(UroToday.com) The 2025 European Association of Urology (EAU) Annual Congress held in Madrid, Spain, between March 21st and 24th, 2025, was host to a thematic session on hot topics in the management of renal cell carcinoma (RCC) patients. Drs. Anders Kjellman and Charles-Karim Bensalah debated whether patients with imaging findings suspicious for RCC should routinely undergo a renal mass biopsy (RMB).
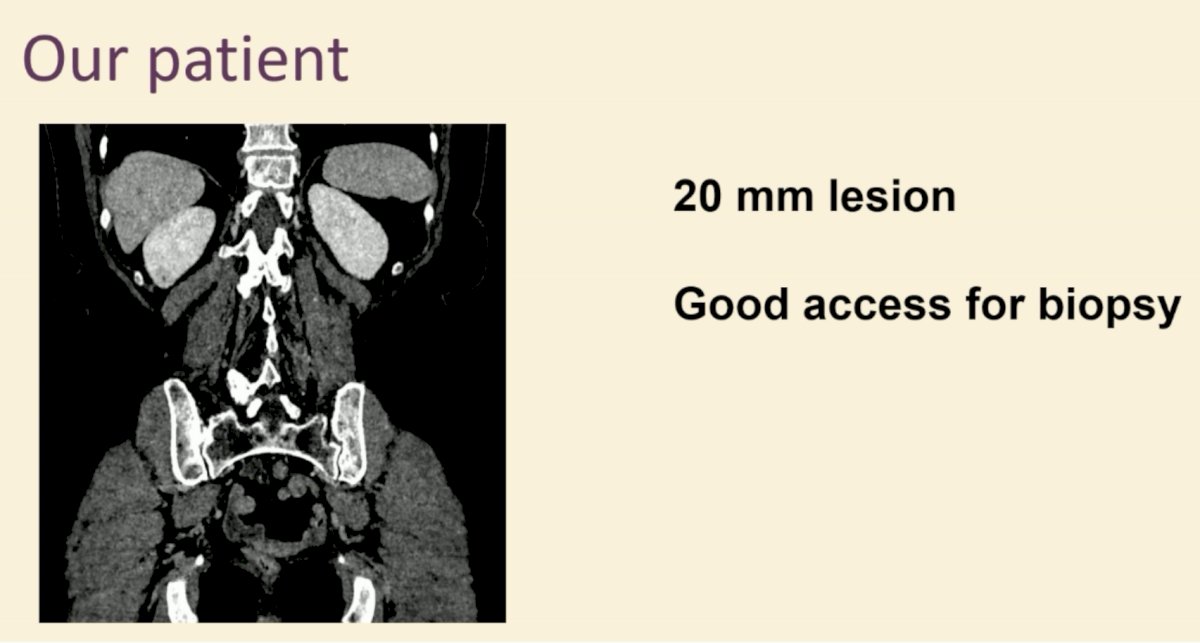
Dr. Gaelle Margue began the session with a case presentation of a 51-year-old female patient with a past medical history of hypertension, otherwise fit with an excellent performance status, who was incidentally found on a CT scan performed for abdominal pain to have a 2 cm right lower pole renal mass (RENAL Nephrometry score: 6p). The remainder of her work-up was negative with no other significant findings. Her blood work was unremarkable, with an eGFR of 96 ml/min.

Dr. Kjellman and Bensalah proceeded to debate whether this patient should undergo an RMB prior to possible intervention.
Dr. Kjellman began his argument in favor of a biopsy in this setting by highlighting that the EAU guidelines strongly recommend performing an RMB before ablative therapy and systemic therapy, in the absence of prior pathology. They note that RMBs offer additional information regarding optimal management, while potentially reducing the overtreatment of benign masses.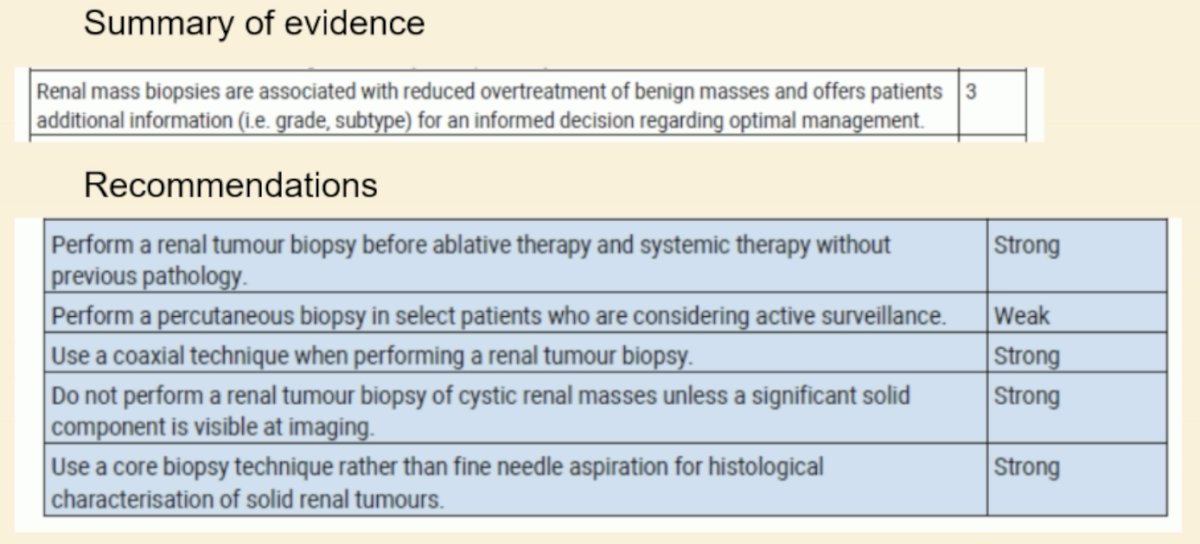
However, despite these recommendations, only a small proportion of patients with small renal masses ≤4 cm are biopsied prior to surgery. Notably, 20–30% of surgically removed small renal masses are benign,1 which highlights the potential issue of overtreatment of these masses.
In addition to 20-30% of such lesions being benign in nature, the probability of high-grade disease is low in tumors <4 cm, as demonstrated below.2 As such, given the significant likelihood of benign or low-grade disease, Dr. Kjellman argued that if a biopsy is performed, many of these patients would be candidates for surveillance.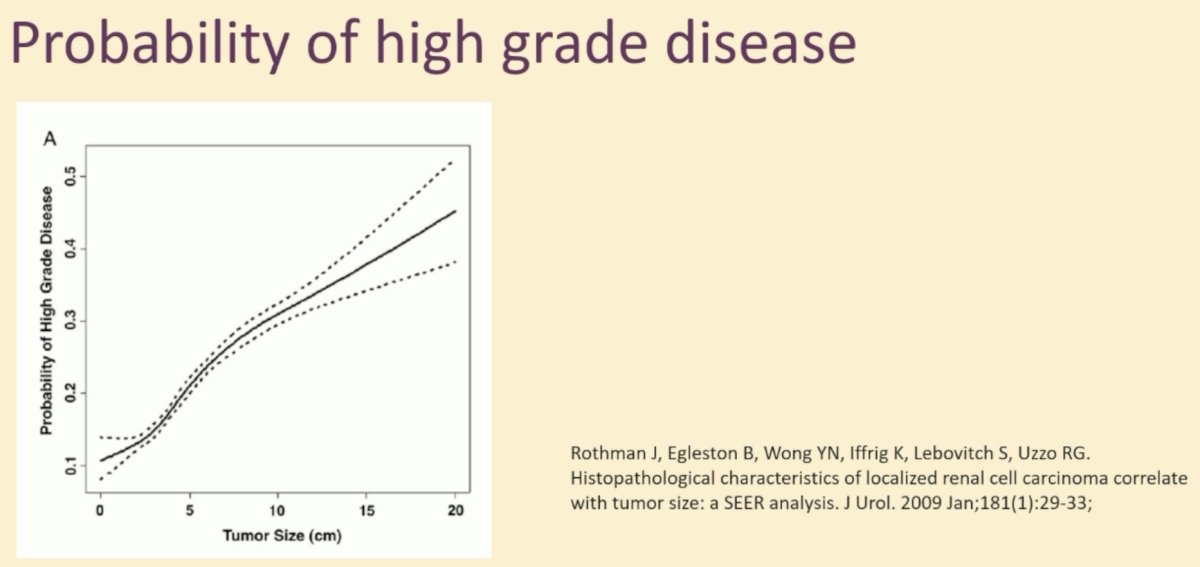
He argued that RMBs of small renal masses are:
- Accurate
- Safe
- Cost-effective
As demonstrated in the table below, RMBs have a sensitivity and specificity of 98% and 96%, respectively. Notably, however, the negative predictive value is only 69%, which means that 31% of patients with ‘negative’ RMBs harbor malignant masses.3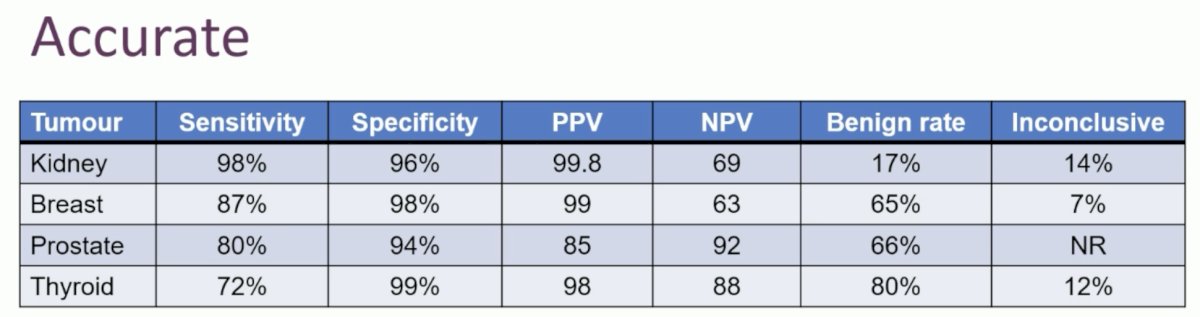
From a safety standpoint, RMBs have low risks of:
- Complications (hematoma, hematuria)
- Hospitalization (<1%)
- No cases of tumor seeding in modern series
From a financial standpoint, RMBs have been shown to be cost-effective, with a cost-utility study performed within the context of a Swedish health care system demonstrating that routinely performing RMBs would incur annual cost savings of 700 thousand Euros.4
What are the effects of increasing biopsy rates?5
- 87% conclusive diagnosis after biopsy
- 14% benign lesions detected (e.g., oncocytoma, angiomyolipoma)
- Less patients undergoing surgery or ablation
- More patients on active surveillance
- 3.2% benign resection rate (down from 20-30%)
Next, Dr. Bensalah argued against the utility of an RMB for this patient, noting that a RMB is not always ‘contributive’. A series of 1,594 patients undergoing RMBs published this year demonstrated that :6
- 9% are non-contributive
- RMBs accurately predict ISUP score and histologic subtype in 58% and 85% of cases, respectively.

The factors associated with a decreased diagnostic yield, include:
- Solitary kidney
- cT1a tumor
- Tumor size
The patient in the case presentation has a small, possibly cystic tumor, which Dr. Bensalah argued is likely to yield a non-diagnostic RMB.
Furthermore, RMBs are not ‘free of cost’. They are associated with increased rates of hospitalization, are invasive in nature, and are associated with complications in 8% of cases, overall, including hematomas and persistent lumbar pain in 8% and 4% of cases, respectively.
The other issue is that despite a benign finding on RMB, there is still a likelihood of underlying malignancy. In 2023, Branger et al. demonstrated in a series of 119 patients with findings of an ‘oncocytoma’ on RMB that only 68% of these patients are actually found to have an oncocytoma on the surgical specimen. 19% of these patients with an oncocytoma on RMB have underlying chromophobe carcinomas, and 7% have hybrid oncocytic/chromophobe tumors.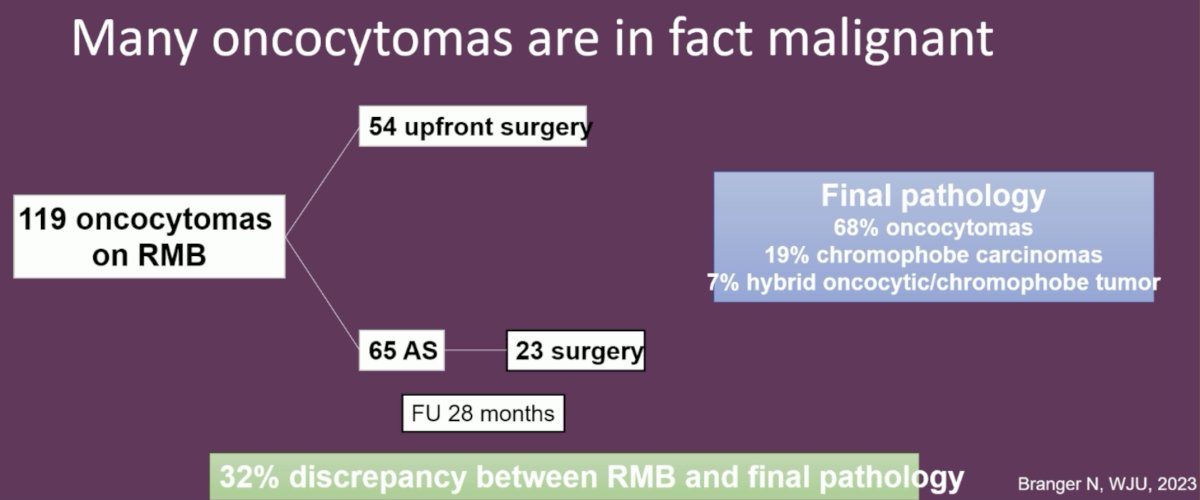
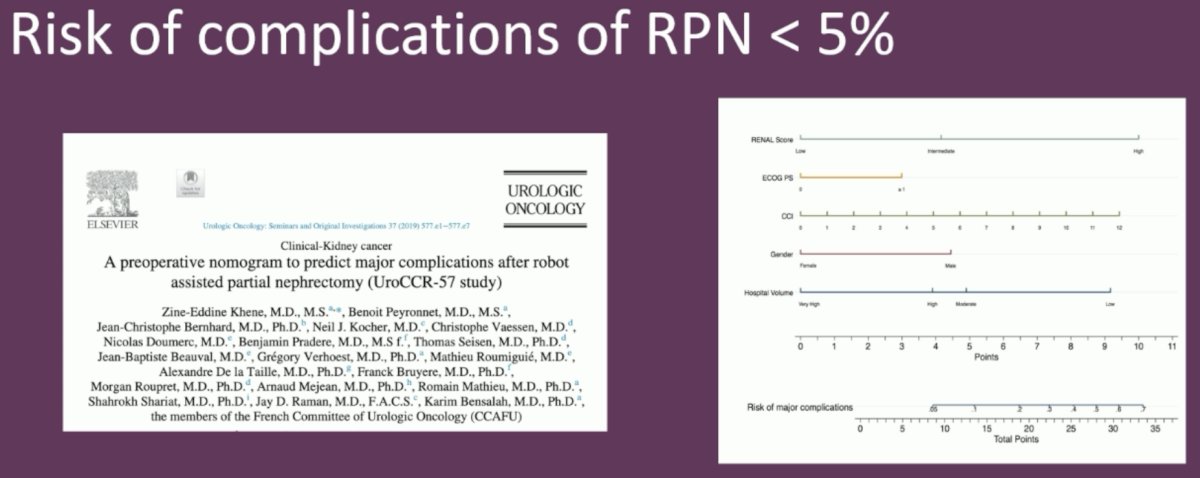
Irrespective of whether a RMB is performed, these patients have excellent long-term oncologic outcomes with robotic partial nephrectomies and have a low risk of complications (<5%). This suggests that further work-up with RMBs may be ‘redundant’ for these patients.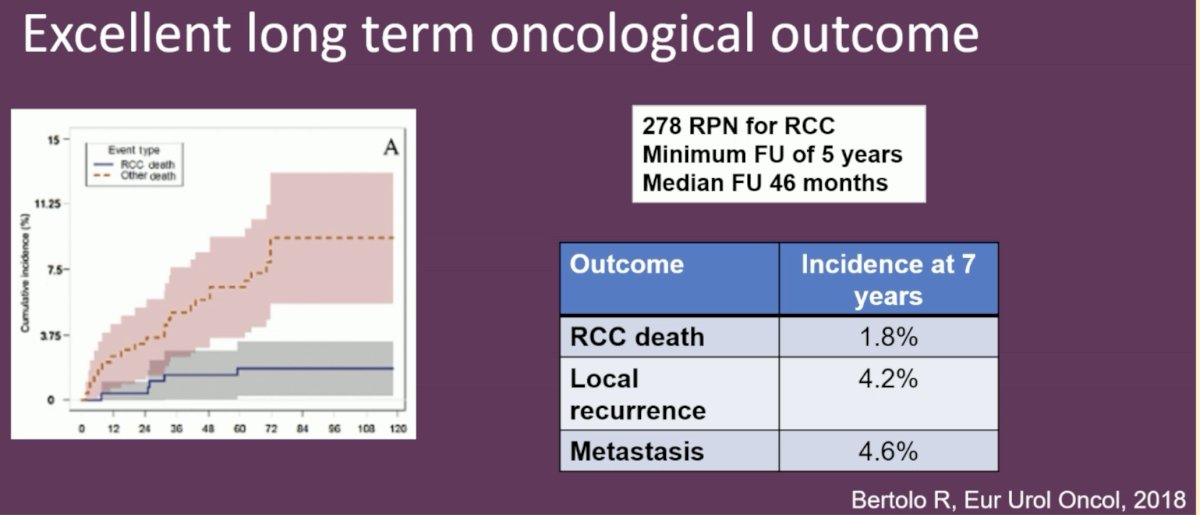
Additionally, robotic partial nephrectomies are being performed as outpatient surgeries at a number of high-volume centers, with reported 1-month complication and readmission rates of 1.2% only.
He noted that partial nephrectomies have very little to no impact on renal function, which further underlines the low morbidity of partial nephrectomies.
He concluded his presentation by arguing that this patient should undergo upfront surgery with a partial nephrectomy, which has low complication rates and avoids the unnecessary morbidity and anxiety associated with biopsy +/- surveillance.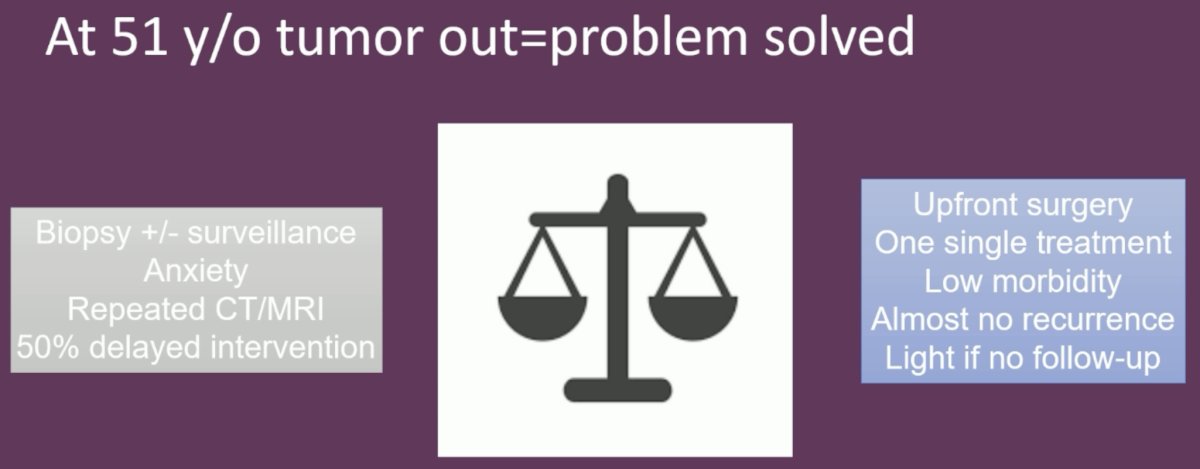
- Anders Kjellman, MD, PhD, Department of Clinical Science, Intervention and Technology, Karolinska Institute and Karolinska University Hospital, Stockholm, Sweden.
- Charles-Karim Bensalah, MD, PhD, Professor and Chairman, Centre Hospitalier Universitaire de Rennes, Rennes, France
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 European Association of Urology (EAU) Annual Congress held in Madrid, Spain between March 21st and 24th, 2025
References:
- Johnson DC, Vukina J, Smith AB, et al. Preoperatively misclassified, surgically removed benign renal masses: a systematic review of surgical series and United States population level burden estimate. J Urol. 2015; 193(1): 30-5.
- Rothman J, Egleston B, Wong YN, et al. Histopathological characteristics of localized renal cell carcinoma correlate with tumor size: a SEER analysis. J Urol. 2009; 181(1): 29-33.
- Gao B, Gorgen ARH, Bhatt, et al. Avoiding "Needless" nephrectomy: What is the role of small renal mass biopsy in 2024? Urol Oncol. 2024; 42(8): 236-44.
- Lind A, Hashim BM, Hagman M, et al. Healthcare costs in relation to increased use of preoperative renal tumour biopsies. Scand J Urol. 2025; 60: 66-72.
- Gao H, Nowroozizadeh B, Zepeda JP, et al. The success rate of small renal mass core needle biopsy and its impact on lowering benign resection rate. BMC Urol. 2023; 23(1): 189.
- Proye P, Gondran-Tellier B, Michel F, et al. Renal Mass Biopsy Prior to Surgical Excision: Practice, Diagnostic Performance, and Impact on Management in the UroCCR Registry (Ancillary Study No. 118). Eur Urol Open Sci. 2025; 60-7.
- Bernhard JC, Robert G, Ricard S, et al. Day-case robotic-assisted partial nephrectomy: feasibility and preliminary results of a prospective evaluation (UroCCR-25 AMBU-REIN study). World J Urol. 20222; 40: 1351-7.