(UroToday.com) The 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain was host to the Biomarkers to guide peri-operative management in Uro-oncology Plenary Session. Dr. Laurence Albiges discussed the role of PDL1 expression, VHL mutations, KIM-1 in Kidney cancer.
Dr. Albiges began by emphasizing the need to improve patient selection for adjuvant therapies in RCC. In the KEYNOTE-564 trial, a subset of patients derived significant benefit from adjuvant pembrolizumab, while others may have been overtreated.1 Identifying which patients truly benefit remains crucial to optimizing treatment strategies, biomarkers such as PDL1 expression, VHL mutations, KIM-1 may contribute significantly in this area.
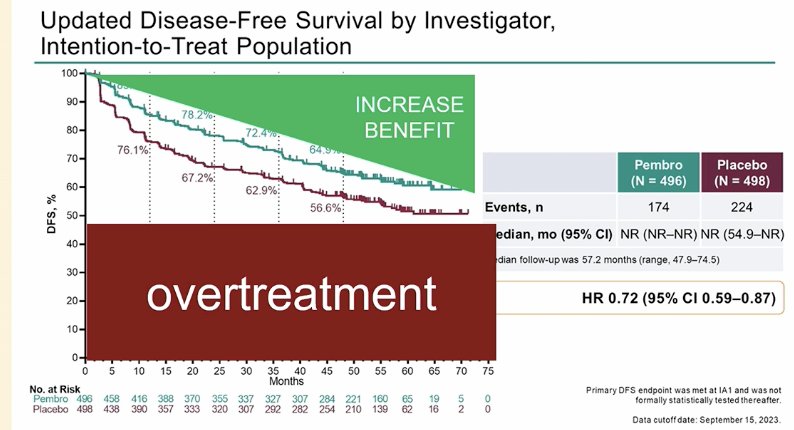
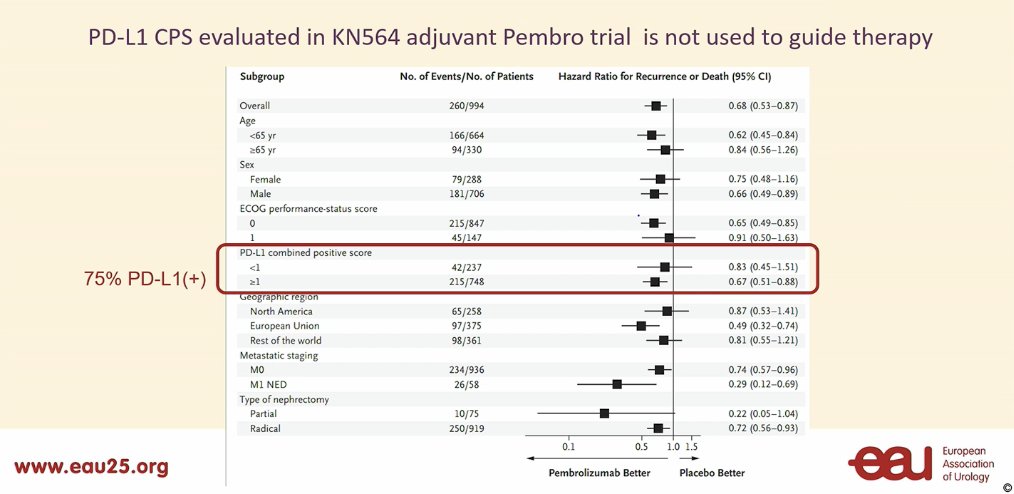
In the KEYNOTE-564 study, PD-L1 CPS was evaluated but not used to guide therapy. Notably, 75% of patients in the study had PD-L1–positive status, which may partly explain why this was the only adjuvant trial to show a positive outcome.1
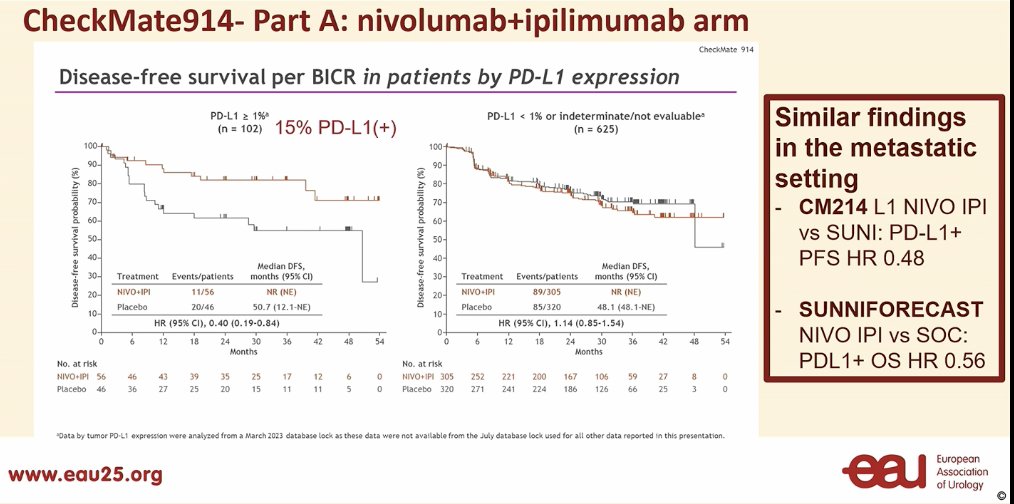
However there is more data regarding PD-L1 expression in RCC. Dr. Albiges presented findings from the CheckMate 914 trial, a negative study, and the SUNNIFORECAST study. Notably, 15% of patients had PD-L1–positive status, and those with PD-L1 positivity experienced significantly improved disease-free survival.2
The ImMOTION 0-10 evaluating adjuvant atezolizumab, was another negative trial. The investigators also evaluated disease-free survival by PD-L1 expression status in an exploratory analysis. Again, patients with high PD-L1 expression showed significantly improved DFS compared to the PD-L1–negative group. Dr. Albiges noted that while this biomarker shows potential, it has not yet been incorporated into routine practice.3

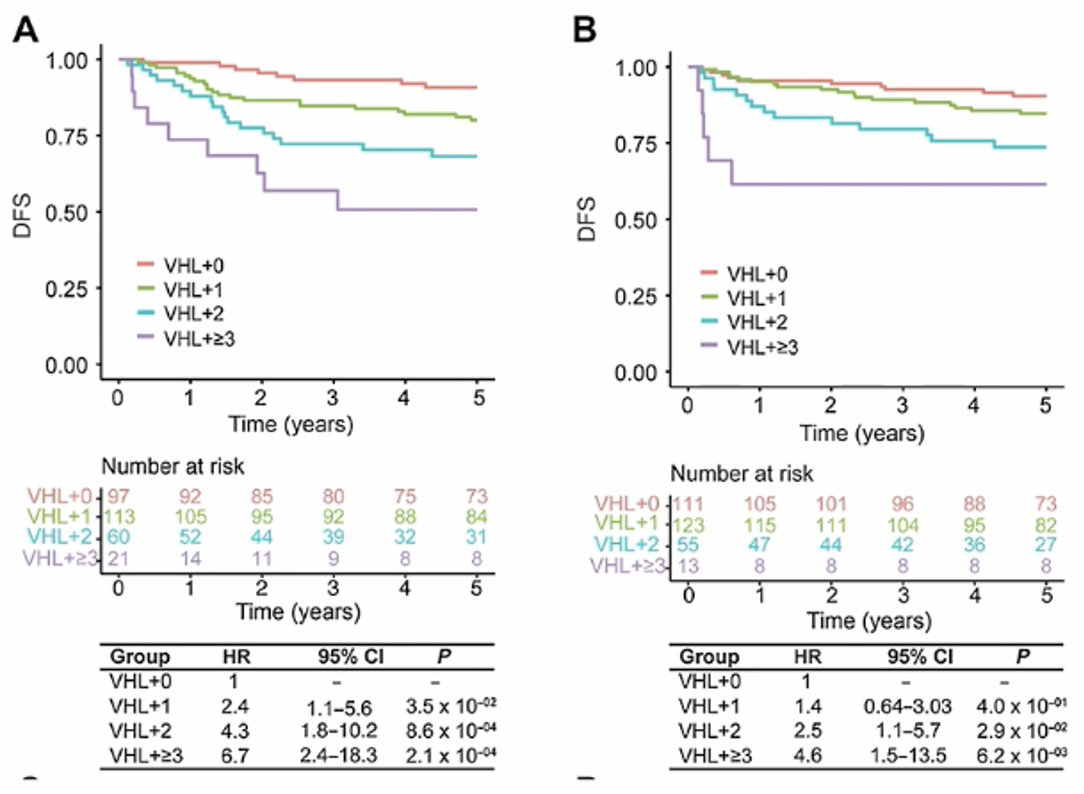
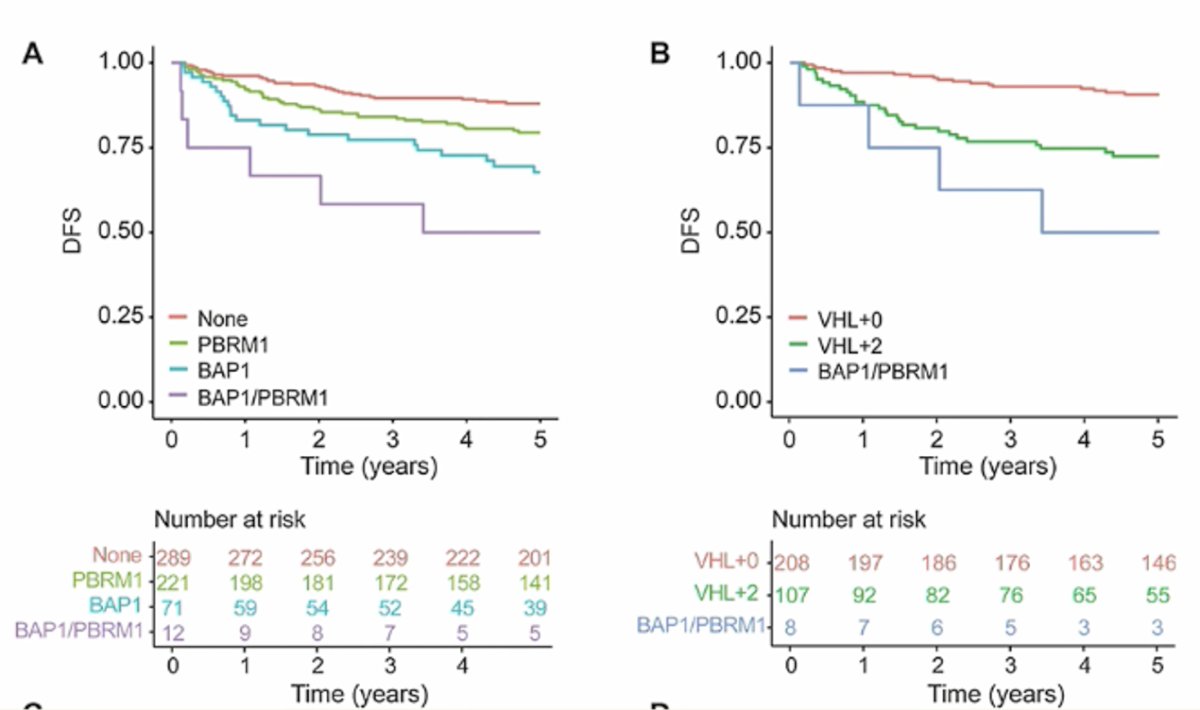
Dr. Albiges presented a study conducted in the UK, where investigators performed genomic sequencing to optimize adjuvant therapy selection. They analyzed somatic mutations across 943 patients, aiming to validate this set and identify those at higher risk of relapse. The somatic mutation status of 12 genes was determined in 943 ccRCC cases with localized RCC to refine risk prediction.4
Tumors containing a VHL mutation alone were associated with significantly improved outcomes compared to tumors with VHL plus additional mutations. In the discovery cohort, the 5-year DFS rates were as follows:
- VHL+0: 90.8%
- VHL+1: 80.1%
- VHL+2: 68.2%
- VHL+≥3: 50.7%
These findings suggest that the presence of additional mutations alongside VHL may indicate a higher risk of relapse and worse disease-free survival.
A key finding of this study is that outcomes vary depending on the specific gene mutation. Patients with BAP1 mutation showed significantly worse DFS compared to those with VHL+0 to VHL+2 mutations. This suggests that BAP1 alterations may serve as a marker for higher relapse risk and poorer prognosis, further highlighting that all mutations are not equivalent in terms of risk of relapse.
However, these biomarkers are so far prognostic but not predictive
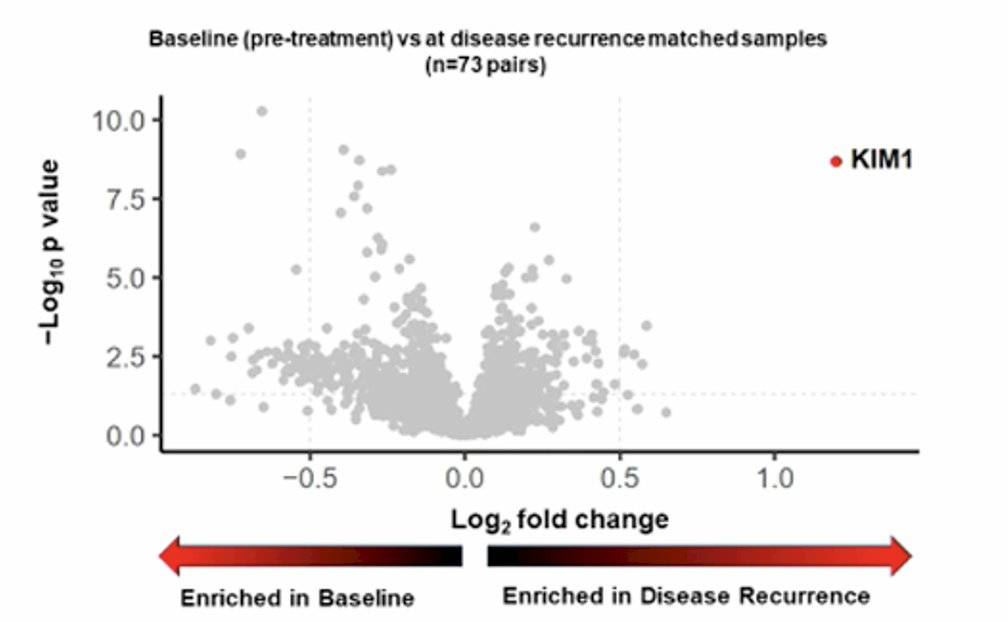
KIM1The circulating kidney injury molecule-1 (KIM-1) biomarker was analyzed in IMmotion010, a randomized Phase 3 study of adjuvant atezolizumab vs. placebo in patients with RCC at increased risk of recurrence after resection. KIM-1 was identified as the most significantly enriched circulating protein in recurrence versus baseline serum samples, suggesting its potential role as a biomarker for disease monitoring and risk stratification in RCC.3
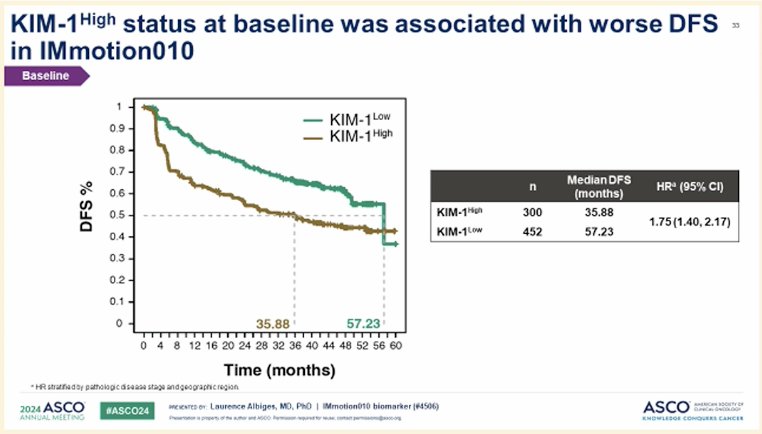
Moreover, KIM-1 high status at baseline was associated with worse DFS in the same population of the IMmotion010 study.3
In the subgroup analysis of the IMmotion010 study assessing different biomarkers, KIM-1 was the only biomarker significantly associated with improved overall survival in patients treated with atezolizumab, as shown in the forest plot below. This finding suggests a potential predictive role for KIM-1 in identifying patients who may derive benefit from adjuvant immune checkpoint inhibition in RCC.

Dr. Albiges highlighted that we are lagging behind in RCC, as most current efforts focus on the adjuvant setting rather than the neoadjuvant setting. She emphasized the need to incorporate biomarkers to better select patients for neoadjuvant trials in RCC, potentially improving treatment strategies and patient outcomes.
Dr. Albiges concluded her presentation with the following messages:
- Biomarkers such as PD-L1 expression, VHL mutations, and KIM-1 have the potential to guide perioperative management in RCC.
- No biomarker is yet implemented in routine practice to guide adjuvant therapy decisions.
- Key open questions for localized RCC and biomarker use include:
- Improving selection of patients at higher risk of relapse.
- Evaluating neoadjuvant approaches versus adjuvant therapy.
- Developing adaptive trial designs based on neoadjuvant response and residual disease.
Presented by: Laurence Albiges, MD, PhD, Medical oncologist and the Head of the Genitourinary Unit at Gustave Roussy Institute, Villejuif
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the European Association of Urology (EAU) 2025 Annual Meeting, Madrid, Spain, Fri, Mar 21 – Mon, Mar 24, 2025.
References:- Choueiri TK, Tomczak P, Park SH, Venugopal B, Ferguson T, Symeonides SN, Hajek J, Chang YH, Lee JL, Sarwar N, Haas NB, Gurney H, Sawrycki P, Mahave M, Gross-Goupil M, Zhang T, Burke JM, Doshi G, Melichar B, Kopyltsov E, Alva A, Oudard S, Topart D, Hammers H, Kitamura H, McDermott DF, Silva A, Winquist E, Cornell J, Elfiky A, Burgents JE, Perini RF, Powles T; KEYNOTE-564 Investigators. Overall Survival with Adjuvant Pembrolizumab in Renal-Cell Carcinoma. N Engl J Med. 2024 Apr 18;390(15):1359-1371. doi: 10.1056/NEJMoa2312695. PMID: 38631003.
- Motzer RJ, Russo P, Grünwald V, Tomita Y, Zurawski B, Parikh O, Buti S, Barthélémy P, Goh JC, Ye D, Lingua A, Lattouf JB, Albigès L, George S, Shuch B, Sosman J, Staehler M, Vázquez Estévez S, Simsek B, Spiridigliozzi J, Chudnovsky A, Bex A. Adjuvant nivolumab plus ipilimumab versus placebo for localised renal cell carcinoma after nephrectomy (CheckMate 914): a double-blind, randomised, phase 3 trial. Lancet. 2023 Mar 11;401(10379):821-832. doi: 10.1016/S0140-6736(22)02574-0. Epub 2023 Feb 9. PMID: 36774933; PMCID: PMC10259621.
- Pal SK, Uzzo R, Karam JA, Master VA, Donskov F, Suarez C, Albiges L, Rini B, Tomita Y, Kann AG, Procopio G, Massari F, Zibelman M, Antonyan I, Huseni M, Basu D, Ci B, Leung W, Khan O, Dubey S, Bex A. Adjuvant atezolizumab versus placebo for patients with renal cell carcinoma at increased risk of recurrence following resection (IMmotion010): a multicentre, randomised, double-blind, phase 3 trial. Lancet. 2022 Oct 1;400(10358):1103-1116. doi: 10.1016/S0140-6736(22)01658-0. Epub 2022 Sep 10. PMID: 36099926.
- Vasudev NS, Scelo G, Glennon KI, Wilson M, Letourneau L, Eveleigh R, Nourbehesht N, Arseneault M, Paccard A, Egevad L, Viksna J, Celms E, Jackson SM, Abedi-Ardekani B, Warren AY, Selby PJ, Trainor S, Kimuli M, Cartledge J, Soomro N, Adeyoju A, Patel PM, Wozniak MB, Holcatova I, Brisuda A, Janout V, Chanudet E, Zaridze D, Moukeria A, Shangina O, Foretova L, Navratilova M, Mates D, Jinga V, Bogdanovic L, Kovacevic B, Cambon-Thomsen A, Bourque G, Brazma A, Tost J, Brennan P, Lathrop M, Riazalhosseini Y, Banks RE. Application of Genomic Sequencing to Refine Patient Stratification for Adjuvant Therapy in Renal Cell Carcinoma. Clin Cancer Res. 2023 Apr 3;29(7):1220-1231. doi: 10.1158/1078-0432.CCR-22-1936. PMID: 36815791; PMCID: PMC10068441.