(UroToday.com) The 2025 European Association of Urology (EAU) Annual Congress held in Madrid, Spain between March 21st and 24th 2025, was host to a thematic session on hot topics in the management of renal cell carcinoma (RCC) patients. Drs. Petrus Järvinen, Laurence Albiges, Cristina Suárez, and Dr. Ben Vanneste debated the optimal strategy for the management of recurrences after curative surgery for RCC: surgical resection, tyrosine kinase inhibitors (TKIs), immunotherapy, and radiotherapy.
Dr. Carlotta Palumbo began the session with a case presentation of a 66-year-old-male with a past medical history of hypertension and diabetes, who was incidentally found to have a left upper pole 3.5 cm renal mass (cT1aN0M0). His eGFR was 72 ml/min/1.73m2.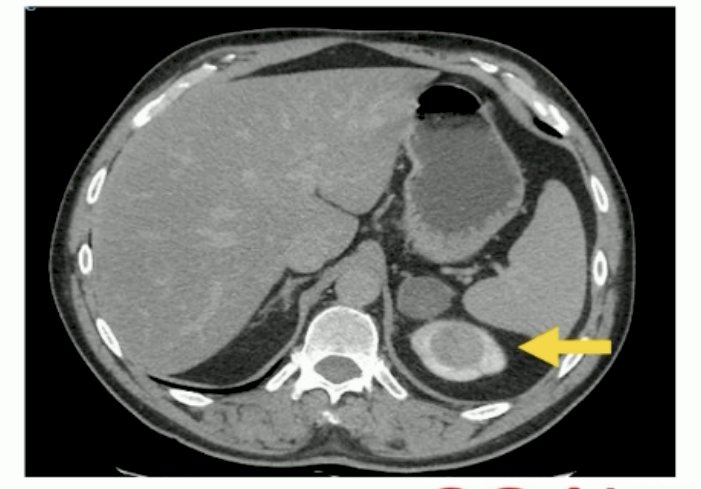
He underwent a robotic partial nephrectomy with enucleation of the mass with pathologic findings of pT1b clear cell RCC, Grade 4 (4.2 cm), with negative surgical margins.
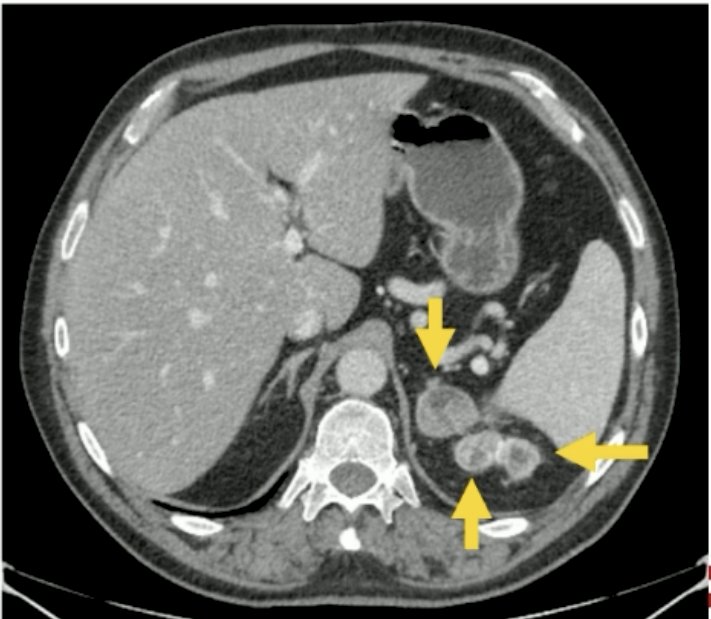
At one-year follow-up, the patient was found to have 2 masses in the upper pole of the left kidney with 1 metastatic site in the left adrenal gland. The eGFR at this point was 65 ml/min/1.73m2.
What is the best next step?
- Partial nephrectomy + adrenalectomy
- Radical nephrectomy + adrenalectomy
- Radiation therapy
- Systemic therapy
Dr. Petrus Järvinen argued in favor of surgical resection in this setting. He noted that radical surgical resection is the only known curative treatment for RCC, and this applies to both primary and recurrent disease. There is no evidence to suggest that other treatments, compared to radical surgery, cure more patients in this setting. Surgery for local recurrence after nephrectomy appears to be superior to systemic therapy.1
He emphasized that resection is the best treatment whenever complete resection is achievable. Retroperitoneal recurrences are ideally treated with surgical resection. This is particularly true for patients with a >2-year disease-free interval following primary surgery, who can achieve long-term disease-free survival with such an approach.
What are the outcomes for surgical resection in this setting? Retrospective series suggest that the 5- and 10-year overall survivals approach 60% and 32%, respectively. At a median follow-up of 48 months, approximately 33% are alive without evidence of disease recurrence. Poor prognostic factors in this setting include sarcomatoid features, positive margins, and high comorbid burden (Charlson ≥2).3,4
He acknowledged that surgery is likely not the correct choice in such a setting if the disease is unresectable or the interval between recurrence and primary surgery is very short. Otherwise, however, a complete metastasectomy for recurrence improves survival, compared to an incomplete or no resection. No biological factor is known to challenge radical surgery in the context of disease recurrence, despite advances in systemic therapy.3
What is the optimal surgical approach? There is no clear evidence, but both open and robotic approaches have been described. Maximizing the likelihood of a radical outcome should guide the approach choice, with positive margins at re-operation known to be associated with worse prognoses.
Another potential option is combining surgery with systemic therapy for patients with local recurrences to further improve on the outcomes with systemic therapy alone. To date, there is no evidence that immune checkpoint inhibitor combinations make surgery unnecessary in such a patient. He concluded his argument by noting that always consider surgery for recurrent disease, if complete resection is achievable.
Next, Dr. Ben Vanneste argued in favor of radiotherapy, namely stereotactic body radiotherapy (SBRT), in this setting. He highlighted recent data from the European RECUR registry that evaluated the role of local treatment of recurrences in patients with non-metastatic RCC. In 505 patients who experienced recurrence following treatment with curative intent for localized RCC, 97 underwent local treatment for their recurrence, and 79 did not. The median overall survival was 70.3 months versus 27.4 months, in favor of local recurrence treatment (p<0.001). This survival benefit was observed across all risk groups.4 He argued that these results strongly support the use of local therapy for the patient in the case example – but which modality is best: surgery or radiotherapy?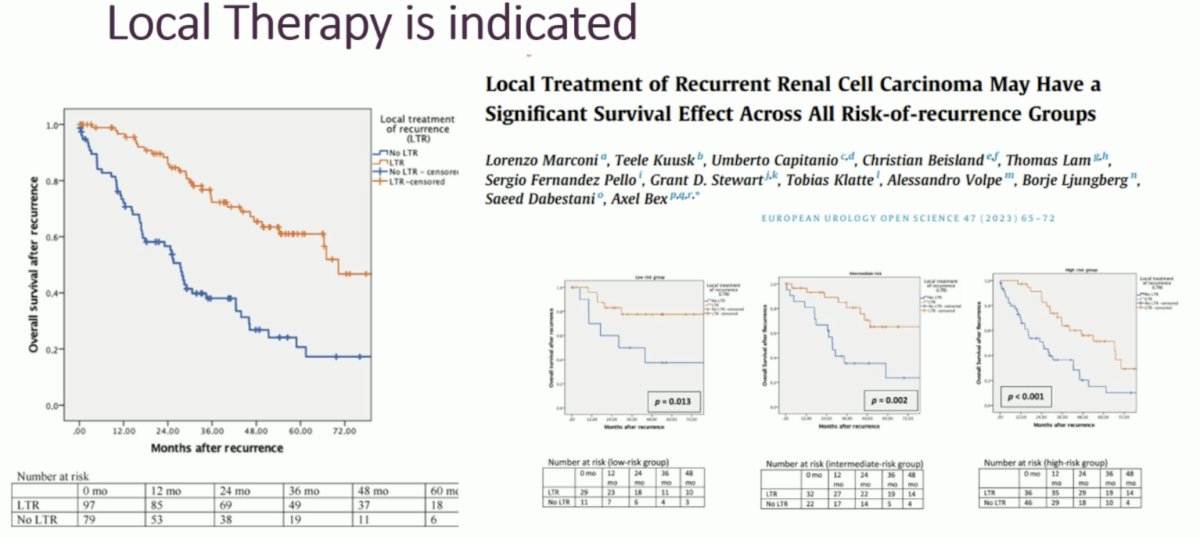
SBRT is an attractive option in this setting given that it is a non-invasive option that does not require general anesthesia and can be administered to large and peri-hilar tumors in the primary setting.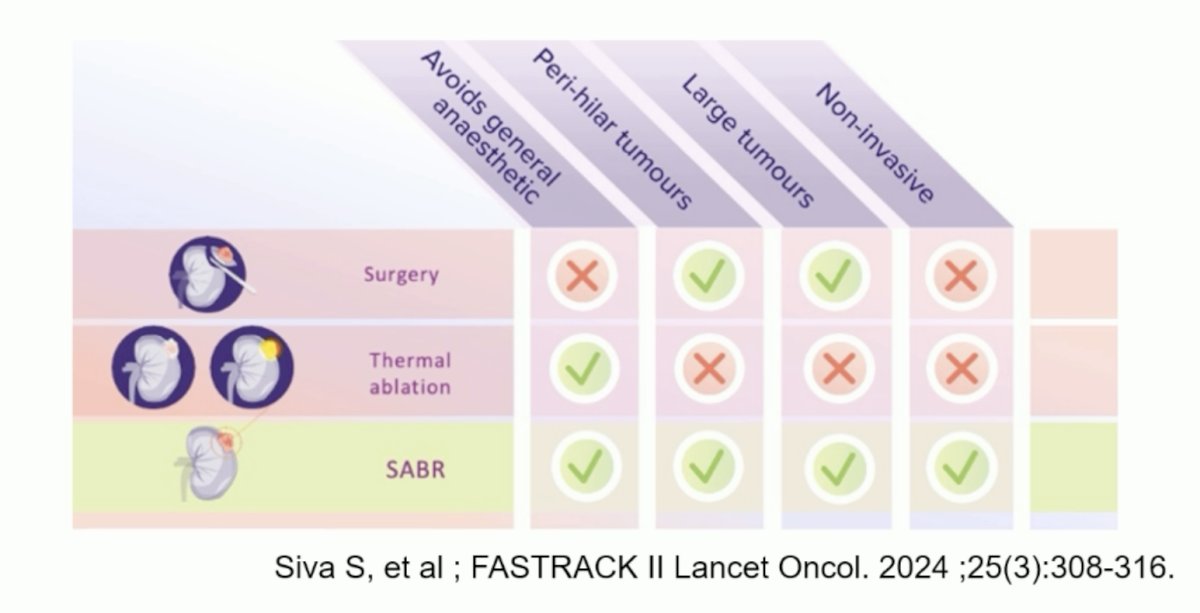
In the primary setting, the FASTRACK II phase II study evaluated SBRT (SABR) in 70 patients with a primary RCC who were medically inoperable, at high risk of complications from surgery or declined surgery. The median tumor size was 4.6 cm. At a median follow-up of 43 months, the 1-year local control rate was 100%, and the adverse event profile was favorable.5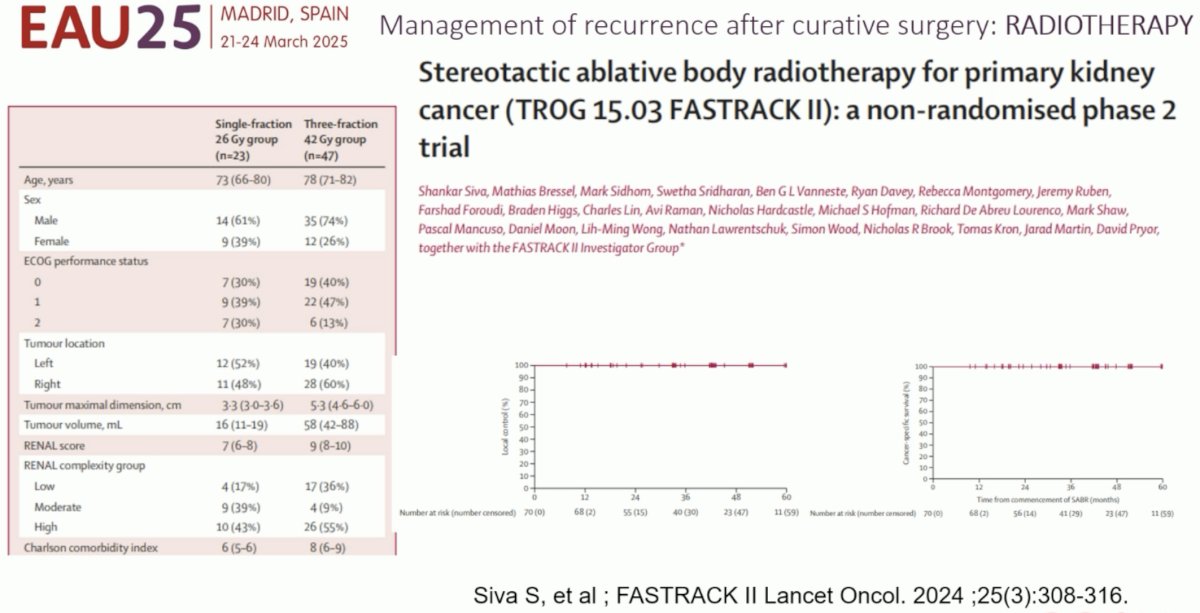
What about SBRT in the locoregional recurrence setting, such as the patient in the case presentation? In 2022, Liu et al. published a matched cohort analysis of 106 patients with local recurrence after radical nephrectomy, of whom 73 underwent local therapy and 33 received systemic therapy. In the local therapy group, 34 received surgery and 39 SBRT. Overall, patients in the systemic therapy group were more likely to have non-clear cell histology (64% versus 43%), T3-4 disease (70% versus 41%), and >5 lesions (30% versus 14%).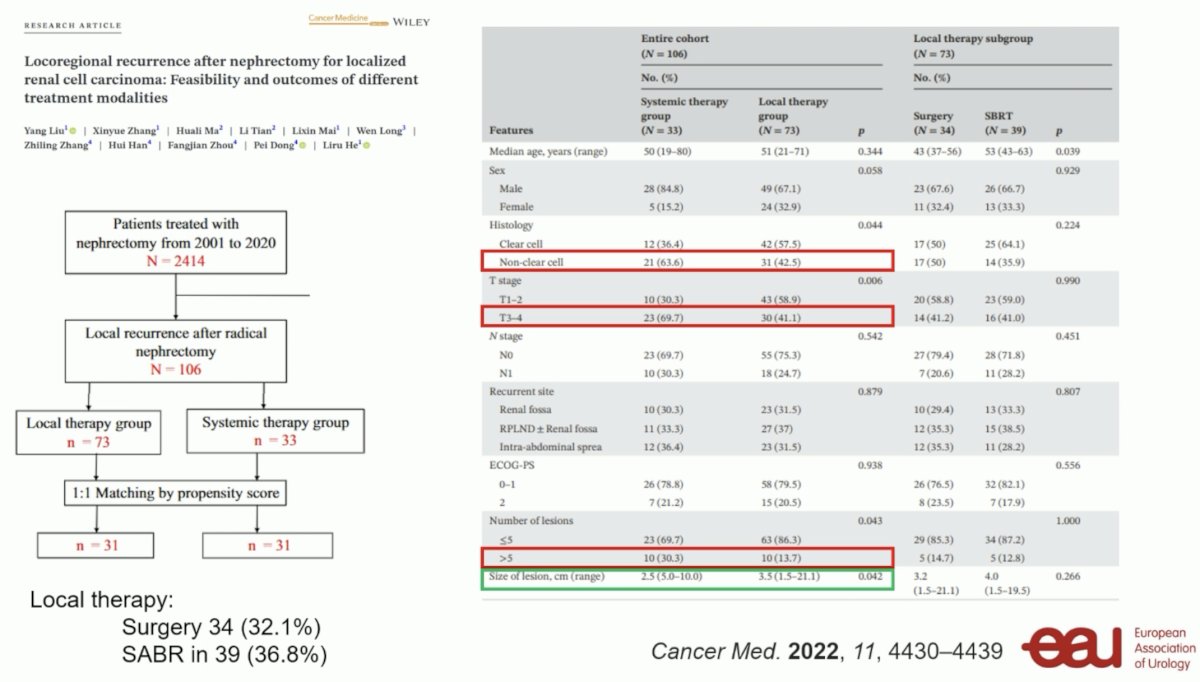
What did the results of this study show? A matched analysis demonstrated that patients who underwent local therapy had superior progression-free (PFS) and overall survivals (OS).6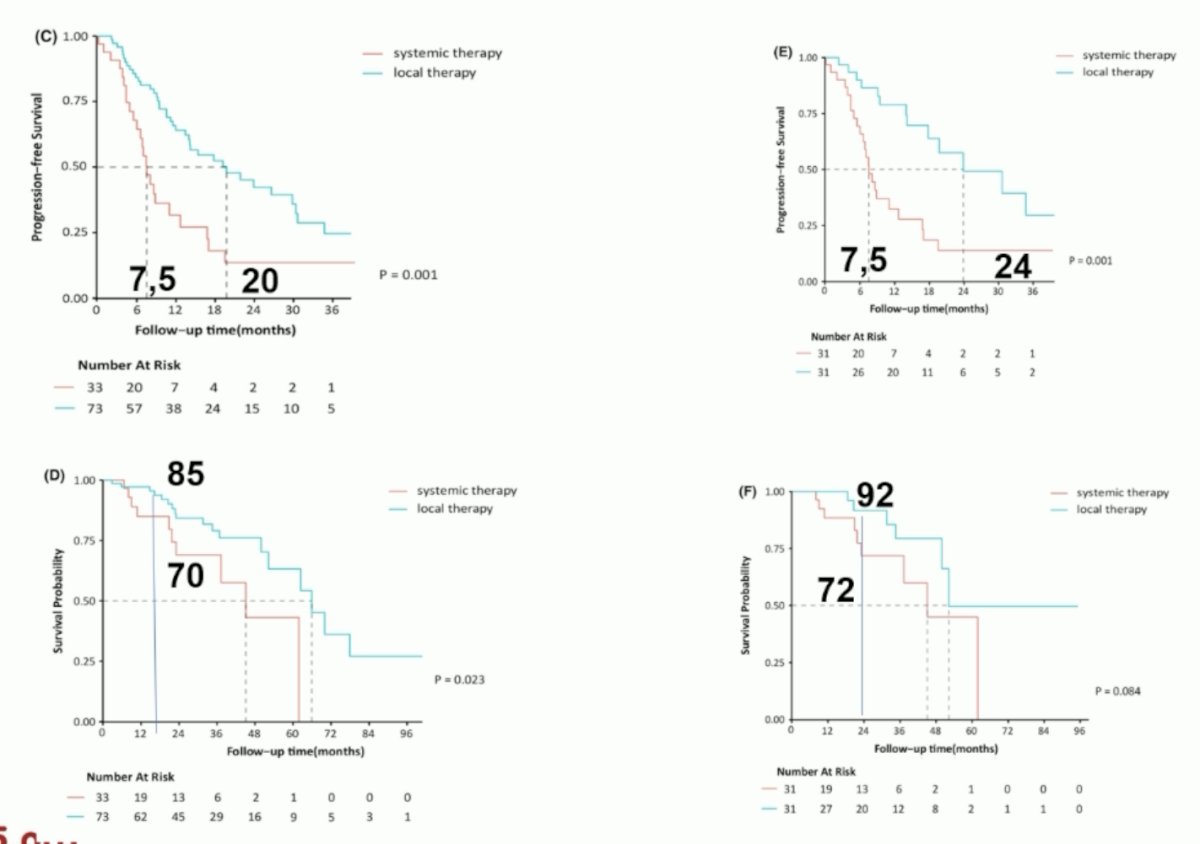
While patients who received SBRT may have had superior PFS compared to surgical excision (median: 22 versus 15 months), there was no difference in median OS (86 versus 83 months).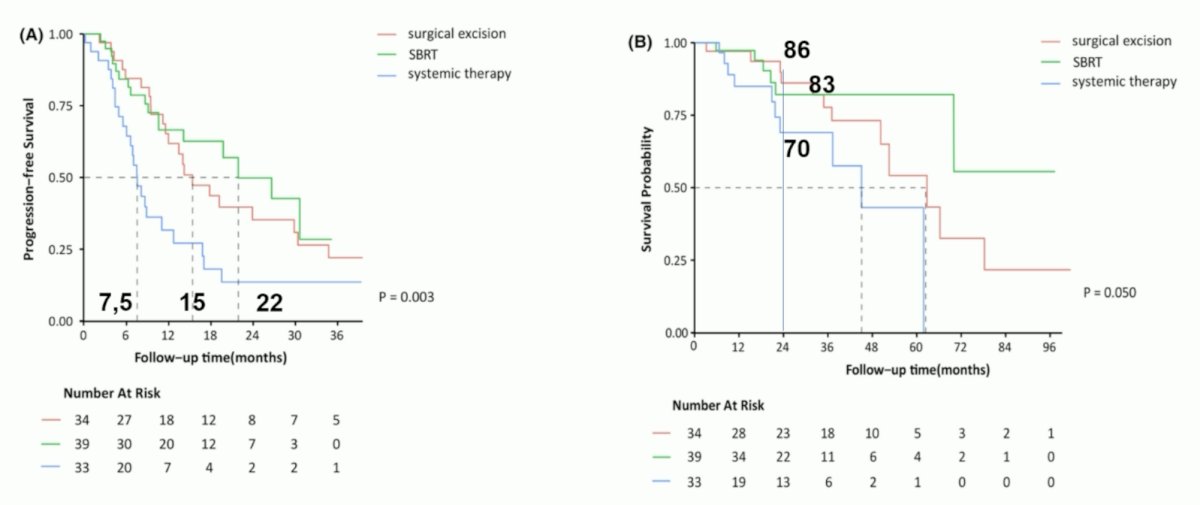
Notably, patients who underwent SBRT had lower rates of grade ≥2 toxicity, compared to those who underwent surgical resection.6
Based on these results, Dr. Vanneste argued that SABR could play a role in the salvage of local recurrences with a low toxicity profile and good local control.
The patient subsequently underwent a left laparoscopic radical nephrectomy, adrenalectomy, and splenectomy (due to bleeding) with findings of clear cell RCC pT3a (renal sinus fat invasion), pN0 (0/3), and G4 with negative surgical margins. The left adrenal gland and spleen were negative for malignancy.
A follow-up CT scan 6 months post-salvage resection demonstrated 2 enhancing masses in the abdominal wall and 1 nodule (15 mm) in the right lung. eGFR at this point was 43 ml/min/1.73m2.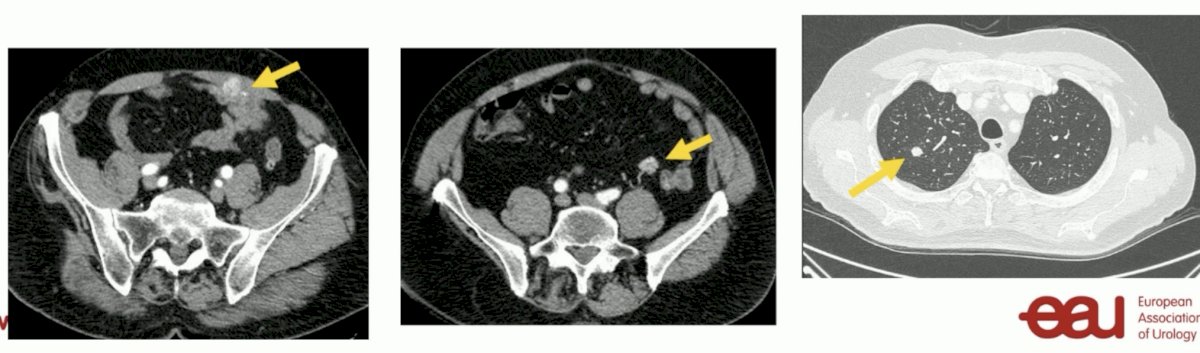
In September 2023, he was started on pembrolizumab (200 mg IV every 3 weeks) + axitinib 5 mg orally twice daily. Dr. Laurence Albiges next addressed the role of TKIs in this setting.
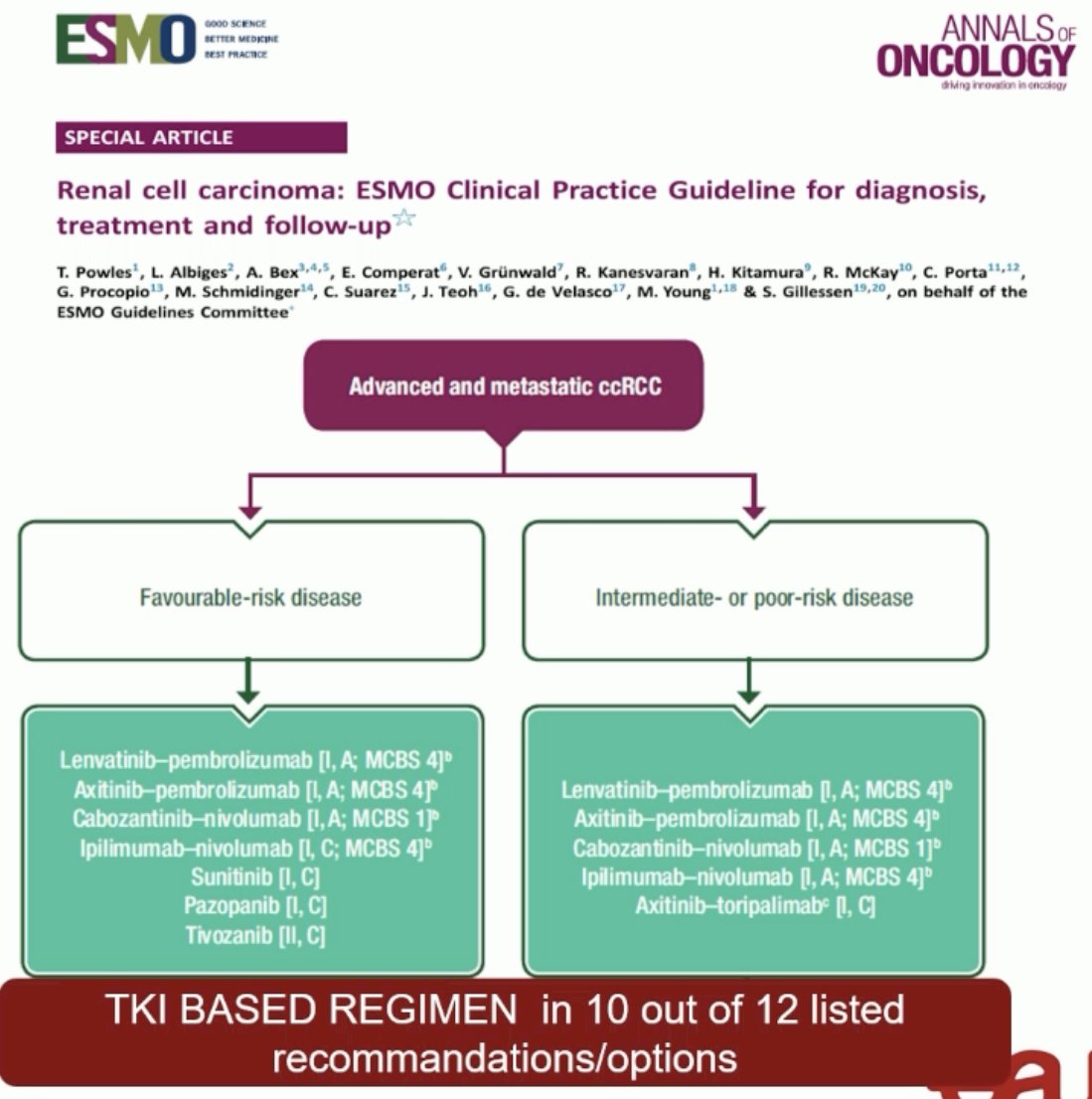
She began by emphasizing that there is rarely a role for single agent TKI therapy. As shown in the ESMO guidelines below, single agent TKIs (sunitinib, pazopanib, tivozanib) can be considered in select favorable risk patients only. All patients with intermediate- or poor-risk disease should receive IO-IO (ipilimumab + nivolumab) or IO+TKI combinations.
Summarized below are the four trials of 1st line standard-of-care combinations with proven overall survival benefits in the locally advanced/metastatic setting:7-10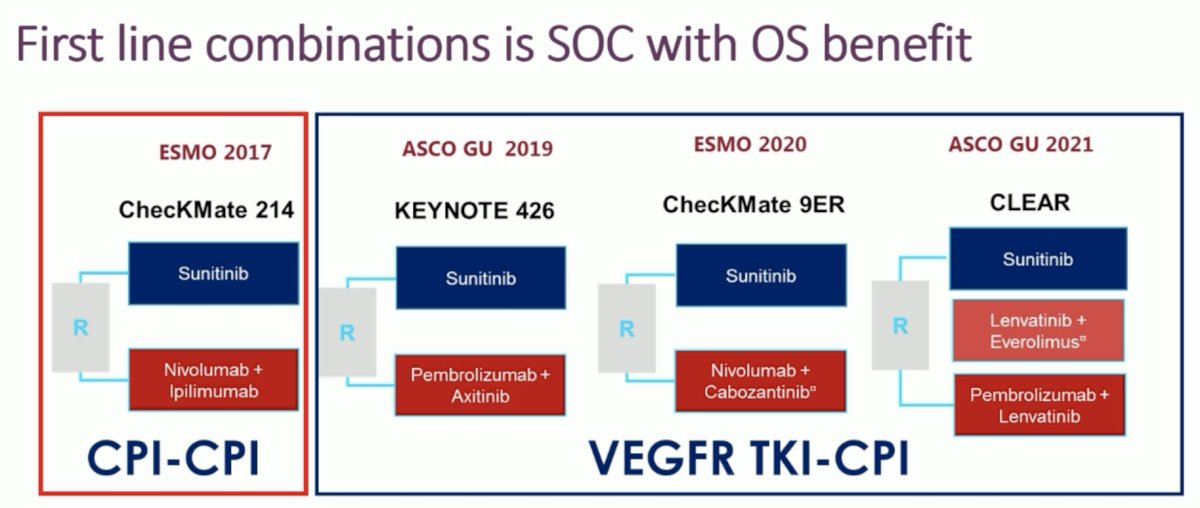
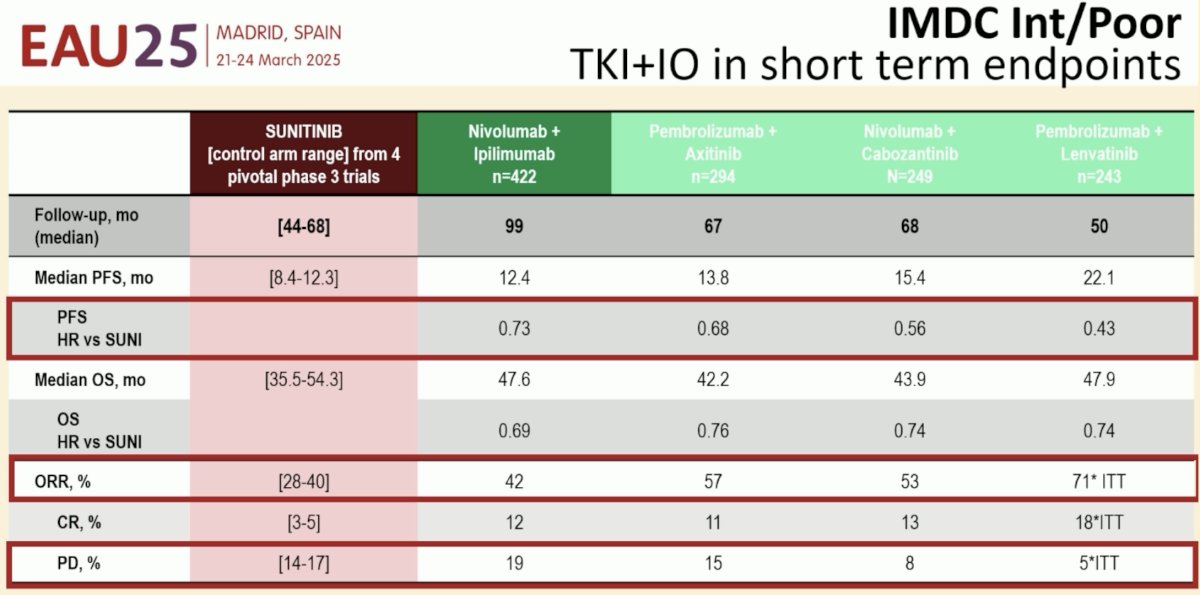
Compared to sunitinib (TKI monotherapy), these IO-IO and IO-TKI combinations have demonstrated improved:
- PFS: HRs 0.43–0.73
- Objective response rate (ORR): 42–71% versus 28–40%
- Progressive disease (PD): 5–19% versus 14–17%
- Overall survival: HRs 0.69–0.76
But which combination should we use? Several factors can guide this decision. First, if the pathology report demonstrates a significant sarcomatoid component, then IO-IO is likely the best option in this setting. If patients are highly symptomatic with poor performance status, then consider combinations with the lowest toxicity burden and consider using both an IO and a TKI, as these patients are less likely to tolerate 2nd line therapies. However, we clearly need better data to guide this decision. CARE-1 is a pragmatic clinical trial that is randomizing treatment-naïve clear cell metastatic intermediate/poor risk group RCC patients to either IO-IO or IO+TKI therapy, with randomization stratified by PD-L1 status: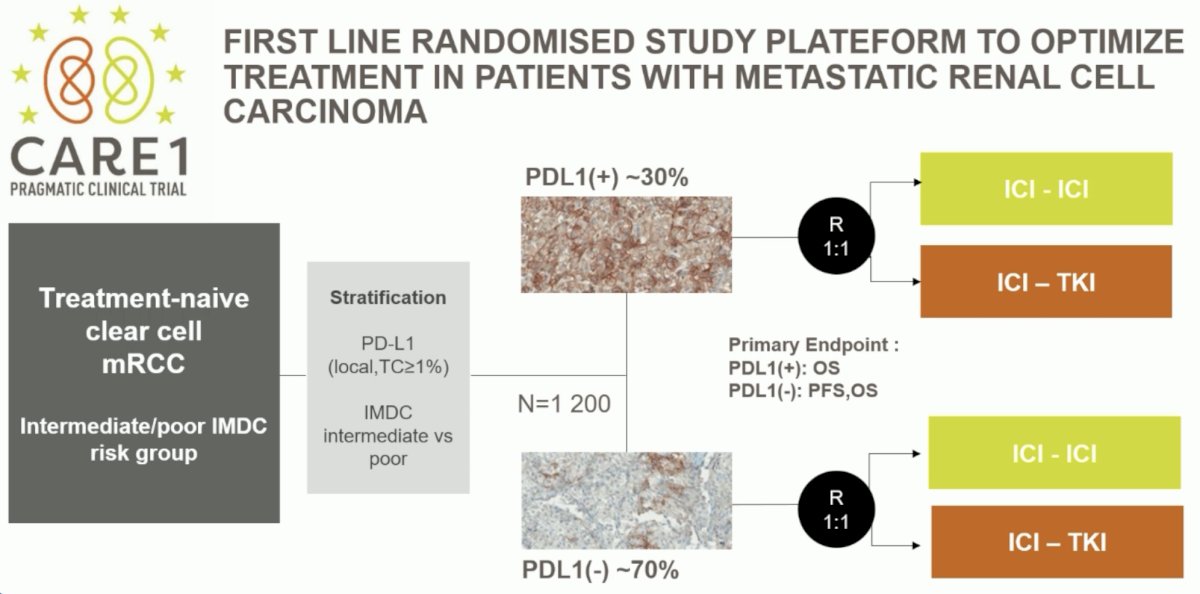
The rationale for stratifying randomization by PD-L1 status is that PD-L1 status is predictive of treatment response to IO-IO therapy, compared to sunitinib, as demonstrated below. Thus, it is hypothesized that PD-L1+ patients may derive a preferentially greater benefit from IO-IO combinations, compared to IO-TKI regimens.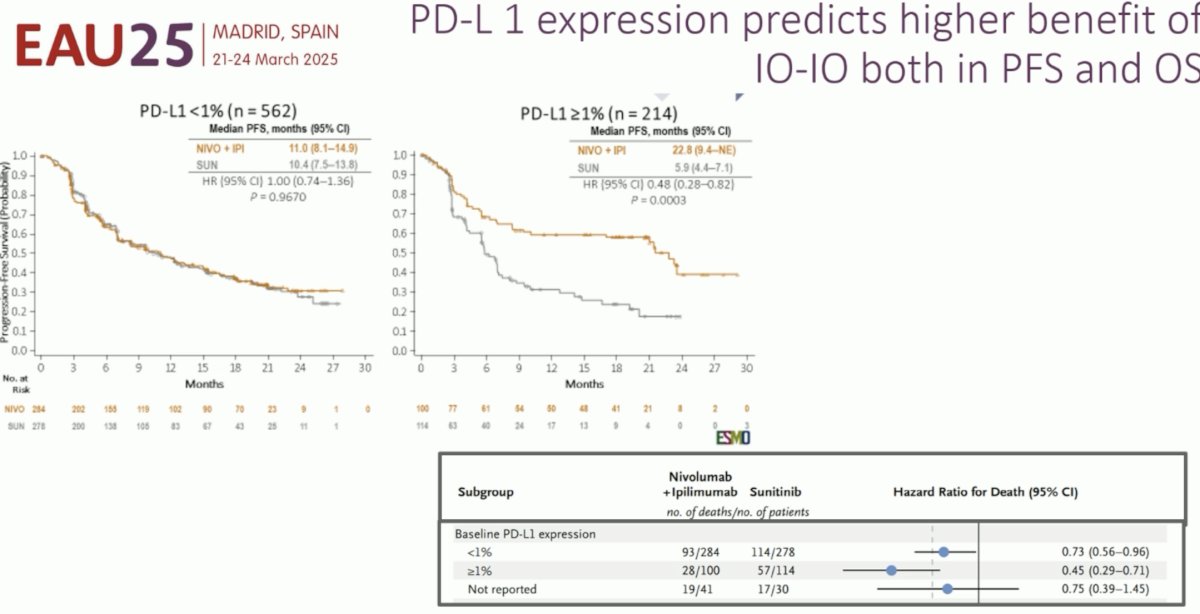
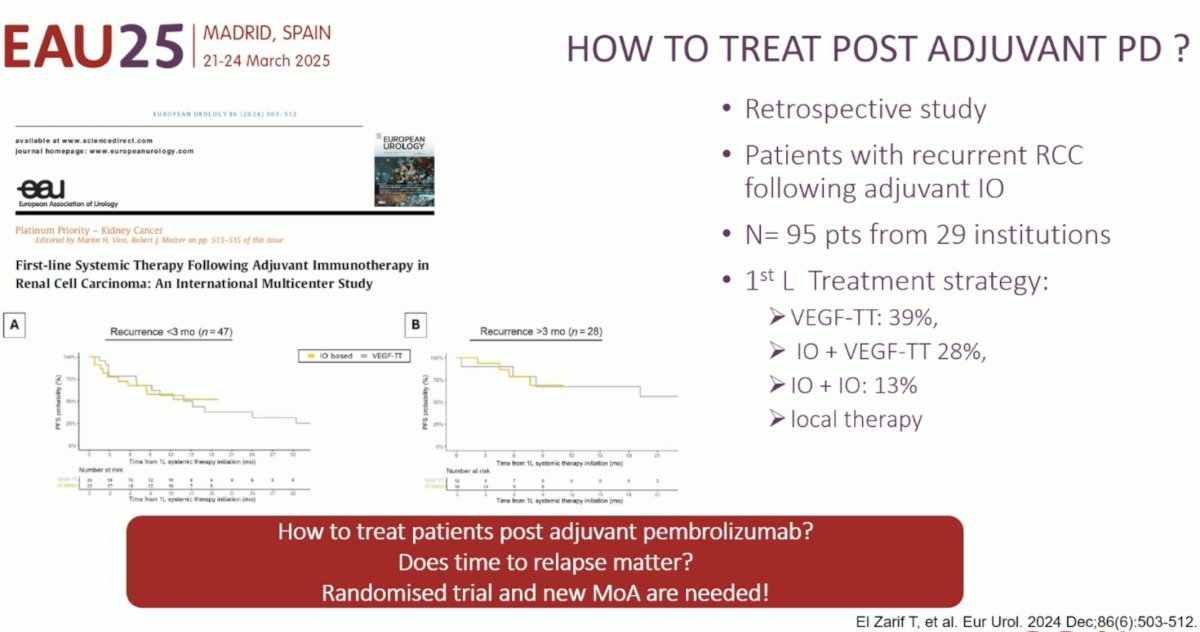
What if this patient had received adjuvant pembrolizumab following his surgery? Would we still recommend IO-IO or IO-TKI regimens? To date, it is unclear how to best treat these patients who have disease progression following exposure to pembrolizumab. How are these patients being treated in the real world? In a retrospective study of 95 patients from 29 institutions, the ‘1st line’ treatment strategies following progression with adjuvant pembrolizumab were:
- Vascular endothelial growth factor inhibitor (VEGFi): 39%
- IO + VEGFi: 28%
- IO-IO: 13%
- Local therapy in select cases
Given the paucity of evidence post-adjuvant pembrolizumab, establishing guidelines recommendations in this setting is challenging. Nonetheless, the EAU guidelines currently note that for patients with early failure within the initial 18 months, single agent TKI should be considered. Conversely, if patients experience late (>18 months) failure, then IO-TKI combinations should be considered.
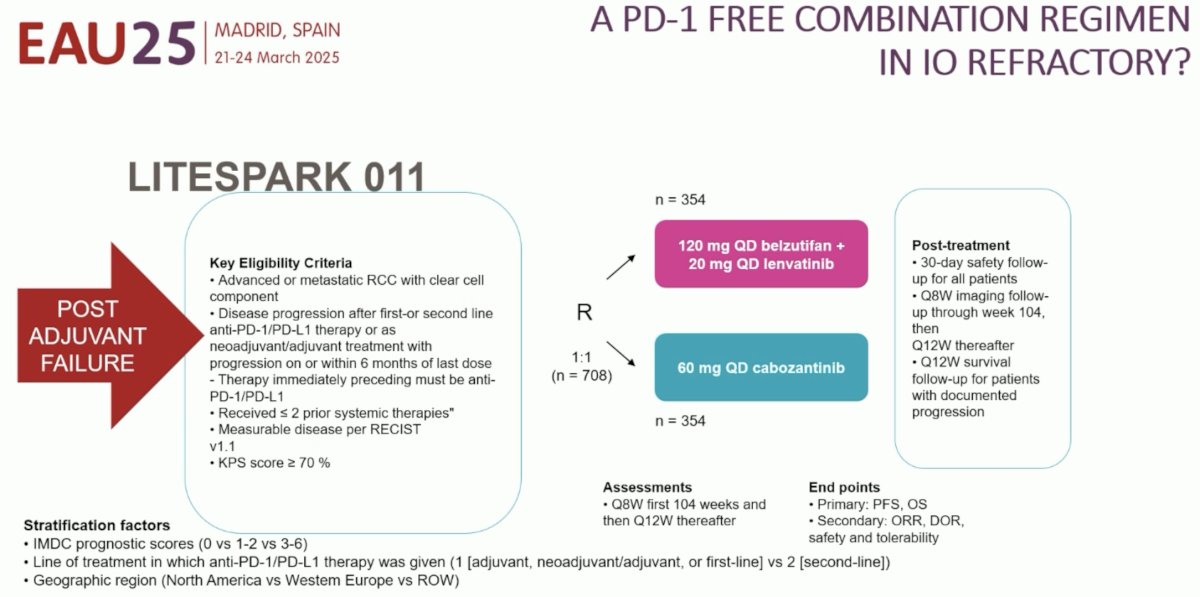
The LITESPARK 011 trial is randomizing patients with advanced/metastatic RCC with disease progression following 1st/2nd line therapy, including post-adjuvant therapy failure, to either belzutifan + lenvatinib or cabozantinib:
Dr. Albiges concluded as follows:
- Combination therapy is standard of care in the 1st line setting
- IO-IO versus IO-TKI is now being investigated in a pragmatic trial (CARE1)
- Little is known in the post-adjuvant failure setting, and we currently are extrapolating strategies from later line settings
- Rescue strategies post-IO therapy are needed given that we are currently unable to achieve a cure beyond the 1st line setting
- Sequence trials are long and challenging
- Real-world data are needed
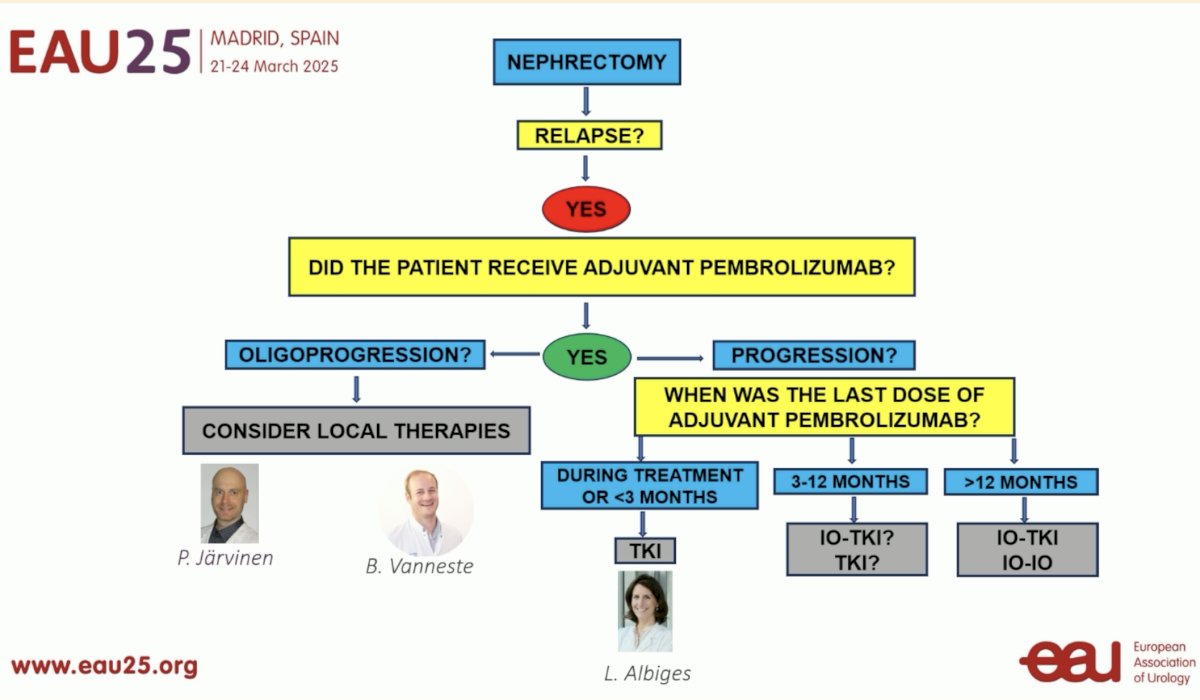
Finally, Dr. Cristina Suárez addressed the role of immunotherapy in this setting. Going back to the case presentation, she noted that if the patient had not received adjuvant pembrolizumab, then the next question would be: did he experience oligoprogression or not? If he had experienced oligoprogression, then local therapy would be reasonable (surgery or SBRT). However, in cases of ‘poly-progression’, then 1st line systemic therapy for locally advanced/metastatic RCC would be indicated.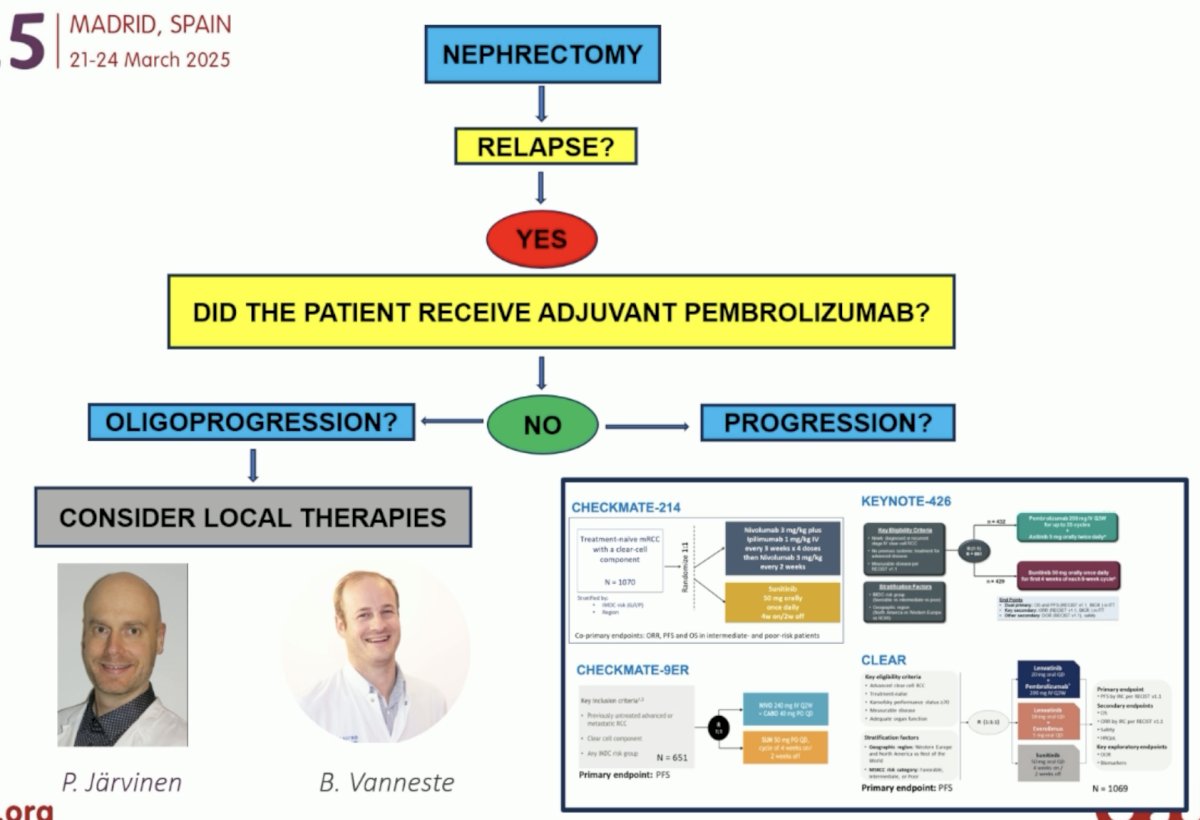
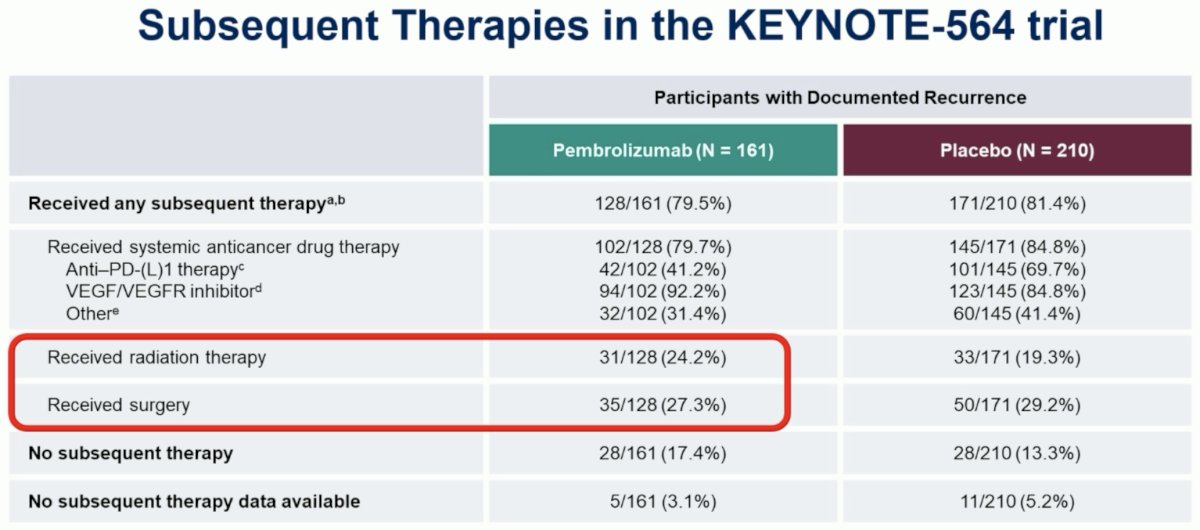
Even if the patient had received adjuvant pembrolizumab and then developed oligoprogression, Dr. Suarez argued that local therapy is still reasonable, as we see below in the subsequent therapy received by patients in the intervention arm of the KEYNOTE-564 trial.12
However, if the patient had received adjuvant pembrolizumab and developed non-oligometastatic disease progression, then what should he receive in this setting? The 1st factor to consider here is: when was the last dose of adjuvant pembrolizumab?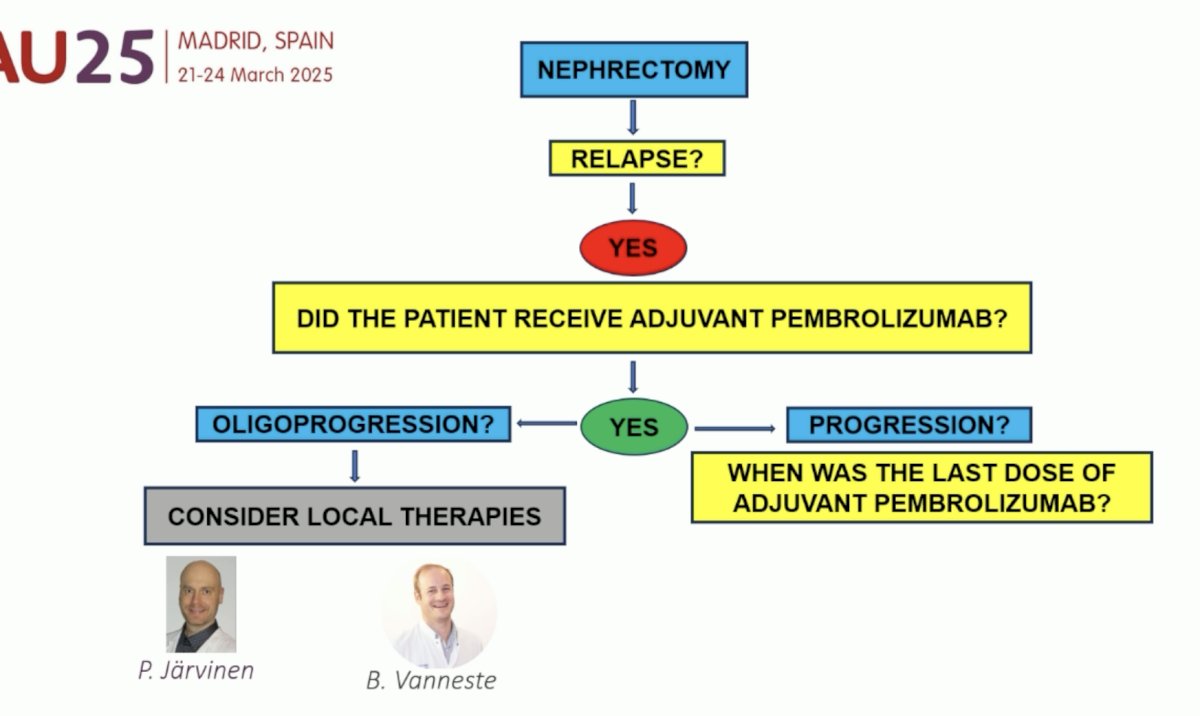
How do we define resistance to PD-1 blockade? The SITC Immunotherapy Resistance Taskforce defines early relapses as those occurring <12 weeks following the last dose of PD-1 inhibitor therapy, and late relapses are those occurring ≥12 weeks following therapy discontinuation.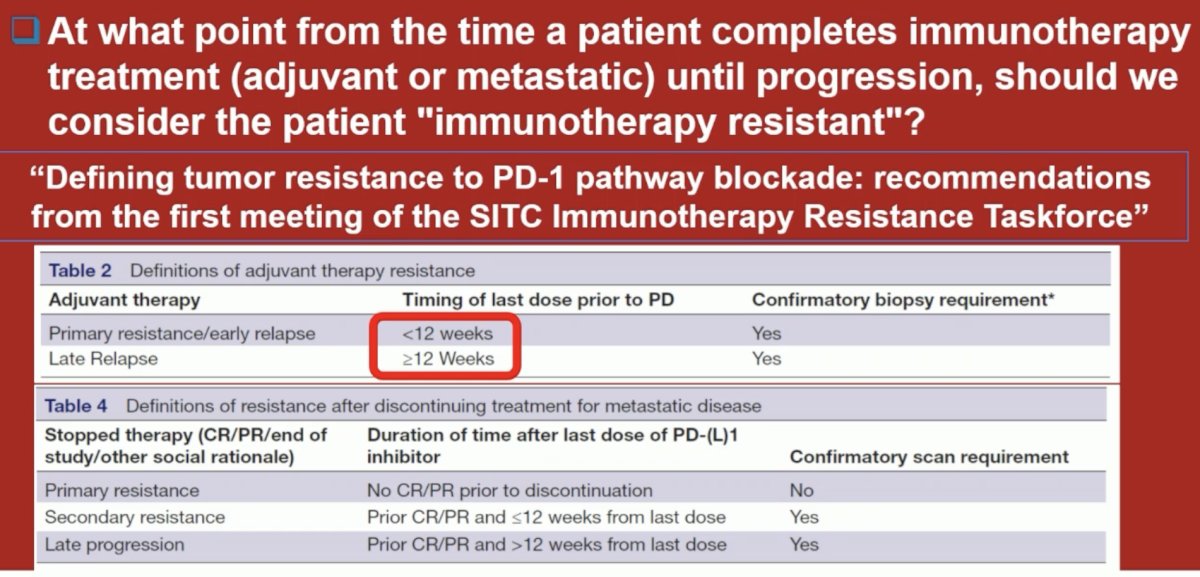
Should we treat patients progressing during adjuvant pembrolizumab or relapsing <3 months after finishing pembrolizumab with IO combinations? Based on the evidence from numerous trials summarized below, there is no role for single agent IO following progression with prior IO therapy: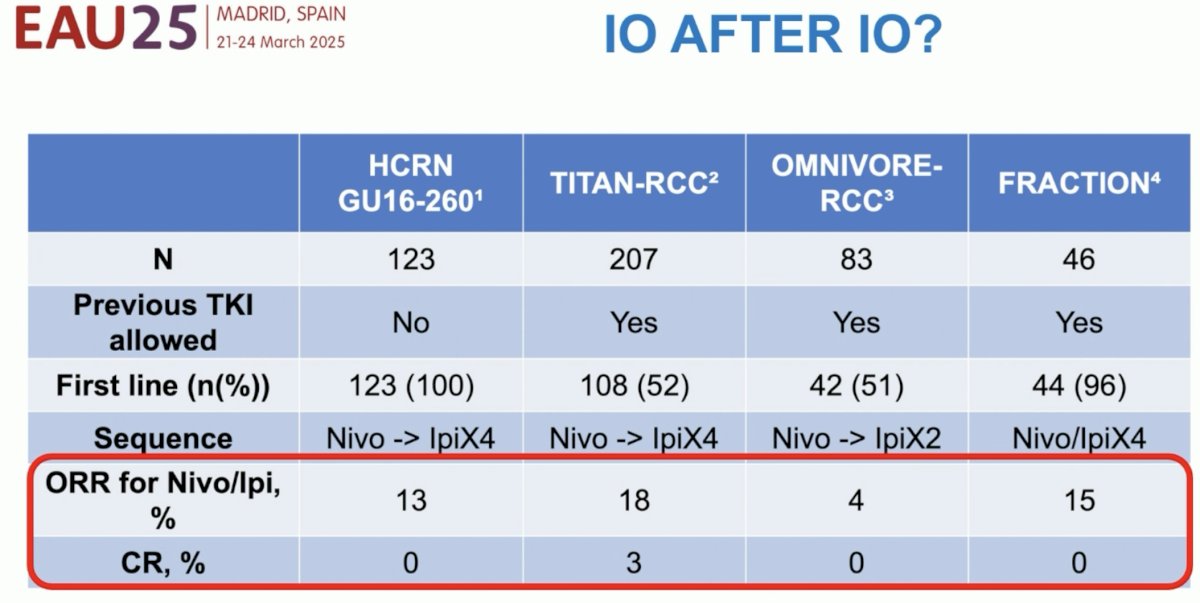
The CONTACT-03 trial randomized patients with radiographic progression during or after prior immune checkpoint inhibitor therapy (adjuvant, 1st or 2nd line) to cabozantinib +/- atezolizumab therapy and failed to demonstrate a PFS or OS benefit with the addition of atezolizumab to cabozantinib.13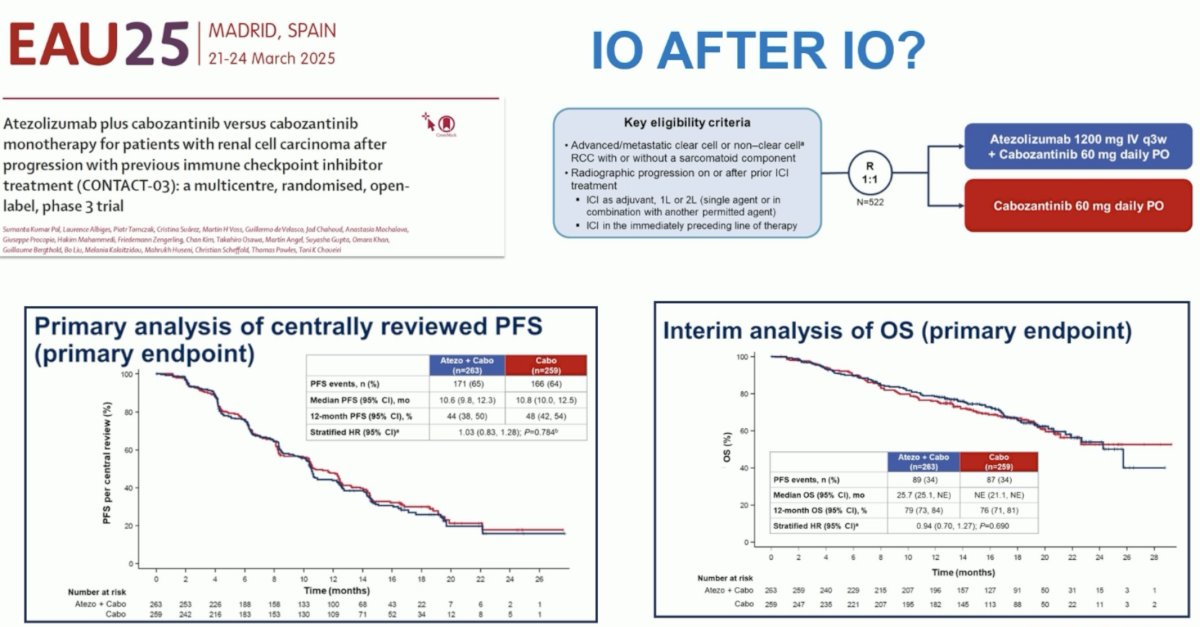
Similarly, the TiNivo-2 phase III trial failed to demonstrate the superiority of tivozanib + nivolumab combination, compared to tivozanib monotherapy, in locally advanced/metastatic clear cell RCC patients who progressed after 1 or 2 prior lines of therapy.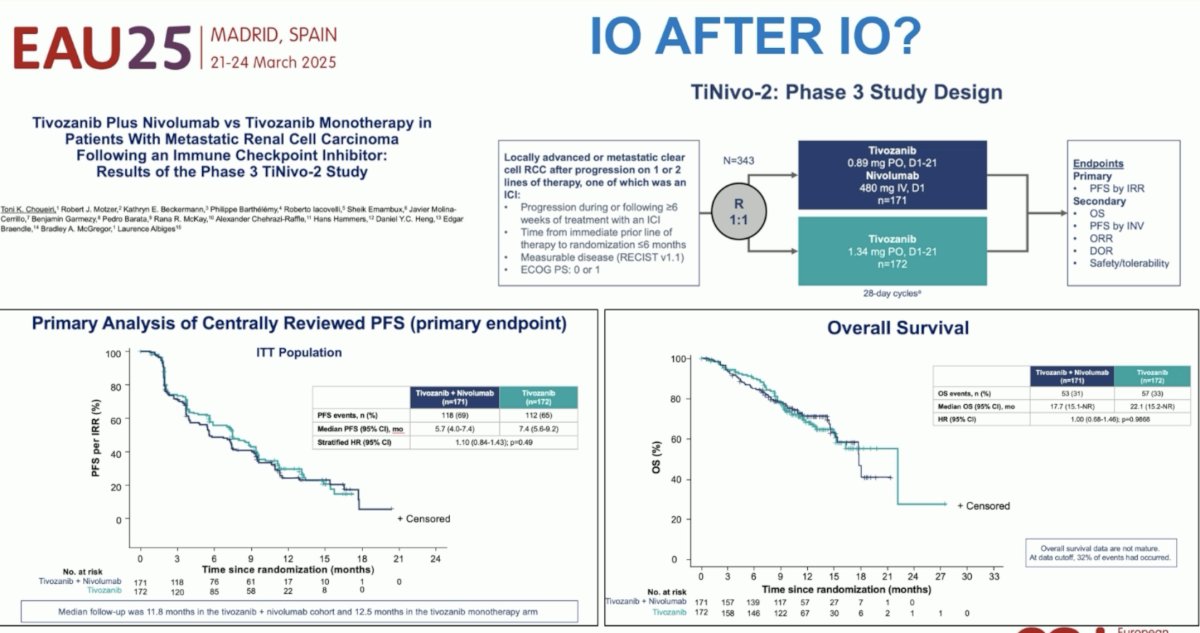
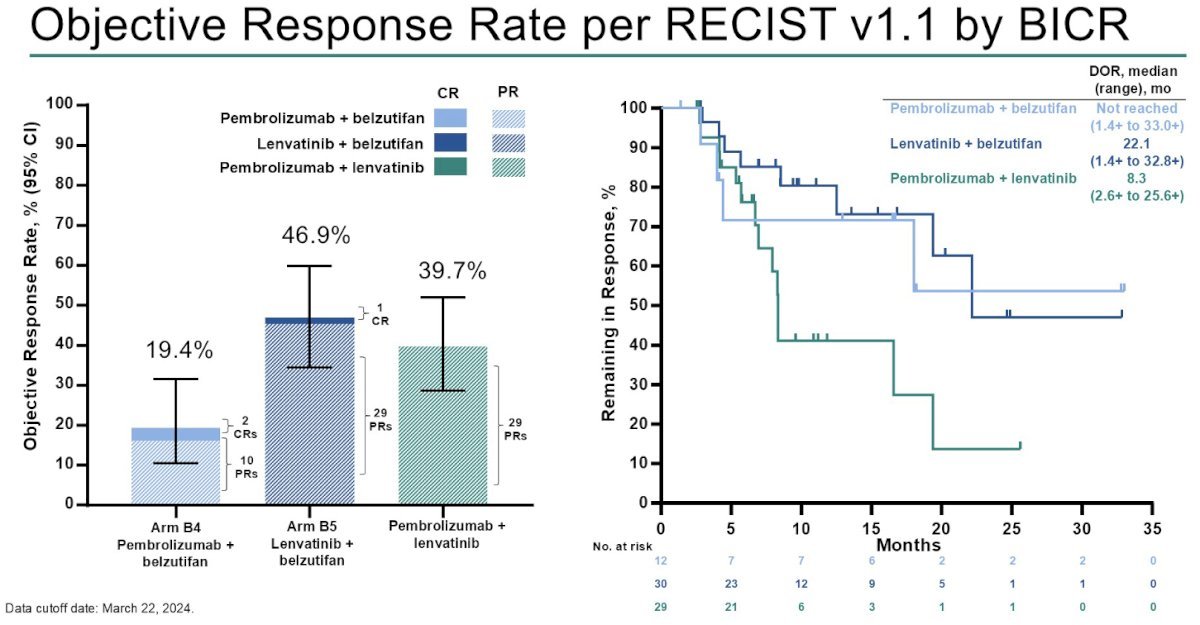
Next, Dr. Suarez highlighted KEYMAKER-U03, a phase 1/2 open-label, rolling arm, umbrella platform designed to evaluate combination treatments for previously treated, clear cell RCC that progressed during or after treatment with PD-(L)1 inhibitor and VEGF-TKI therapy. Presented at ASCO GU 2025 were the results from participants treated with targeted therapy-containing regimens:
- Pembrolizumab + belzutifan
- Lenvatinib + belzutifan
- Pembrolizumab + lenvatinib
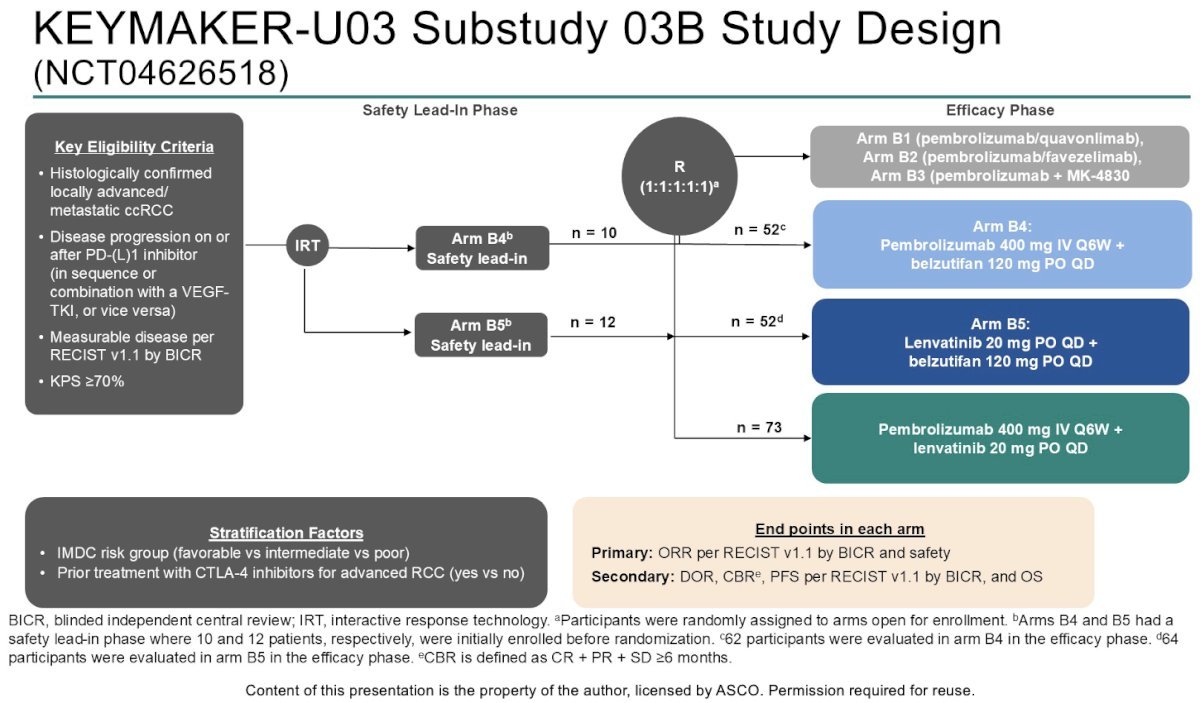
The ORRs were as follows:
- Pembrolizumab + belzutifan (Arm B4): 19.4%
- Median duration of response (DoR): not reached
- Reduction in target lesion size: 66%
- Lenvatinib + belzutifan (Arm B5): 47%
- Median DoR: 22.1 months
- Reduction in target lesion size: 88%
- Pembrolizumab + lenvatinib: 40%
- Median DoR: 8.3 months
- Reduction in target lesion size: 92%
The median PFS rates were highest with the combination of lenvatinib + belzutifan (12.5 months), followed by pembrolizumab + lenvatinib (9.4 months) and pembrolizumab + belzutifan (5.4 months).
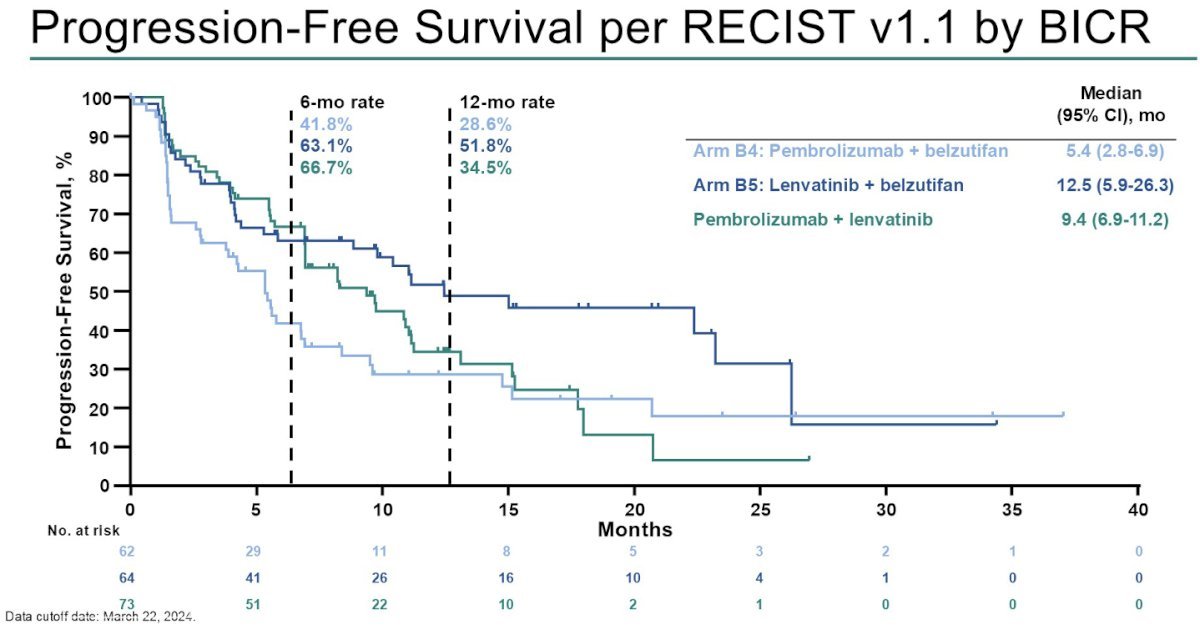
These results provide promise for emerging treatment options in the post-IO setting.
Dr. Suarez concluded her presentation with the following recommendations for the treatment of patients with disease progression following adjuvant pembrolizumab therapy:
Presented by:
- Petrus Järvinen, MD, PhD, Professor, Department of Urology, University of Helsinki and Helsinki University Hospital, Helsinki, Finland.
- Ben Vanneste, MD, PhD, Department of Radiation Oncology, Maastricht University Medical Centre, Maastricht, The Netherlands
- Laurence Albiges MD, PhD, Professor, Medical Oncology, Vice Chair of the Department of Cancer Medicine at the Gustave Roussy Institute, Villejuif, France
- Cristina Suárez, MD, PhD, Medical Oncology, Vall d´Hebron Institute of Oncology (VHIO), Hospital Universitari Vall d´Hebron, Vall d´Hebron Barcelona Hospital Campus, Barcelona, Spain
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 European Association of Urology (EAU) Annual Congress held in Madrid, Spain between March 21st and 24th, 2025
References:- Kriegmair MC, Bertolo R, Karakiewicz PI, et al. Systematic Review of the Management of Local Kidney Cancer Relapse. Eur Urol. 2018; 1(6): 512-23.
- Herout R, Graff J, Brokowetz A, et al. Surgical resection of locally recurrent renal cell carcinoma after nephrectomy: Oncological outcome and predictors of survival. Urol Oncol. 2018; 36(1): 11.e1-6.
- Tornberg SV, Visapaa H, Kilpelainen TP, et al. Surgery for metastases of renal cell carcinoma: outcome of treatments and preliminary assessment of Leuven-Udine prognostic groups in the targeted therapy era. Scan J Urol. 2018; 52(5-6): 419-26.
- Marconi L, Kuusk T, Capitanio U, et al. Local Treatment of Recurrent Renal Cell Carcinoma May Have a Significant Survival Effect Across All Risk-of-recurrence Groups. Eur Urol Open Sci. 2022; 47: 65-72.
- Siva S, Bressel M, Sidhom M, et al. Stereotactic ablative body radiotherapy for primary kidney cancer (TROG 15.03 FASTRACK II): a non-randomised phase 2 trial. Lancet Oncol. 2024; 25(3): 308-16.
- Liu Y, Zhang X, Ma H, et al. Locoregional recurrence after nephrectomy for localized renal cell carcinoma: Feasibility and outcomes of different treatment modalities. Cancer Med. 2022; 11(23): 4430-9.
- Motzer RJ, Tannir NM, McDermott DF, et al. Nivolumab plus Ipilimumab versus Sunitinib in Advanced Renal-Cell Carcinoma. N Engl J Med. 2018; 378(14): 1277-90.
- Rini BI, Plimack ER, Stus V, et al. Pembrolizumab plus Axitinib versus Sunitinib for Advanced Renal-Cell Carcinoma. N Engl J Med. 2019; 380(12): 1116-27.
- Choueiri TK, Powles T, Burotto M, et al. Nivolumab plus cabozantinib versus sunitinib for advanced renal-cell carcinoma. N Engl J Med. 2021; 384(9): 829-41.
- Motzer R, Alekseev B, Rha SY, et al. Lenvatinib plus Pembrolizumab or Everolimus for Advanced Renal Cell Carcinoma. N Engl J Med. 2021; 384(14): 1289-300.
- El-Zarif T, Semaan K, Xie W, et al. First-line Systemic Therapy Following Adjuvant Immunotherapy in Renal Cell Carcinoma: An International Multicenter Study. Eur Urol. 2024; 86(6): 503-12.
- Choueiri TK, Tomczak P, Park SH, et al. Adjuvant Pembrolizumab after Nephrectomy in Renal-Cell Carcinoma. N Engl J Med. 2021; 385(8): 683-94.
- Pal SK, Albiges L, Tomczak P, et al. Atezolizumab plus cabozantinib versus cabozantinib monotherapy for patients with renal cell carcinoma after progression with previous immune checkpoint inhibitor treatment (CONTACT-03): a multicentre, randomised, open-label, phase 3 trial. Lancet. 2023; 302(10397): 185-95.