(UroToday.com) The 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain between March 21st and 24th 2025, was host to the Biomarkers to guide peri-operative management in Uro-oncology Plenary Session. Dr. Andrea Necchi discussed the role of human papilloma virus (HPV) status in penile cancer as a potential biomarker in the perioperative setting.
Dr. Necchi began his presentation by highlighting that a significant proportion of penile cancers are related to human papillomavirus (HPV). Effective prevention among high-risk populations should include the implementation of personalized HPV vaccination programs and novel therapeutic agents, including immune-checkpoint inhibitors, which offer great promise in the management of advanced penile cancer.
The predictable clinical course of penile squamous cell carcinoma guides the main indications for lymph node dissection. Inguinal lymph node dissection (ILND) is recommended for patients with cN0 disease and high-risk features, those with cN1-N2 disease, and for cN3 disease following neoadjuvant chemotherapy. The role of pelvic lymph node dissection is much more controversial and is only endorsed if high-risk features are found at ILND pathology.
A study using the US National Cancer Database (NCDB) analyzed 1,123 patients with lymph node-positive (LN+) penile cancer and found that only 66.8% underwent lymph node dissection (LND). Notably, overall survival was significantly lower in patients who did not receive LND. Furthermore, while LND was associated with improved overall survival, neither chemotherapy nor radiotherapy showed a significant survival benefit, highlighting ongoing knowledge gaps regarding the role of perioperative treatments.1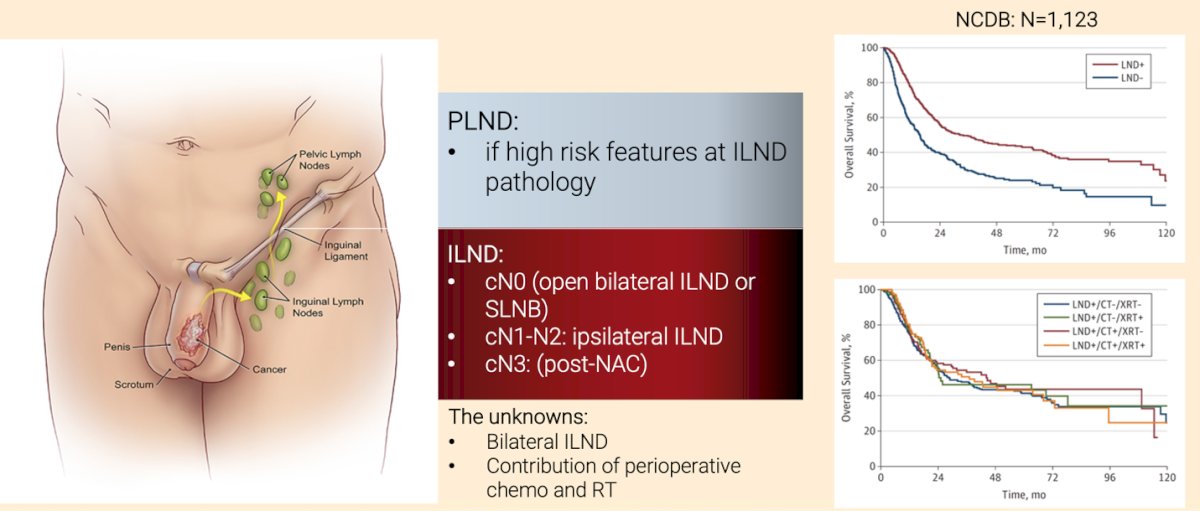
Dr. Necchi highlighted the joint efforts of the European Association of Urology (EAU) and the American Society of Clinical Oncology (ASCO) in developing the EAU-ASCO collaborative guidelines on penile cancer,2 as well as the recently published European Society for Medical Oncology (ESMO)-European Rare Adult Solid Cancer Network (EURACAN) practice guidelines.3 These initiatives underscore the increasing recognition of penile cancer and the ongoing efforts to enhance patient care.
The EAU-ASCO guideline recommends neoadjuvant chemotherapy as an alternative approach to upfront surgery for patients with bulky mobile inguinal nodes or bilateral disease (cN2). However, the strength rating of this recommendation is weak.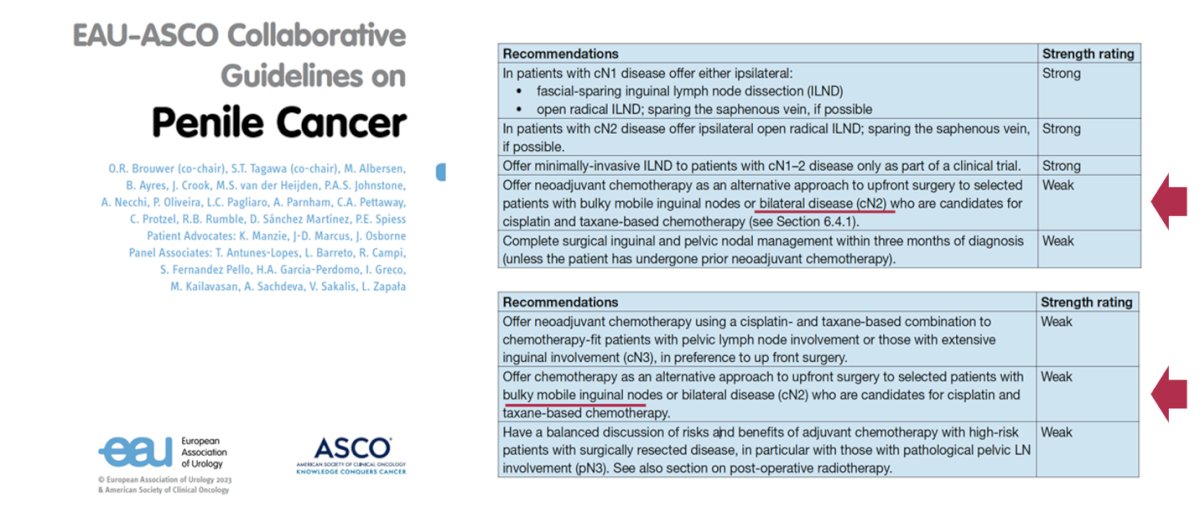
These recommendations are based on benchmark chemotherapy studies. Pagliaro et al. evaluated 30 patients with cN2/3 M0 squamous cell carcinoma (SCC) of the penis, reporting a time to progression of 8.1 months, overall survival of 17.1 months, and an overall response rate of 50% (3 complete responses and 12 partial responses). Among the 30 patients, 22 (73%) underwent radical resection, and 10 (33%) remained alive after a median follow-up of 34 months.5 Similarly, a systematic review and meta-analysis of perioperative chemotherapy in penile SCC, including 10 studies with 182 patients, reported a pooled overall response rate of 53%, a pathologic complete response rate of 16%, and grade ≥3 toxicity in 40% of patients. The overall mortality rate was 55%.6
The overall incidence of HPV DNA in penile squamous cell carcinoma ranges between 42-70%, with HPV prevalence varying across histologic subtypes—100% in the warty subtype and 80% in basaloid carcinoma. HPV-positive penile cancer is generally associated with a more favorable prognosis. Notably, differences exist in the tumor immune microenvironment between HPV-positive and HPV-negative penile squamous cell carcinoma, with HPV-positive tumors exhibiting lower PD-L1 expression and higher median tumor mutational burden.
Additionally, the HPV viral protein E7 can directly inhibit RB and p21, leading to the accumulation of p16, which is associated with better prognosis.6

According to the Global Cancer Observatory (GLOBOCAN), the incidence of penile cancer is highest in South America, Africa, and Southeast Asia it would be hard to conduct penile cancer trials in Europe or the United States. Similar trends were observed in data from the Global Society of Rare Genitourinary Tumors (GSRGT) survey, which highlighted significant geographical disparities in disease burden, with South America reporting the highest incidence. Risk factors positively associated with higher penile cancer incidence included alcohol consumption, human immunodeficiency virus (HIV) infection, and unsafe sexual practices.7
Notably, when comparing penile cancer incidence maps with HPV vaccination coverage for the first dose in males, vaccination rates have increased, particularly in North America and Europe. However, regions with the highest penile cancer incidence, such as South America, Africa, and Southeast Asia, still have low HPV vaccination coverage, highlighting a critical gap in preventive efforts.
Dr. Necchi highlighted a study evaluating the efficacy of quadrivalent HPV vaccination in males. Notably, HPV vaccination demonstrated efficacy against condylomata acuminata, with rates of 67.2% in the intention-to-treat population and 89.4% in the per-protocol population. However, its efficacy in preventing penile intraepithelial neoplasia (PeIN) and penile cancer requires further investigation.8
In a cohort study analyzing 397 penile squamous cell carcinoma cases, genomic alterations in over 300 cancer-associated genes and genomic signatures, including tumor mutational burden (TMB), were evaluated using hybrid capture-based comprehensive genomic profiling with FoundationOne and FoundationOne CDx assays. Significant biomarker differences were observed in nearly 15% of patients with a TMB of 10 mutations per megabase or higher, with human papillomavirus identification increasing as TMB rose. Notably, the study identified a distinct subgroup of advanced penile squamous cell carcinoma characterized by HPV positivity, high TMB, and PIK3CA/KMT2D mutations, warranting further clinical investigation.9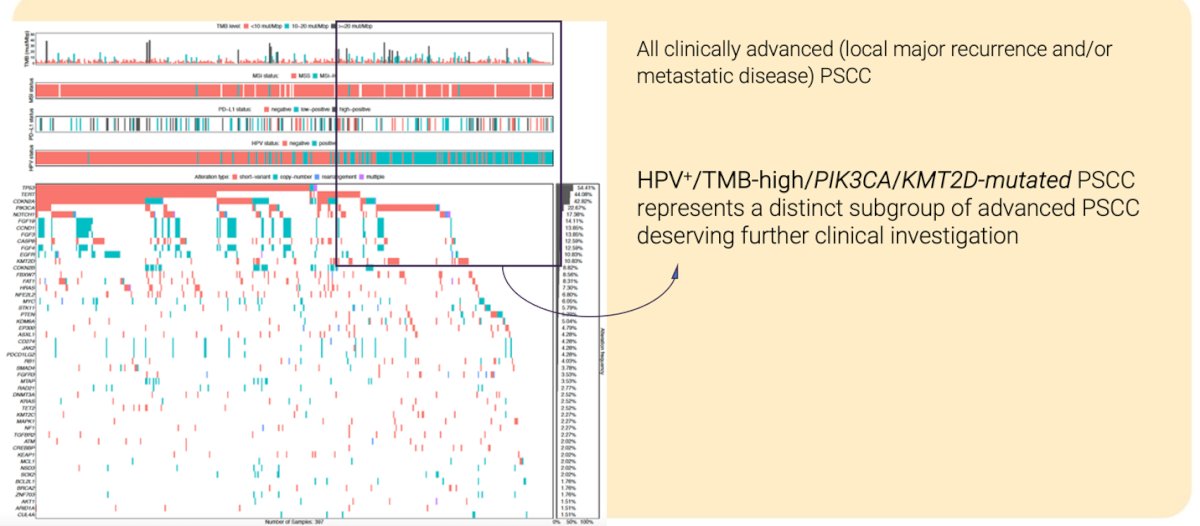
The use of immunotherapy in HPV-unselected penile cancer patients has increased in recent years, with overall response rates ranging from 13% to 44%. In 2018, the FDA approved cemiplimab for cutaneous squamous cell carcinoma, which may serve as a standard therapy option in the post-chemotherapy setting. Additional real-world and retrospective data from the FMI-Flatiron Health Database and Chinese cohorts support these findings. Early results from neoadjuvant trials indicate a potential for pathologic complete response (pCR) rates up to 61% with combination therapy involving EGFR inhibitors, PD-L1 inhibitors, and chemotherapy. Furthermore, ongoing research into therapeutic vaccines and T-cell therapies for HPV-positive cancers holds promise for future treatment strategies.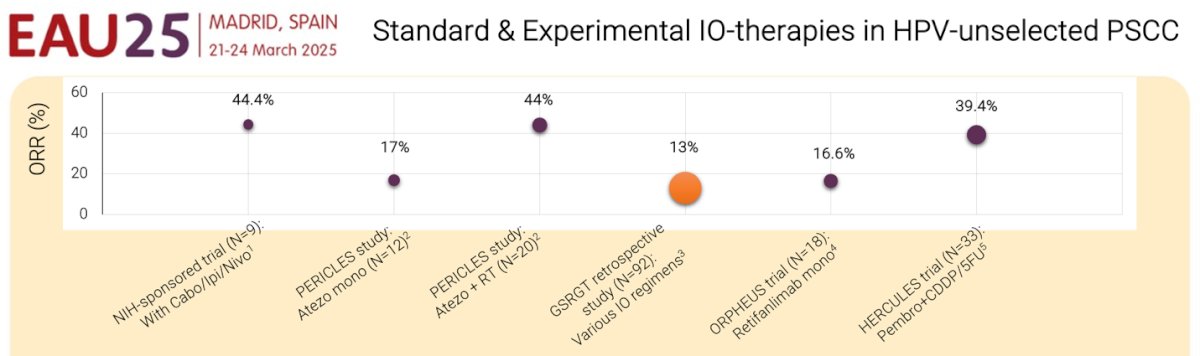
Dr. Necchi concluded his presentation with the following remarks:
- The EAU/ASCO Guidelines and retrospective studies endorse the use of neoadjuvant chemotherapy for unresectable or recurrent lymph node metastases (cN3) and selected cN2 patients after thorough discussion
- Chemo-IO may be an alternative option to TIP (in biomarker-selected patients) in the future
- Basket trials including penile squamous cell carcinoma patients are needed in the post-chemotherapy setting
- We should start thinking of penile cancer as multiple distinct biological entities
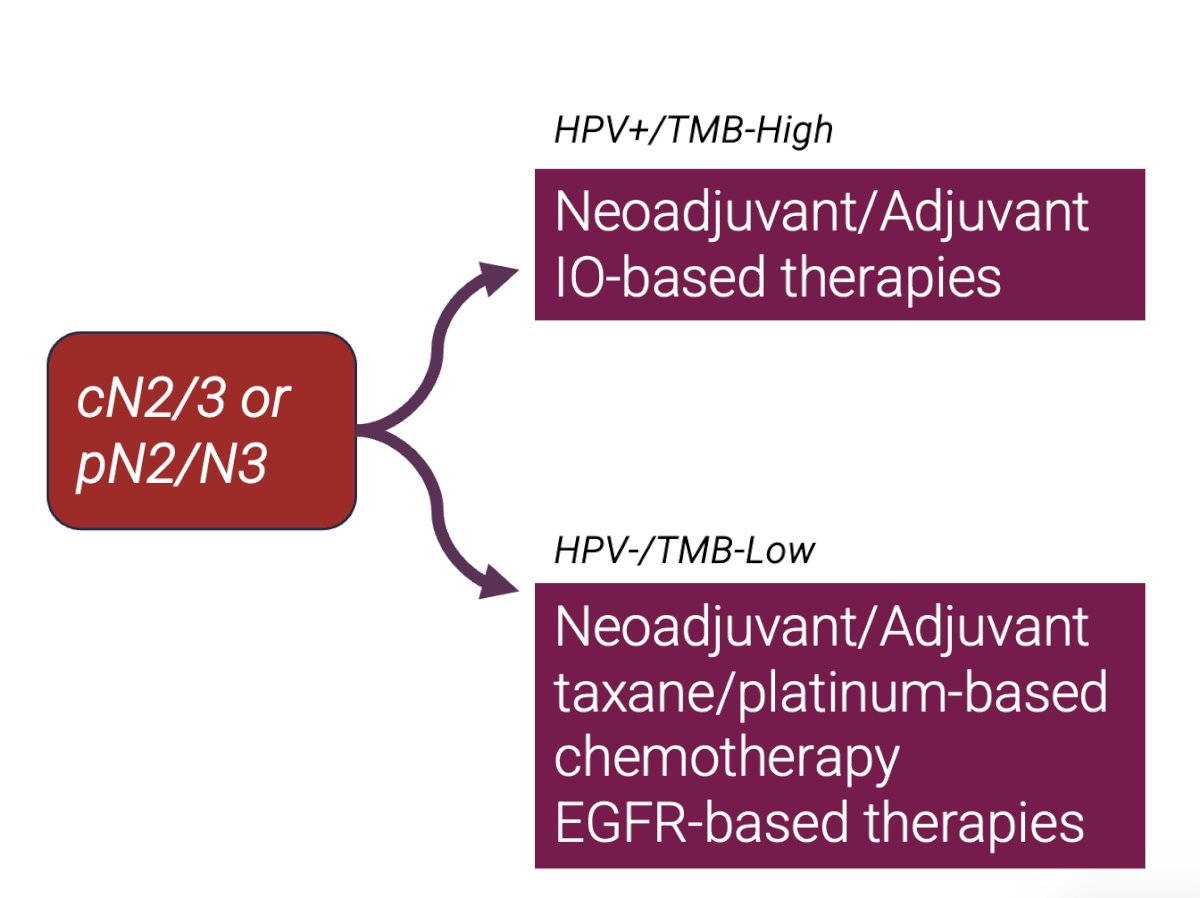
- TMB-high/HPV+ penile squamous cell carcinoma patients will deserve next-generation ICI therapy-based trials such as the proposed algorithm below
Presented by: Andrea Necchi, MD, Medical Oncologist, Professor of Oncology, Vita-Salute San Raffaele University, Chief of Genitourinary, Medical Oncology, Fondazione IRCCS Instituto Nazionale dei Tumori, IRCCS San Raffaele Hospital and Scientific Institute, Milan, Italy
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain between March 21st and 24th 2025
References:
- Joshi SS, Handorf E, Strauss D, Correa AF, Kutikov A, Chen DYT, Viterbo R, Greenberg RE, Uzzo RG, Smaldone MC, Geynisman DM. Treatment Trends and Outcomes for Patients With Lymph Node-Positive Cancer of the Penis. JAMA Oncol. 2018 May 1;4(5):643-649. doi: 10.1001/jamaoncol.2017.5608. PMID: 29494739; PMCID: PMC5885184.
- EAU-ASCO Penile Cancer Guidelines. Edn. presented at the EAU Annual Congress Milan 2023. ISBN 978-94-92671-19-6
- Muneer A, Bandini M, Compérat E, De Meerleer G, Fizazi K, Gietema J, Gillessen S, Kirkham A, Sangar V, Alifrangis C, Powles T; ESMO Guidelines Committee. Electronic address: . Penile cancer: ESMO-EURACAN Clinical Practice Guideline for diagnosis, treatment and follow-up. ESMO Open. 2024 Jul;9(7):103481. doi: 10.1016/j.esmoop.2024.103481. Epub 2024 Jul 11. PMID: 39089768; PMCID: PMC11360427.
- Pagliaro LC et al, Neoadjuvant Paclitaxel, Ifosfamide, and Cisplatin Chemotherapy for Metastatic Penile Cancer: A Phase II Study. J Clin Oncol. 2010;28(24):3851-7
- Azizi M, et al. J Urol. 2020 Jun;203(6):1147-1155
- Holzbeierlein JM, Spiess PE. Advances in Penile and Testicular Cancer: Promising Horizons in Clinical Care. Urol Clin North Am. 2024 Aug;51(3):xv-xvi. doi: 10.1016/j.ucl.2024.05.001. Epub 2024 May 14. PMID: 38925747.
- Huang J, Chan SC, Pang WS, Liu X, Zhang L, Lucero-Prisno DE 3rd, Xu W, Zheng ZJ, Ng AC, Necchi A, Spiess PE, Teoh JY, Wong MCS; Global Society of Rare Genitourinary Tumors (GSRGT). Incidence, risk factors, and temporal trends of penile cancer: a global population-based study. BJU Int. 2024 Mar;133(3):314-323. doi: 10.1111/bju.16224. Epub 2023 Dec 1. PMID: 37953505.
- Giuliano AR, Palefsky JM, Goldstone S, Moreira ED Jr, Penny ME, Aranda C, Vardas E, Moi H, Jessen H, Hillman R, Chang YH, Ferris D, Rouleau D, Bryan J, Marshall JB, Vuocolo S, Barr E, Radley D, Haupt RM, Guris D. Efficacy of quadrivalent HPV vaccine against HPV Infection and disease in males. N Engl J Med. 2011 Feb 3;364(5):401-11. doi: 10.1056/NEJMoa0909537. Erratum in: N Engl J Med. 2011 Apr 14;364(15):1481. PMID: 21288094; PMCID: PMC3495065.
- Necchi A, Spiess PE, Costa de Padua T, Li R, Grivas P, Huang RSP, Lin DI, Danziger N, Ross JS, Jacob JM, Sager RA, Basnet A, Li G, Graf RP, Pavlick DC, Bratslavsky G. Genomic Profiles and Clinical Outcomes of Penile Squamous Cell Carcinoma With Elevated Tumor Mutational Burden. JAMA Netw Open. 2023 Dec 1;6(12):e2348002. doi: 10.1001/jamanetworkopen.2023.48002. PMID: 38150257; PMCID: PMC10753400.