(UroToday.com) The 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain between March 21st and 24th 2025, was host to the Biomarkers to guide peri-operative management in Uro-oncology Plenary Session. Dr. Martin Gleave delivered a presentation on the current landscape of peri-operative therapies in localized prostate cancer.
Dr. Gleave began by highlighting the goals of neoadjuvant therapies in high-risk localized prostate cancer (PCa), which include improving cancer control by enhancing local control (reducing positive surgical margins) and reducing recurrence through an impact on micrometastases, ultimately prolonging metastasis-free survival (MFS) and overall survival (OS). Additionally, neoadjuvant approaches provide a window of opportunity for molecular correlative studies, allowing insights into mechanisms of action, therapeutic response, and drug resistance. These strategies also contribute to drug development by refining pharmacokinetic and pharmacodynamic (pk/pd) endpoints.
The rationale behind neoadjuvant androgen deprivation therapy (ADT) studies is based on its role as a radiosensitizer, which reduces tumor volume, decreases tumor hypoxia, and increases DNA stress. This has led to its adoption as the standard of care in combination with radiotherapy.
Early pre-surgical trials in the 1990s comparing 0 vs. 3 months and 3 vs. 8 months of neoadjuvant ADT demonstrated a 50% reduction in positive margin rates, but pathologic complete response (pCR) rates remained low (<8%), and biochemical recurrence (BCR) rates were similar between groups. However, these studies had several limitations:
- Patients were not selected for high-risk disease.
- The trials were underpowered to detect meaningful differences.
- The studies assessed the wrong endpoints for long-term benefit.
More recent data indicate that ARPI-based and ADT-docetaxel doublet therapies also yield low pCR rates, with only marginally improved outcomes, as seen in the CALGB 90203 (PUNCH) trial.1
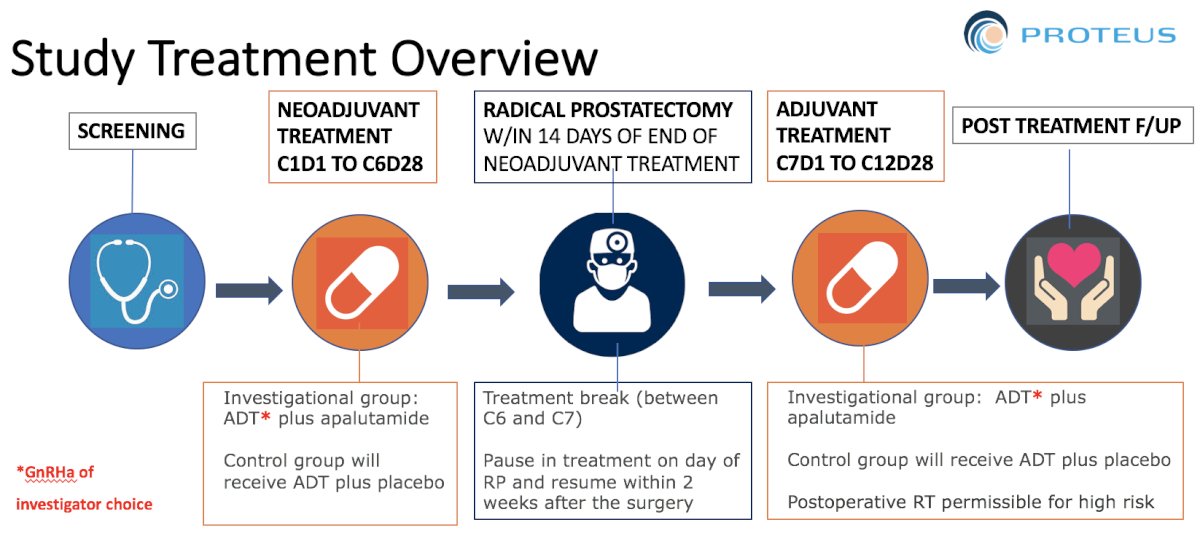
Neoadjuvant ADT StudiesPROTEUS was a Phase III randomized controlled trial evaluating 6 months of neoadjuvant plus 6 months of adjuvant LHRHa with or without apalutamide in men with high-risk localized prostate cancer. The trial enrolled 1,500 men, with dual primary endpoints of pathological complete response (pCR) rate and metastasis-free survival (MFS) as detected on PSMA PET. The study treatment design is shown below and results are eagerly awaited2
The current landscape of perioperative therapies in localized PCa includes several investigational approaches across multiple therapeutic classes, that could be broken down into eight groups:
1. ARPI Doublets
- Numerous phase II trials have been conducted, and the phase III PROTEUS trial has completed enrollment.
- CALGB 90203 (PUNCH): ADT + docetaxel
- ACDC Trial (NCT02543255): Evaluating anti-androgens and cabazitaxel in defining complete response in prostatectomy (UHN, Toronto).
- SWOG S2210: Neoadjuvant carboplatin for patients with localized PCa and germline DNA repair deficiency.
3. PARP Inhibitors (PARPi) – either in monotherapy or in combination with ARPI.
- NEPTUNE study: Neoadjuvant olaparib + ADT for high-risk localized PCa (Rana McKay).
- Ascertain: Pharmacokinetic/pharmacodynamic (pk/pd) study of AZ5305.
- Lu-177-PSMA-617.
- Neoadjuvant J591 Treatment for Prostate Cancer (NCT02693860) – Cornell University.
- PEM-PRO (NCT04565496): Phase II study of neoadjuvant pembrolizumab before radical prostatectomy in high-risk localized PCa (San Raffaele).
- SNARE (NCT05593497): Phase II study of neoadjuvant ARPI with capivasertib for HRLPCa with PTEN loss (VA Office of Research, Ryan P. Kopp).
Molecular Correlative Studies
In two studies evaluating the molecular characterization of genomic alterations after neoadjuvant treatment, the Phase III CALGB 90203 (Alliance) trial assessed neoadjuvant chemohormonal therapy. Investigators found that the mutation frequency of TP53 was higher in the chemotherapy-ADT arm compared to the control, while the mutation frequency of SPOP was lower in the chemotherapy-ADT arm than in Arm B.3,4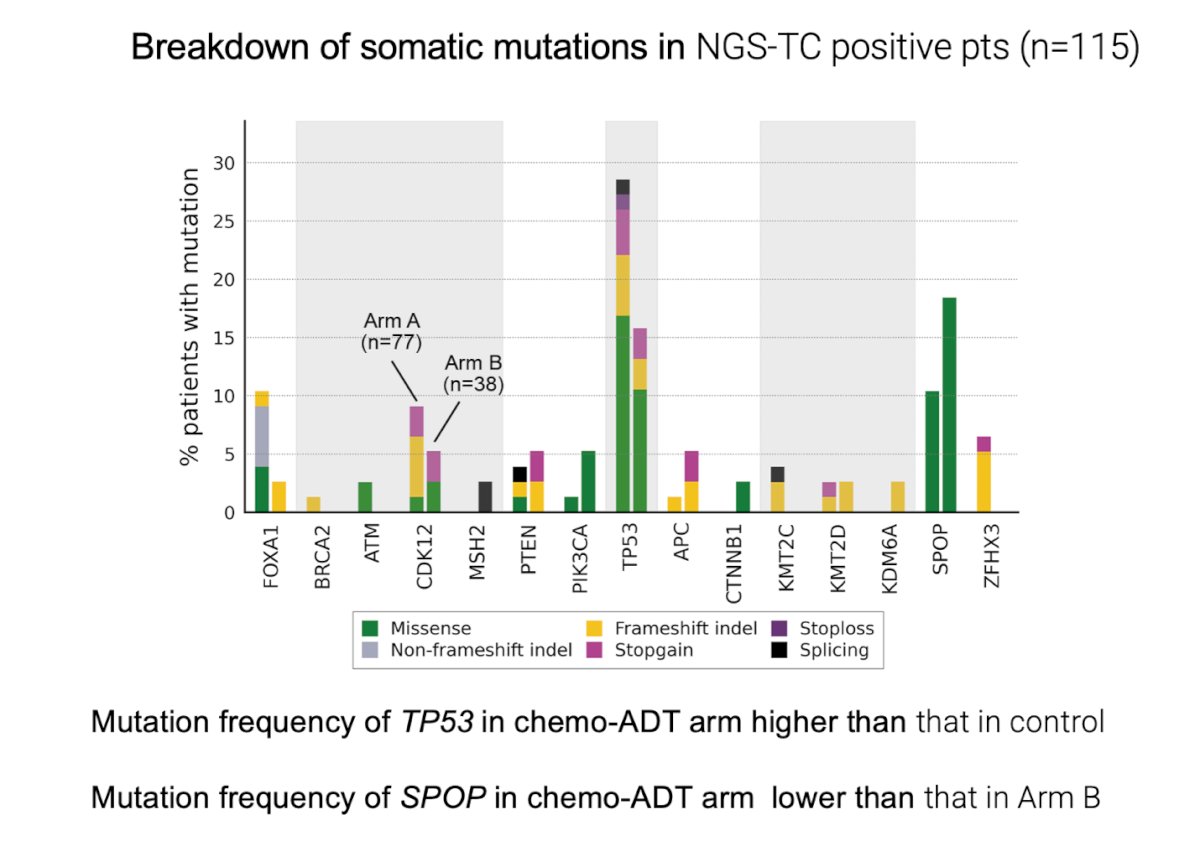
Moreover, the tumor fraction estimated from DNA sequencing was significantly lower in post-treated tumor tissues after chemohormonal therapy compared with controls. A higher tumor fraction after chemohormonal therapy was associated with aggressive pathologic features and poor outcomes, including prostate-specific antigen–progression-free survival. SPOP alterations were infrequently detected after chemohormonal therapy, while TP53 alterations were enriched and associated with shorter overall survival, this suggests a shift of subclonal segmentation in these cancers that were treated with neoadjuvant chemohormonal therapy. Similarly, they observed changes in mRNA expression in pre-treated and post-treated PCa tissues, with downregulation of AR-target genes like KLK3 and increased expression of AR-V7.3,4
As an example, Dr. Chi and colleagues evaluated co-targeting the stress response with the CLU inhibitor OGX-011. OGX-011 is an antisense inhibitor of clusterin and was assessed in combination with docetaxel/prednisone in patients with metastatic castration-resistant prostate cancer. They were the first to demonstrate that a drug like OGX-011 effectively hits its target in humans. Interestingly, induction of the ER stress markers ATF4 and GRP78 was not affected by YB-1 silencing, suggesting that YB-1 was not a general upstream activator of these ER stress markers but rather specifically upregulated CLU.5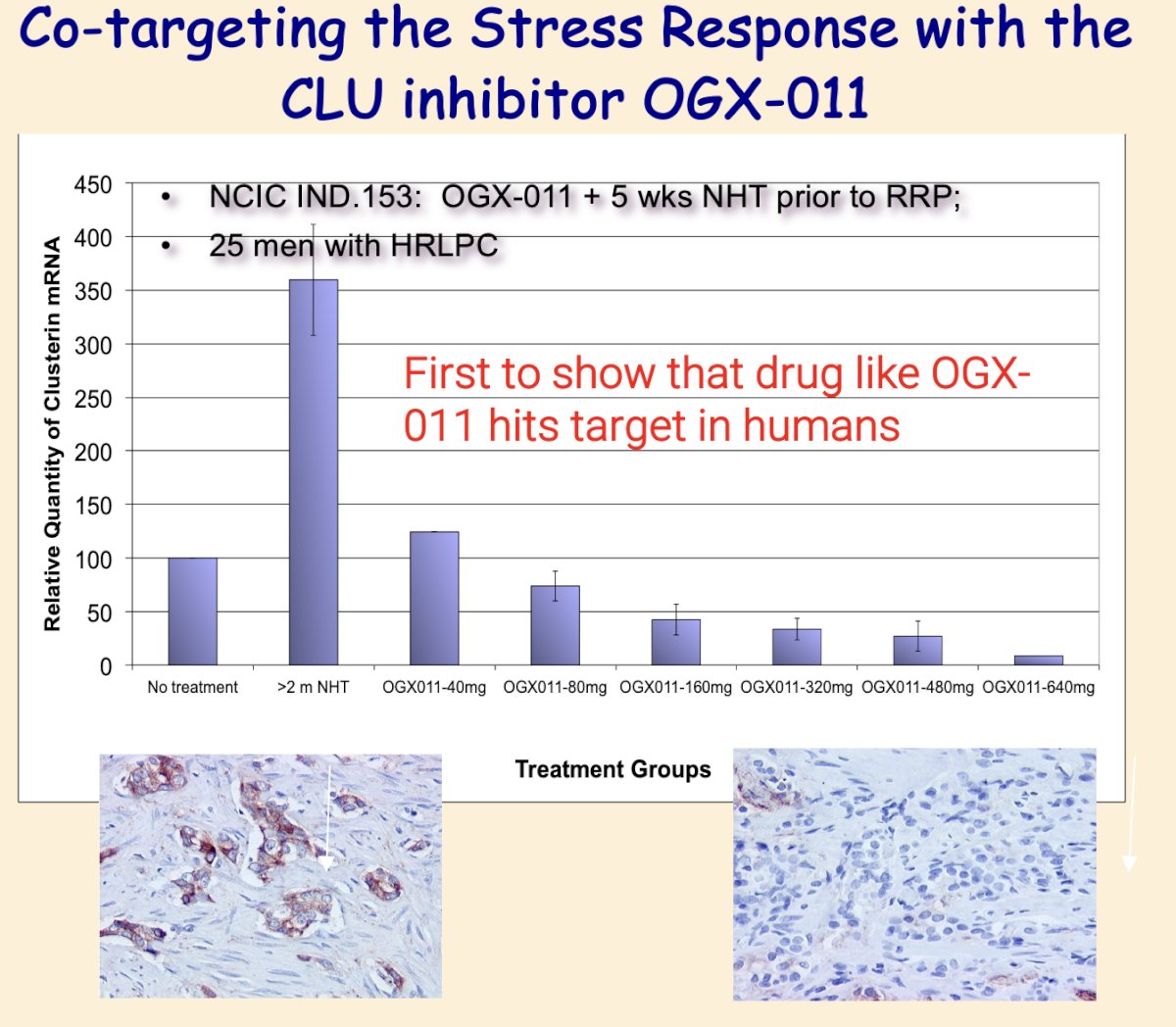
Moreover, an example of this type of study that is open now is the ASCERTAIN trial (study design illustrated below) is evaluating the mechanism of action of AZD5305 + ARPI. AZD5305 is a highly potent and selective inhibitor of PARP1 with 500-fold selectivity for PARP1 over PARP2. The primary endpoint is yH2AX assessing DNA damage.
Targeted Neoadjuvant Treatment for Patients with Localized Prostate Cancer and Germline DNA Repair Deficiency
The SWOG S2210 study (NCT05806515) explored the role of neoadjuvant carboplatin for high-risk localized prostate cancer with germline BRCA1/2 mutations. High-risk localized prostate cancer was defined as Gleason 8-10, Grade Group 4-5, PSA >20, or cT3 by conventional imaging. This study is still open, and investigators are actively recruiting patients alongside the GUNS study. However, patient recruitment has been challenging due to the need for established genetic testing infrastructure.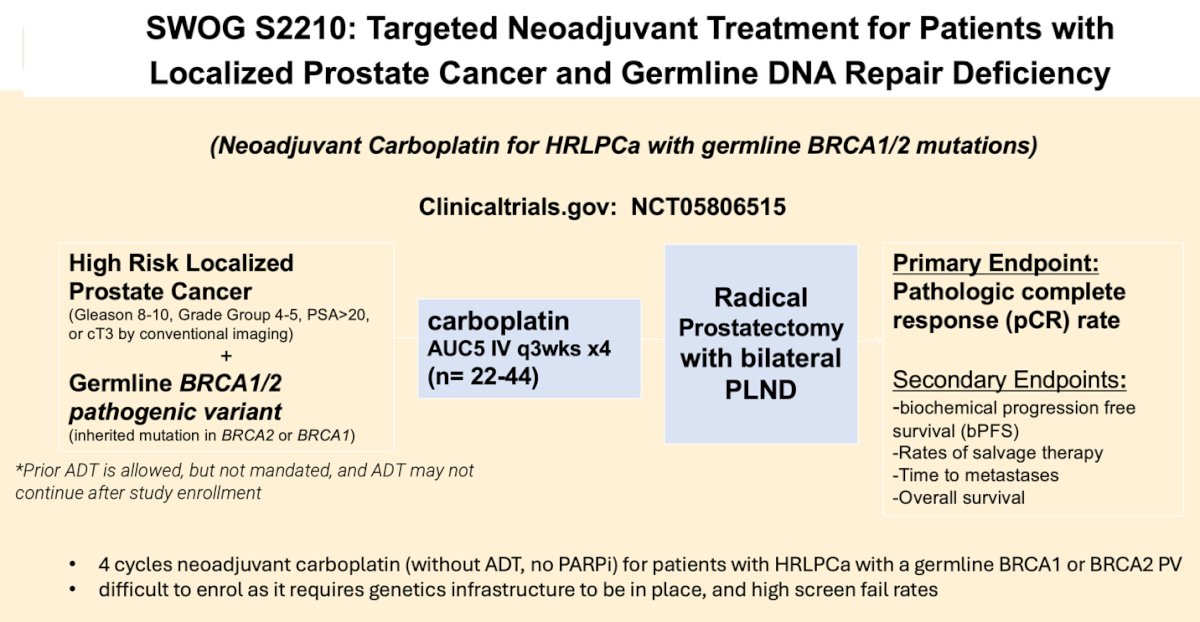
Biomarker-Driven Neoadjuvant Strategies in High Risk PCa
The rationale for biomarker-driven neoadjuvant strategies in high-risk prostate cancer lies in the ability of genomic sequencing to match targeted agents to distinct molecular aberrations. However, most defects occur in a small proportion of patients (10-20%), making clinical testing challenging with multiple single-agent, single-arm, phase II studies. Despite improved survival with ADT plus docetaxel or ARPI doublets in mCSPC, pCR rates remain low (<8%) when used neoadjuvantly in localized prostate cancer, differing from breast or bladder cancer, where pCR rates exceed 30%. This low pCR rate presents an opportunity to evaluate novel combinations, based on actionable genomic alterations, to improve pathological response
The Genomic Umbrella Neoadjuvant Study (GUNS)The GUNS trial (NCT04812366) is a multicenter, adaptive phase II umbrella study evaluating ARPI combination therapies in high-risk, localized prostate cancer (high-volume pattern 4, 5). Patients go on 8 weeks of LHRHa + Apalutamide while they await for their genomic profiling and assignment. Its goal is to define the impact of biomarker-selected targeted therapies on pathological response, including complete response (pCR) or minimal residual disease (MRD) <5 mm. Sub-protocols combine ARPI doublets with agents targeting specific genomic biomarkers, such as docetaxel for RB1, PTEN, and/or TP53 loss, niraparib for DNA damage repair (DDR) deficiency, and anti-PD-L1 for mismatch repair (MMR) deficiency. The trial initially enrolls 24 participants per arm, with arms being dropped if ≤5 achieve MRD. If ≥6 MRD cases are observed, 21 additional patients are accrued, totaling 45 per arm.
The rationale behind biomarker-driven neoadjuvant strategies in high-risk prostate cancer is that co-targeting the AR with other contextually relevant targets, defined by specific genomic subtypes, may enhance response depth (pCR, MRD). Multi-plexed and spatial analyses of post-treatment radical prostatectomy specimens can provide unique insights into emergent resistance mechanisms within distinct genomic subtypes when treated with precision-targeted regimens. Additionally, these approaches can help identify synthetic lethal regimens in genomically subtyped prostate cancer, guiding co-targeting strategies in metastatic disease.
Dr. Gleave presented a heatmap from DNA sequencing of 105 out of 127 patients, revealing a genomic landscape dominated by AR-related genes including T2E fusions (31%), FOXA1 (23%), and SPOP (13%) alterations. Other frequently altered genes included TP53 (14%), PTEN (12%), and BRCA2 (9%). Pre-treatment transcriptomes largely clustered according to ETS-fusion and SPOP status. ETS fusions were associated with the PCS2-luminal subtype and decreased proliferative signatures, whereas most other alterations were linked to the PCS1-luminal subtype. AR signatures were associated with SPOP and FOXA1 mutations but not with ETS fusions, as shown below.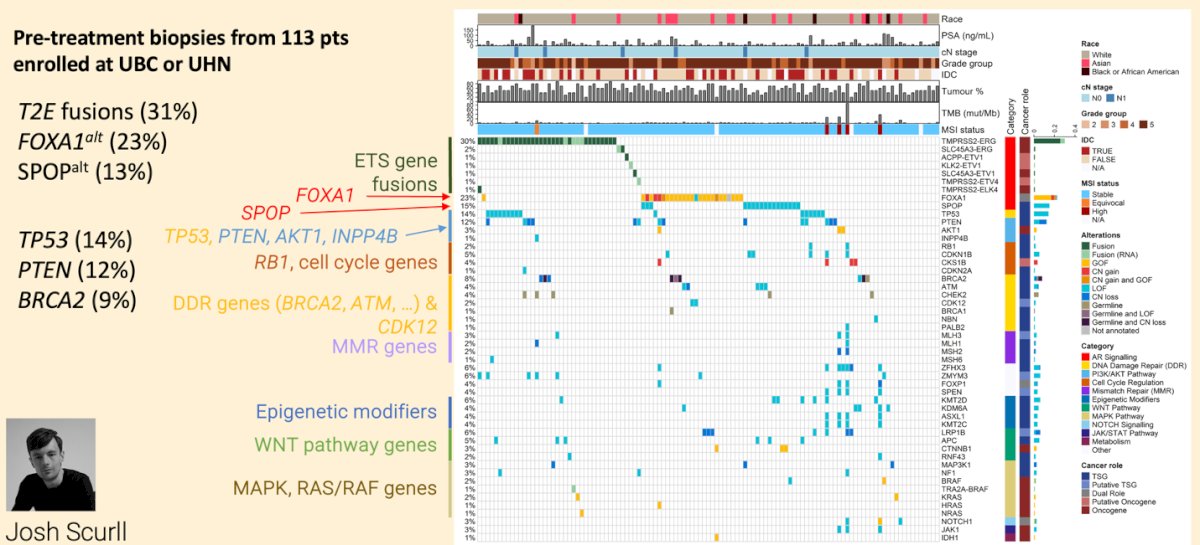
Dr. Gleave discussed that Sub-protocol (SP) 1 was divided into two sub-protocols for comparison:
- SP1a: ARPI doublet (LHRHa + APA)
- SP1b: ARPI triplet (LHRHa + APA + AAP)
They tested the hypothesis that ARPI triplet intensification, in cancers with AR-associated genomic alterations without co-occurring aggressive tumor suppressor gene (TSG) loss, would increase the depth of pathologic response. The results showed that the ARPI triplet yielded a higher MRD rate than the doublet (43% vs. 13%, p=0.012), with an odds ratio of 5.9, this is higher than they had anticipated. There were no data on pCR. Additionally, the rate of undetectable pre-surgery PSA was 70% in SP1b versus 49% in SP1a (p=0.12). Moreover, positive margin R1 (17%) and lymph node involvement (35% vs 26%) status were similar in both arms. The higher MRD rates in patients treated with the ARPI triplet compared to the doublet are noteworthy and support further evaluation with a second-stage expansion of SP, this subprotocol is being further expanded.
He discussed the case of patient 01-001 in GUNS, which exhibited an MSH2 alteration and high tumor mutational burden (TMB) in SP-4 after treatment. Notably, they also observed a significant increase in neuroendocrine prostate cancer signatures post-treatment, suggesting a potential shift in tumor biology.
This has led to the addition of two new sub-protocols, SP5 and SP6, GUNS now includes six sub-protocols:
- SP5: Patients with plasticity-associated alterations (TP53, RB1, ESC, NE) receive LHRHa/ABI + EZH2 inhibitor (Tazmetostat).
- SP6: Patients receive LHRHa/ABI + AKT inhibitor (Capivasertib), further divided into:
- SP6a: Genomically favorable cohort.
- SP6b: PTEN-deficient or AKT-gain cohort.

Dr. Gleave concluded his presentation with the following key messages:
- Neoadjuvant studies aim to reduce local and metastatic recurrence, but none has yet become standard of care (PROTEUS study of LHRHa + APA poised to read out in 2025)
- Despite improved survival of ADT plus docetaxel or ARPI doublets in mCSPC, pCR rates remain low (<8%) when used neoadjuvantly in high risk localized PCa
- Neoadjuvant studies provide a unique opportunity to test ability of novel combinations to increase depth of response and define emergent resistant mechanisms and window of opportunity trials to support mechanistic or pk/pd drug development
- GUNS is an adaptive window of opportunity trial using biomarker-directed combination regimens to evaluate path responses as a surrogate of contextual lethality
Presented by: Martin Gleave, CM, MD, FRCSC, FACS Urologic Oncologist at University of British Columbia and the Vancouver Prostate Centre.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain between March 21st and 24th 2025
References:- McKay RR, Xie W, Ye H, Fennessy FM, Zhang Z, Lis R, Calagua C, Rathkopf D, Laudone VP, Bubley GJ, Einstein DJ, Chang PK, Wagner AA, Parsons JK, Preston MA, Kilbridge K, Chang SL, Choudhury AD, Pomerantz MM, Trinh QD, Kibel AS, Taplin ME. Results of a Randomized Phase II Trial of Intense Androgen Deprivation Therapy prior to Radical Prostatectomy in Men with High-Risk Localized Prostate Cancer. J Urol. 2021 Jul;206(1):80-87.
- Adam S. Kibel et al. PROTEUS: A randomized, double-blind, placebo (PBO)-controlled, phase 3 trial of apalutamide (APA) plus androgen deprivation therapy (ADT) versus PBO plus ADT prior to radical prostatectomy (RP) in patients (pts) with localized or locally advanced high-risk prostate cancer (PC).. JCO 40, TPS285-TPS285(2022).
- Beltran H, Wyatt AW, Chedgy EC, Donoghue A, Annala M, Warner EW, Beja K, Sigouros M, Mo F, Fazli L, Collins CC, Eastham J, Morris M, Taplin ME, Sboner A, Halabi S, Gleave ME. Impact of Therapy on Genomics and Transcriptomics in High-Risk Prostate Cancer Treated with Neoadjuvant Docetaxel and Androgen Deprivation Therapy. Clin Cancer Res. 2017 Nov 15;23(22):6802-6811. doi: 10.1158/1078-0432.CCR-17-1034. Epub 2017 Aug 25. PMID: 28842510; PMCID: PMC5690882.
- Sumiyoshi T, Wang X, Warner EW, Sboner A, Annala M, Sigouros M, Beja K, Mizuno K, Ku S, Fazli L, Eastham J, Taplin ME, Simko J, Halabi S, Morris MJ, Gleave ME, Wyatt AW, Beltran H. Molecular features of prostate cancer after neoadjuvant therapy in the phase 3 CALGB 90203 trial. J Natl Cancer Inst. 2024 Jan 10;116(1):115-126.
- Chi KN, Hotte SJ, Yu EY, Tu D, Eigl BJ, Tannock I, Saad F, North S, Powers J, Gleave ME, Eisenhauer EA. Randomized phase II study of docetaxel and prednisone with or without OGX-011 in patients with metastatic castration-resistant prostate cancer. J Clin Oncol. 2010 Sep 20;28(27):4247-54.