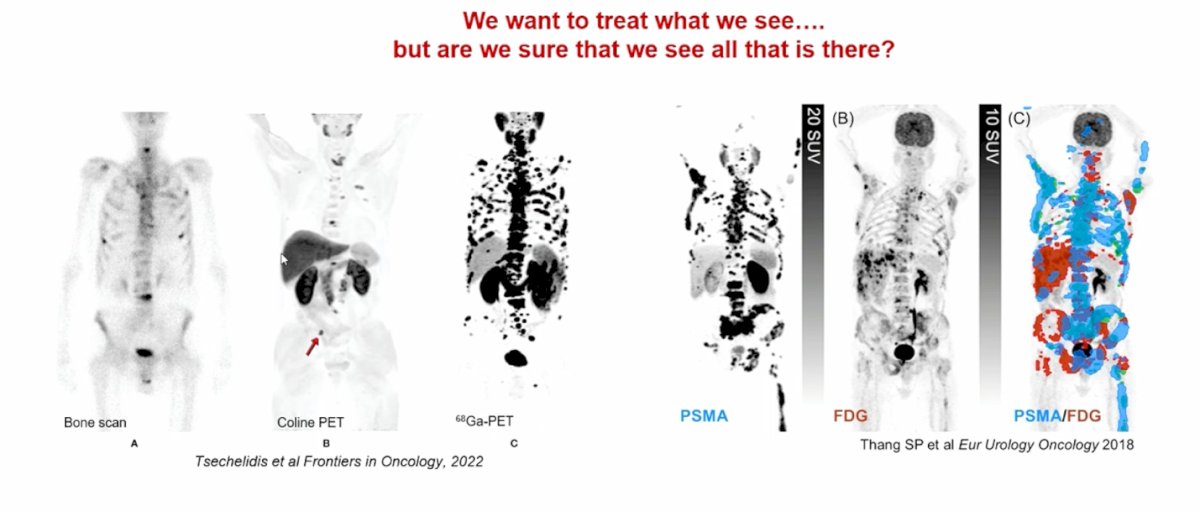
Another key consideration is that we often focus on treating what we see. With different radiotracers and radionuclides available, it is tempting to target only the visible metastases. However, this approach may address only the tip of the iceberg rather than the underlying disease. These patients require systemic therapy to manage the full extent of their cancer
Androgen receptor pathway inhibitors (ARPI) have been shown to improve survival outcomes across all stages of prostate cancer, including metastatic hormone-sensitive prostate cancer (mHSPC), non-metastatic castration-resistant prostate cancer (nmCRPC), castration-resistant prostate cancer (CRPC), biochemical recurrence, and even high-risk localized or locally advanced disease. Given this broad efficacy, it is likely that ARPI could also improve outcomes in patients with PSMA PET-positive–only metastatic disease.

Dr. Castro concluded her presentation by emphasizing two key questions that remain unanswered when treating these patients with androgen receptor pathway inhibitors (ARPI):
- How should we monitor these patients? Should we rely on regular PSMA PET scans or prostate-specific antigen (PSA) levels?
- What should be the duration of treatment? Should ARPI therapy be continued indefinitely, or is there a possibility to de-escalate and eventually stop treatment?
She highlighted that there is still much to learn about the optimal management of ARPI therapy in this setting.
Presented by: Elena Castro, MD, PhD, Medical Oncologist. Hospital Universitario 12 de Octubre, Madrid, Spain.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain between March 21st and 24th 2025