(UroToday.com) The 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain between March 21st and 24th 2025, was host to the clinically relevant questions in the management of advanced, hormone-sensitive prostate cancer: Thematic session. Dr. Karim Fizazi delved into when to stop combined treatments in patients with high-volume disease at hormone sensitive prostate cancer with good response to therapy.
Dr. Fizazi emphasized that the key question we should be addressing is how long systemic treatment should be used—a complex issue with no easy answer. Historically, the standard for M1 disease has been lifelong systemic treatment, initially consisting of ADT alone.
M1 was traditionally defined based on conventional imaging, and we know that androgen deprivation therapy (ADT) improves overall survival. However, its side effects remain a concern and should be carefully managed and prevented. An important consideration is whether ADT can be stopped at some point in M1 disease and restarted when needed—raising the question of whether intermittent therapy could be a viable strategy.
In metastatic disease, the largest trial comparing continuous ADT to intermittent ADT (IADT) was the SWOG trial, which enrolled 1,535 patients with mCSPC. A good response was defined as a PSA value of ≤4 ng/mL. With a very long follow-up of 10 years, the trial reported a marginal quality-of-life benefit with IADT compared to continuous ADT. This is an important discussion to have with patients.
The trial was designed as a non-inferiority study, meaning the hypothesis was that IADT would not be inferior to continuous ADT. However, the median overall survival was 5 years with IADT versus 6 years with continuous ADT, suggesting a potential loss of nearly one year of survival with intermittent therapy.1
The key question is whether these findings also apply to patients with minimal disease. In the SWOG trial, minimal disease was defined as lymph node involvement only or bone metastases limited to the axial skeleton, with no visceral disease. In this subgroup, the difference in survival was even more pronounced—5.4 years of median OS with intermittent ADT versus 6.9 years with continuous ADT, a gap of 1.5 years.1 This raises concerns about the potential harm of using IADT in patients with M1 disease, particularly those with minimal metastatic burden.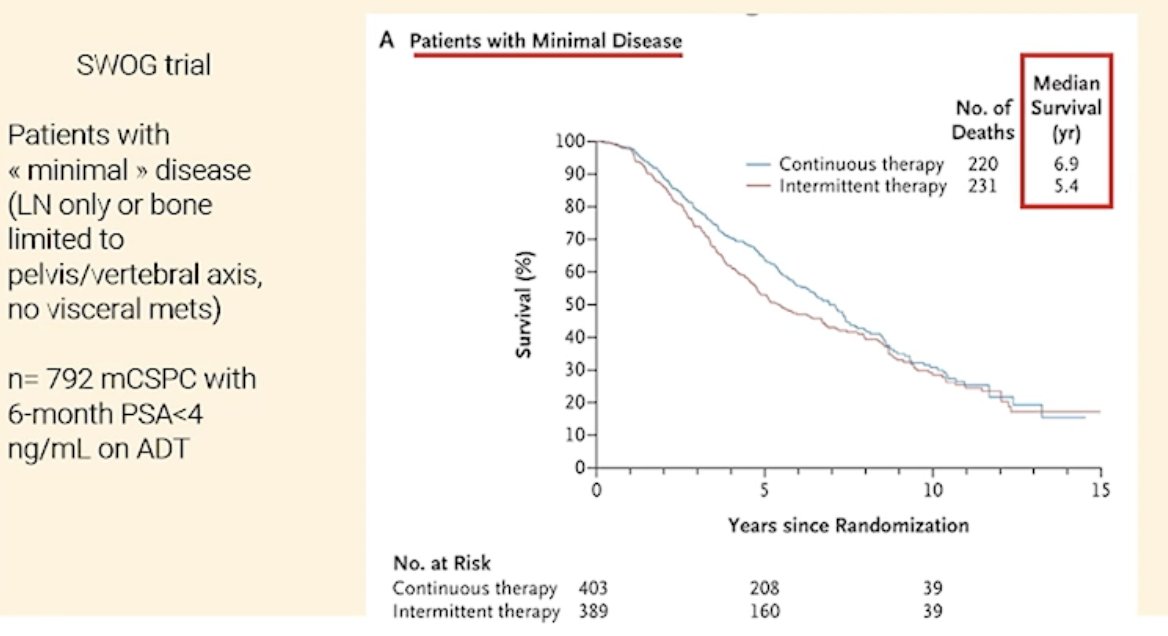
We know that longer ADT duration improves outcomes in high-risk localized disease, and it is very likely true in M1 as well. This provides a strong rationale to avoid short-term systemic treatment (6 months) in all-comer M1 patients.
Recent data from GETUG-15 analyzed 280 patients, selecting 89 who were long-term survivors 10 years after randomization. Notably, IADT was chosen in less than 10% of patients and only in 28% of long-term survivors. With a median follow-up of 13 years, 28% discontinued ADT, with a median discontinuation time of 6 years, and 60% did not require reinitiation.2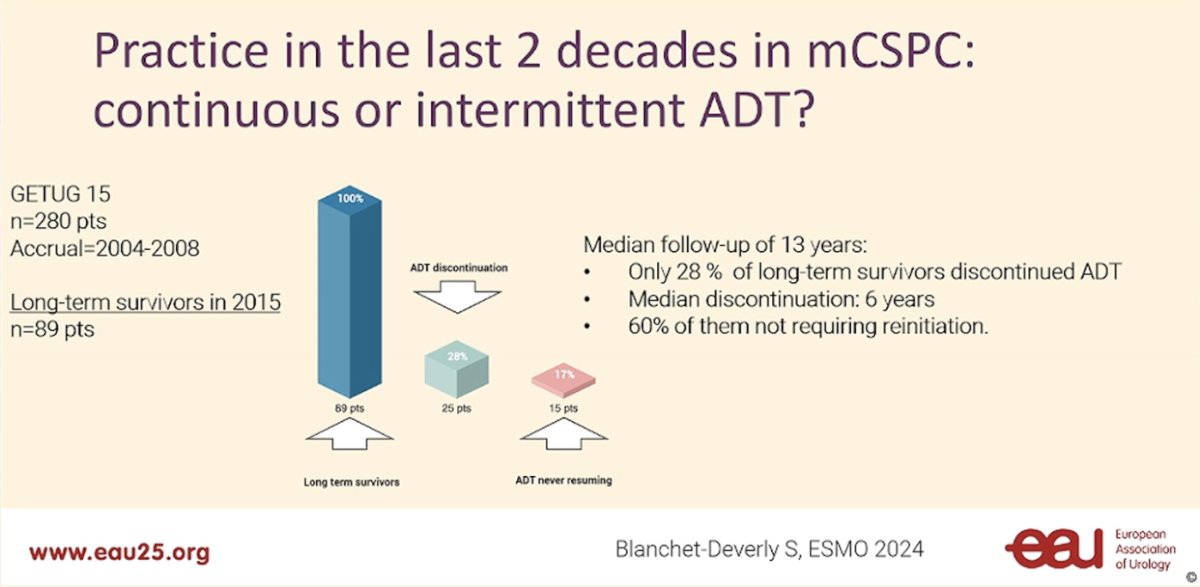
The historical standard for M1 disease: lifelong systemic treatment, remains relevant, but its role must be reconsidered in the current landscape of:
- Intensified systemic treatment combined with primary tumor radiotherapy
- M1 disease detected via PSMA-PET
- M1 relapse, which often exhibits a more indolent course compared to de novo M1 disease
A key question is whether we can better identify excellent responders. Evidence from PEACE-1 and other trials over the past decade strongly supports PSA cutoffs of 0.2 or 0 as a predictor of response. While de-escalation strategies might be considered for good responders, we currently lack the necessary evidence to support this approach.3
At APCCC last year, the audience was asked whether ADT should be stopped in favorable scenarios—specifically in patients with a deep remission (PSA <0.2). The response was divided: half supported stopping ADT, while 47% favored continuing continuous treatment. However, there is still no definitive answer to this question.
Dr. Fizazi noted that when faced with uncertainty, we should conduct randomized trials. The PEACE-6 study group, stratifies patients into good and poor responders based on PSA levels at 6 months.
For poor responders, a trial intensifying treatment with Lu-PSMA has already begun. For good responders, a separate randomized controlled trial, DE-ESCALATE, is being planned under the EORTC to evaluate treatment de-escalation strategies. The study design is as follows:
LIBERTAS is a pharma-sponsored trial evaluating treatment strategies for men with newly diagnosed mHSPC. Based on PSA response, patients will either receive treatment intensification or continue with standard treatment. The study design is outlined below.
Dr. Fizazi concluded his presentation with the following key points
- The optimal duration of systemic treatment in M1 disease remains unknown, and treatment should be individualized.
- Life-long ADT should remain the standard, as we do not want to harm patients.
- Stopping ADT should only be considered when systemic treatment becomes dangerous
- In other cases, intermittent ADT may be an option, but likely only if:
- There is an excellent response (PSA <0.2 ng/mL).
- The treatment duration has already been reasonable (2-3 years), though this remains uncertain.
- The patient is informed and motivated, but for those tolerating treatment well, stopping may not be the best approach.
- Trial participation should be encouraged to help answer all these pressing questions.
- In the future, biomarkers and AI may aid in decision-making.
Presented by: Karim Fizazi, MD, PhD, Medical Oncologist at Institut Gustave Roussy and Full Professor in Oncology at the University of Paris Saclay in Villejuif, France.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain between March 21st and 24th 2025
References:
- Hussain M, Tangen CM, Berry DL, Higano CS, Crawford ED, Liu G, Wilding G, Prescott S, Kanaga Sundaram S, Small EJ, Dawson NA, Donnelly BJ, Venner PM, Vaishampayan UN, Schellhammer PF, Quinn DI, Raghavan D, Ely B, Moinpour CM, Vogelzang NJ, Thompson IM Jr. Intermittent versus continuous androgen deprivation in prostate cancer. N Engl J Med. 2013 Apr 4;368(14):1314-25. doi: 10.1056/NEJMoa1212299. PMID: 23550669; PMCID: PMC3682658.
- Blanchet-Deverly A, Gravis G, Boher JM, et al. Long survivors after androgen deprivation therapy (ADT) with or without docetaxel for metastatic castration-sensitive prostate cancer (mCSPC): Long-term follow-up of GETUG-15. Ann Oncol. 2024;35(suppl_2):S962-S1003. doi: 10.1016/annonc/annonc1607.
- Fizazi K, Foulon S, Carles J, Roubaud G, McDermott R, Fléchon A, Tombal B, Supiot S, Berthold D, Ronchin P, Kacso G, Gravis G, Calabro F, Berdah JF, Hasbini A, Silva M, Thiery-Vuillemin A, Latorzeff I, Mourey L, Laguerre B, Abadie-Lacourtoisie S, Martin E, El Kouri C, Escande A, Rosello A, Magne N, Schlurmann F, Priou F, Chand-Fouche ME, Freixa SV, Jamaluddin M, Rieger I, Bossi A; PEACE-1 investigators. Abiraterone plus prednisone added to androgen deprivation therapy and docetaxel in de novo metastatic castration-sensitive prostate cancer (PEACE-1): a multicentre, open-label, randomised, phase 3 study with a 2 × 2 factorial design. Lancet. 2022 Apr 30;399(10336):1695-1707. doi: 10.1016/S0140-6736(22)00367-1. Epub 2022 Apr 8. PMID: 35405085.