(UroToday.com) The 2025 European Association of Urology (EAU) Annual Congress held in Madrid, Spain between March 21st and 24th 2025, was host to a thematic session on hot topics in the management of renal cell carcinoma (RCC) patients. Dr. Geraldine Pignot discussed the need for new approaches to the risk stratification of patients with metastatic RCC (mRCC).
Dr. Pignot noted that accurate, reliable risk stratification for mRCC remains a real challenge. Optimal risk stratification is important for practicing oncologists to predict survival and optimize patient treatment selection. This is becoming increasingly important in mRCC, given that there have been several recently approved treatments with distinct targets, including immune checkpoints inhibitors. There remains room for improvement for identifying patients with poorer prognosis, and those who will or will not respond to systemic treatment
What risk stratification models are currently available? The MSKCC/Motzer criteria were developed in the cytokine era in 1991. This prognostic model was initially developed in the 1st line context among patients receiving interferon or interleukin. There are five factors in the model as summarized below:1
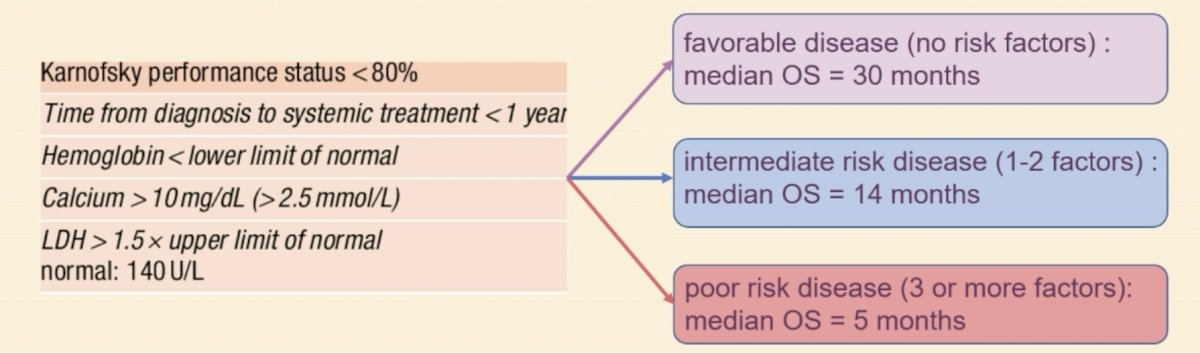
The IMDC/Heng criteria were developed in the vascular endothelial growth factor receptor inhibitor (VEGFRi) era. Currently, the IMDC criteria are more commonly used in research and clinical practice, compared to the MSKCC criteria. This model divides patients into favorable, intermediate, and poor risk groups, according to six prognostic factors:2
The IMDC criteria are the gold standard for risk-stratifying patients with mRCC. Currently, all evidence-based recommendations for systemic treatment are based on Heng’s/IMDC risk group stratification. However, does this still make sense in the immune checkpoint inhibitor era?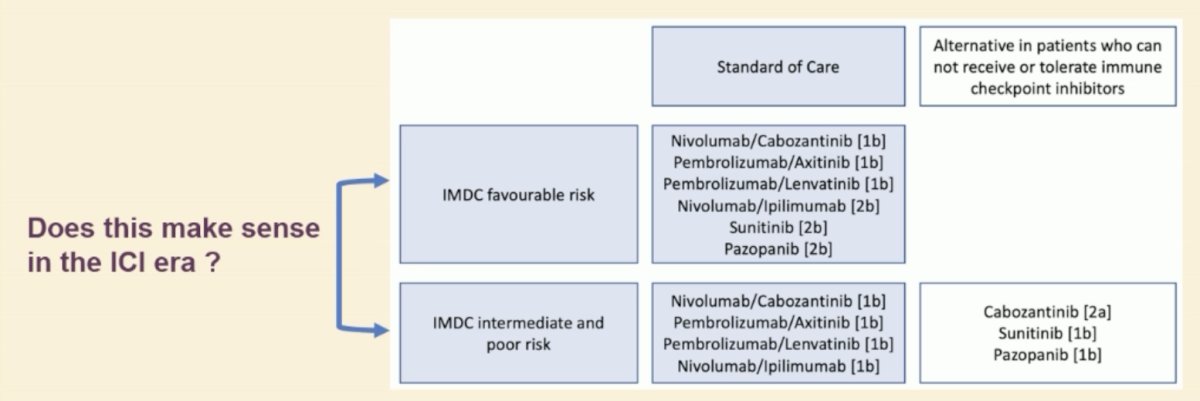
Dr. Pignot argued that the inconsistency observed in the trials of 1st line therapy for mRCC suggests that that may not be the case. As seen below for the CheckMate 214 and CheckMate 9ER trials, there are inconsistent results within the favorable risk groups with regard to treatment benefits with novel IO–IO/IO–TKI combination therapies, compared to sunitinib.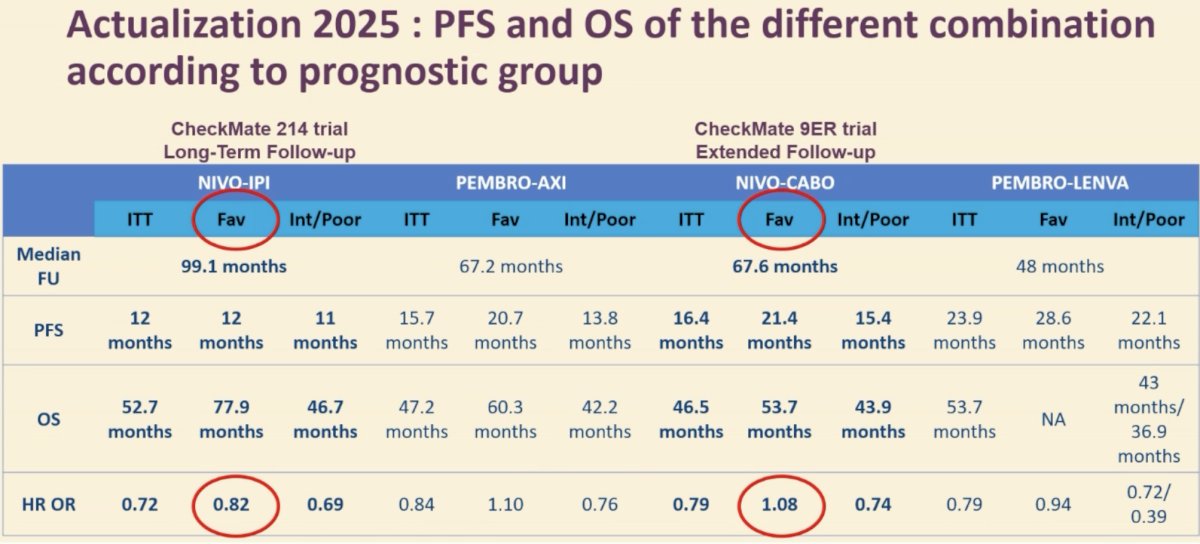
Dr. Pignot argued that in the immune checkpoint inhibitor era, we need updated, more accurate models that potentially incorporate:
- Additional clinical factors
- Molecular biomarkers
- Genetic signatures
- Artificial intelligence models
What are some possible additional clinical factors that could be incorporated?
- Number of metastases
- Sites of metastases: Both liver and bone metastases are poor prognostic factors in patients treated with immune checkpoint inhibitors
- Significantly, the tumor microenvironment differs significantly between metastatic sites and influences responses to immunotherapy
- Thus, sites of metastatic disease likely influence responses to immune checkpoint inhibitors
- Significantly, the tumor microenvironment differs significantly between metastatic sites and influences responses to immunotherapy
What are some novel biological risk factors that could be incorporated?
- Alkaline phosphatase
- Elevated C-reactive protein (CRP)
- Increased neutrophil-to-lymphocyte ratio
- All three factors are associated with poor outcomes in patients treated with immunotherapy
- Increased BMI may be protective in mRCC patients
- Obesity has been shown to alter fatty acid metabolism, which plays a role in both oncogenesis and responses to immunotherapy
Importantly, we need to move from prognostic to predictive factors. A prognostic biomarker informs about the risk of evolution of the cancer (i.e. cancer recurrence, disease progression or death), regardless of the treatment received. Conversely, a predictive marker ideally allows to identify patients in whom the treatment would be effective or not (responder/non-responder patients). This could impact the choice of treatment strategy, which is particularly significant in the immune checkpoint inhibitor era, where numerous 1st line treatment options are available.
What about histologic biomarkers? Sarcomatoid differentiation is associated with a poorer response to sunitinib, but better response to immune checkpoint inhibitor therapy.
Kidney Injury Molecule-1 (KIM-1) is a circulating protein plasma biomarker that, in localized disease, has been shown to be associated with:
- Worse disease-free survival independent of therapy received (i.e., prognostic)
- Improved outcomes with adjuvant immunotherapy post-nephrectomy (IMmotion 010/CheckMate 914; i.e., predictive)
In metastatic disease:
- High initial KIM-1 levels are associated with worse overall survival outcomes (i.e., prognostic)
- Early decreases in KIM-1 levels are associated with better progression-free survival with immunotherapy (CheckMate 214; i.e., predictive)

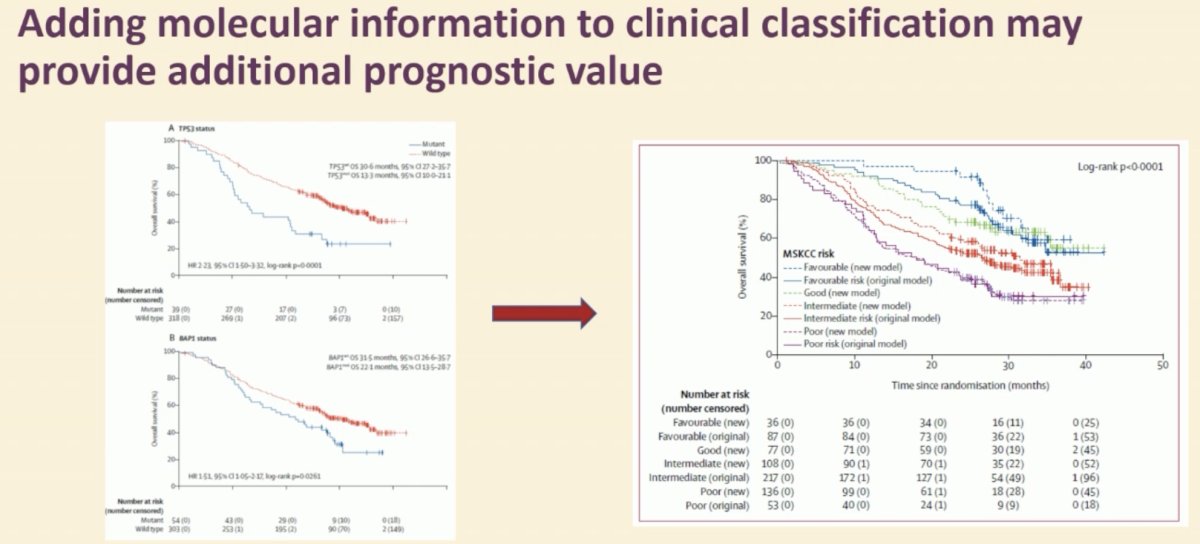
What about molecular biomarkers? Patient-specific molecular data suggest that patterns of response and resistance to VEGFRi and immunotherapy are innately different and depend on tumor biology. There is overlap between what the clinical characteristics used in IMDC risk stratification and genetic characteristics capture.
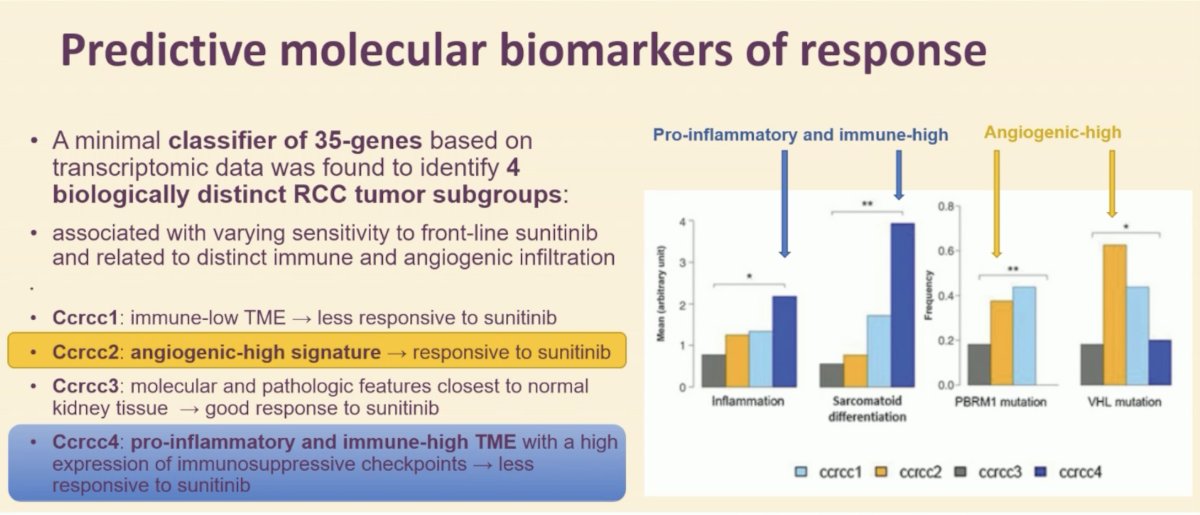
A minimal classifier of 35-genes based on transcriptomic data was found to identify four biologically distinct RCC tumor subgroups associated with varying sensitivity to front-line sunitinib and related to distinct immune and angiogenic infiltration:
- Ccrcc1: immune-low TME → less responsive to sunitinib
- Ccrcc2: angiogenic-high signature → responsive to sunitinib
- Сcrcc3: molecular and pathologic features closest to normal kidney tissue→ good response to sunitinib
- Ccrcc4: pro-inflammatory and immune-high TME with a high expression of immunosuppressive checkpoints → less responsive to sunitinib
BIONIKK is a French multicenter randomized non-comparative trial that randomized untreated mRCC patients according to their tumor molecular subgroup, defined on a frozen tumor sample. Patients with ccRCC1 and ccRCC4 tumors were randomized to receive nivolumab alone or nivolumab + ipilimumab, whereas patients with ccRCC2 and ccRCC3 tumors were randomized to receive nivolumab + ipilimumab or a TKI alone. 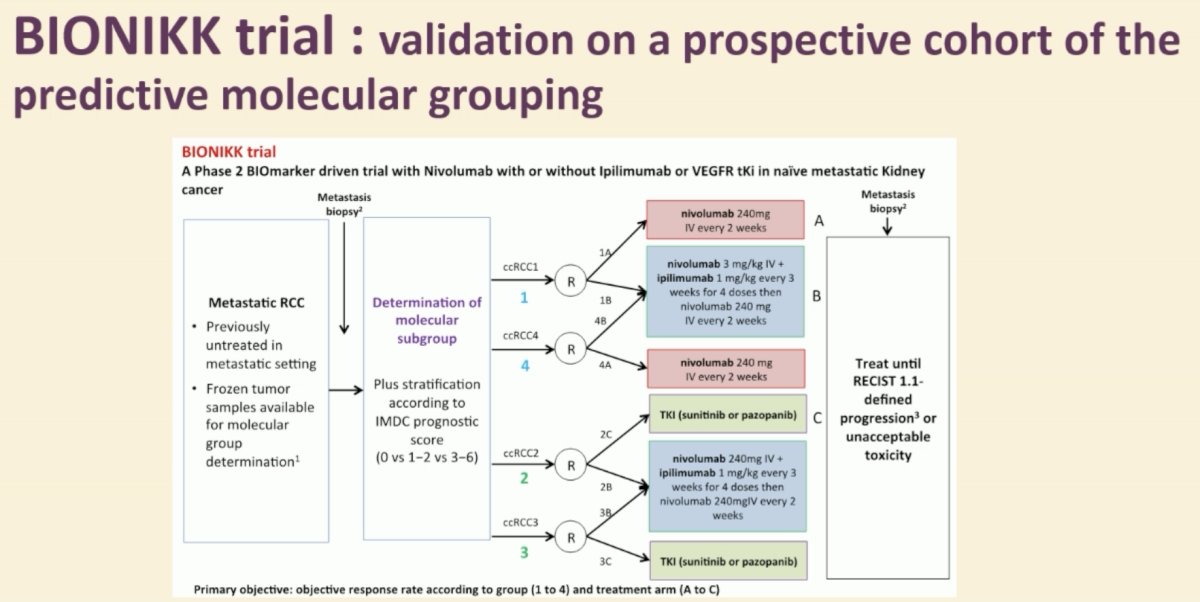
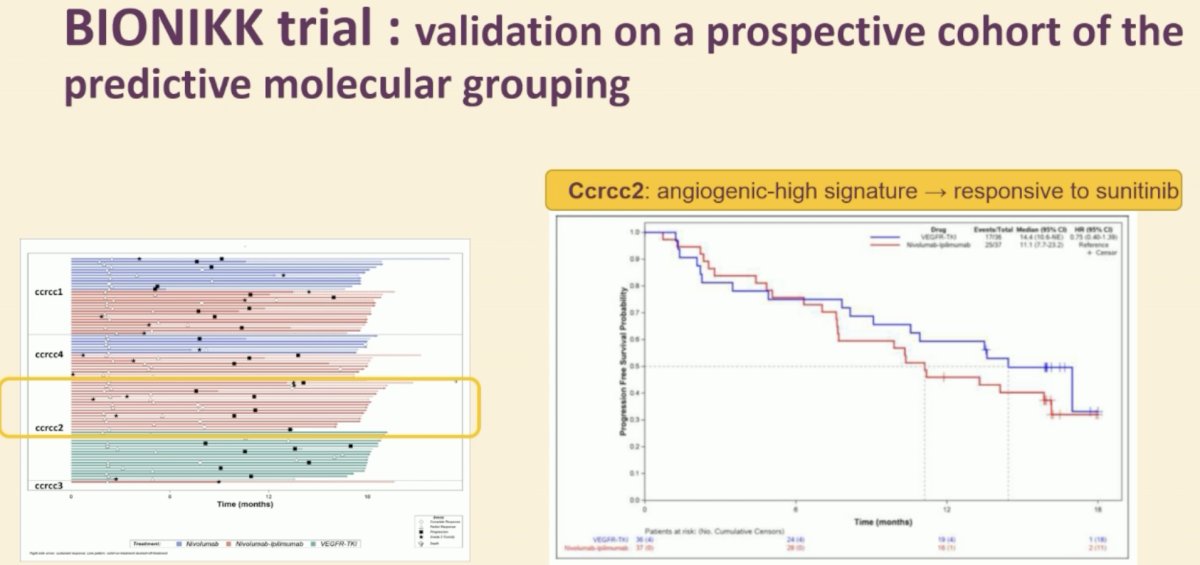
The main findings were as follows:7
- High efficacy of TKIs as well as nivolumab + ipilimumab in ccRCC2 tumors
- Higher efficacy of nivolumab +/- ipilimumab in ccRCC4 tumors, compared to ccRCC1.
Dr. Pignot concluded as follows:
- Risk stratification should be recognized as an ongoing, dynamic process.
- Therefore, updated prognostic models may be improved for patients treated with immune checkpoint inhibitors
- There have been efforts to integrate clinical variables, as well as molecular biomarkers.
- Risk-adapted therapy is necessary to optimally balance the efficacy and risks of systemic therapy, thus ensuring the best possible individual therapy.
Presented by: Geraldine Pignot, MD, PhD, Department of Surgical Oncology 2, Institut Paoli-Calmettes, Marseille, France
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 European Association of Urology (EAU) Annual Congress held in Madrid, Spain between March 21st and 24th, 2025
References:- Motzer R, Mazumdar M, Bacik J, Berg W, Amsterdam A, Ferrara J. Survival and prognostic stratification of 670 patients with advanced renal cell carcinoma. J Clin Oncol. 1999; 17(8): 2530-40.
- Heng DY, Xie W, Regan MM, et al. Prognostic factors for overall survival in patients with metastatic renal cell carcinoma treated with vascular endothelial growth factor-targeted agents: results from a large, multicenter study. J Clin Oncol. 2009; 27(34): 5794-9.
- Motzer RJ, Tannir NM, McDermott DF, et al. Nivolumab plus Ipilimumab versus Sunitinib in Advanced Renal-Cell Carcinoma. N Engl J Med 2018;378(14):1277-1290.
- Choueiri TK, Powles T, Burotto M, et al. Nivolumab plus cabozantinib versus sunitinib for advanced renal-cell carcinoma. N Engl J Med. 2021 Mar 4;384(9):829-841.
- Iacovelli R, Ciccarese C, Bria E, et al. Patients with sarcomatoid renal cell carcinoma - re-defining the first-line of treatment: A meta-analysis of randomised clinical trials with immune checkpoint inhibitors. Eur J Cancer. 2020; 136: 195-203.
- Motzer RJ, Banchereau R, Hamidi H, et al. Molecular Subsets in Renal Cancer Determine Outcome to Checkpoint and Angiogenesis Blockade. Cancer Cell. 2020; 38(6): 803-17.e4.
- Vano YA, Elaidi R, Bennamoun M, et al. Nivolumab, nivolumab-ipilimumab, and VEGFR-tyrosine kinase inhibitors as first-line treatment for metastatic clear-cell renal cell carcinoma (BIONIKK): a biomarker-driven, open-label, non-comparative, randomised, phase 2 trial. Lancet Oncol. 2022; 23(5): 612-24.