(UroToday.com) The 2025 EAU annual meeting featured a session on intravesical therapy for bladder cancer and a presentation by Dr. Marco Moschini discussing that the combination of gemcitabine and docetaxel is the ideal combination therapy. Dr. Moschini notes that the mechanism of action for gemcitabine is a nucleoside analog and inhibition of DNA function, whereas docetaxel inhibits tubulin disassembly leading to inhibition of cell division. Thus, these two intravesical chemotherapy agents have a synergistic effect.
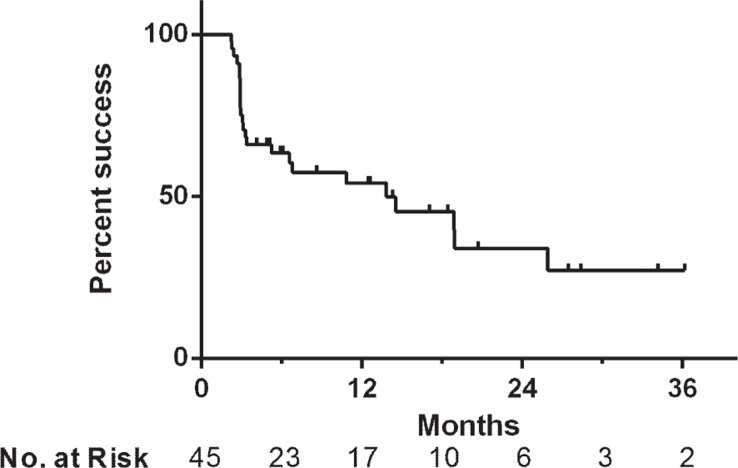
For the remainder of his presentation, Dr. Moschini discussed several of the retrospective studies that have shaped utilization of gemcitabine + docetaxel in non muscle invasive bladder cancer. This chemotherapy combination was first described ~10 years ago based on the University of Iowa experience. Among 45 patients treated between June 2009 and May 2014, 9% were BCG naïve, 42% were BCG refractory, 40% were BCG relapsing, and 9% were BCG intolerant.1 The median follow-up was 15 months, with treatment success reported 66% at first surveillance, 54% at 1 year, and 34% at 2 years after initiating induction:
The Iowa experience was expanded to a multicenter analysis of 276 patients, including 38% of patients being BCG unresponsive.2 Over a median follow-up of 23 months, the 2 year outcomes:
- Recurrence free survival: 46%
- High grade recurrence free survival: 52%
- Cancer specific mortality: 4%
- Overall mortality: 13%
During the induction phase of treatment, this is done over 6 weeks of weekly intravesical instillations, while the maintenance phase includes monthly instillations for 10 to 24 months. With regards to administration, docetaxel (37.5 mg/50 mL) is instilled and retained in the bladder for 60 minutes. Subsequently, the bladder is drained after retention using a clamped catheter. Gemcitabine (1 g/50 mL) is administered after bladder drainage and patients are instructed to retain the drug for 90 minutes prior to voiding.
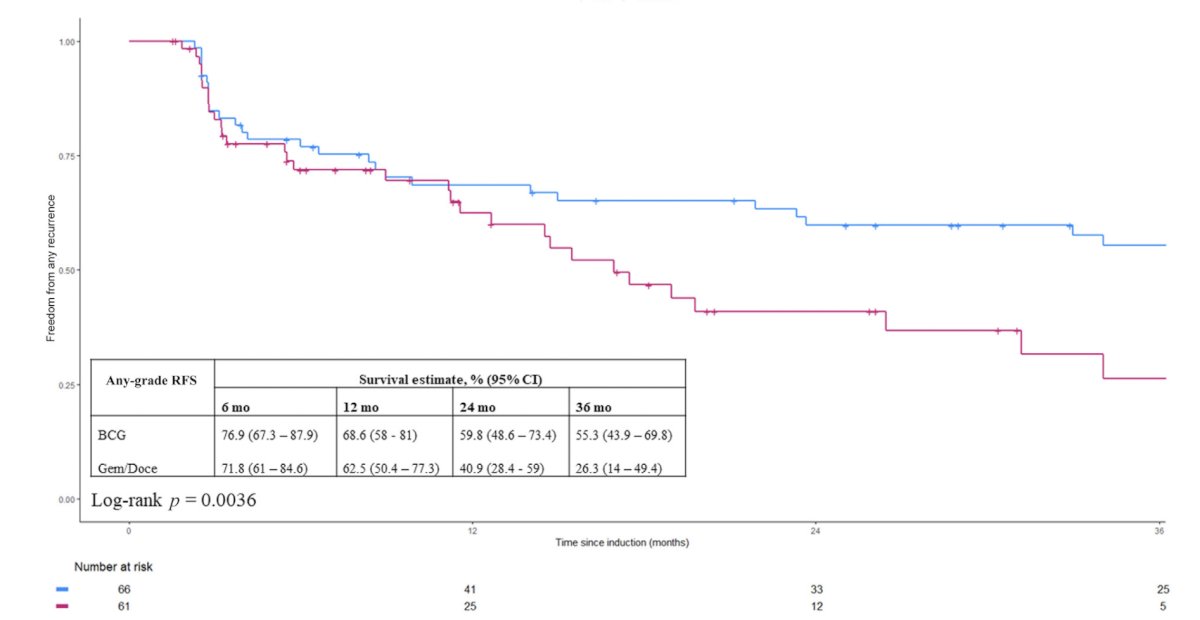
For intermediate risk patients using gemcitabine + docetaxel, Dr. Moschini discussed the experience of Mount Sinai who treated 127 patients with intermediate risk non muscle invasive bladder cancer patients with induction + one year of maintenance.3 Over a median follow-up of 53 months, the 1 year high grade recurrence free survival with BCG was 93% versus 82% for gemcitabine + docetaxel, and the 2 year high grade recurrence free survival with BCG was 81% versus 61% for gemcitabine + docetaxel. The any grade recurrence free survival is as follows:
In a multicenter assessment of gemcitabine + docetaxel in intermediate risk disease, Tan et al. evaluated oncological outcomes for 182 patients treated with BCG (n = 100) or intravesical sequential gemcitabine and docetaxel (n = 82).4 Notably, recurrence rates were similar in the two treatment groups (HR 1.06, 95% CI 0.65-1.73; p = 0.8). Dr. Moschini provided the following summary statements for treatment of intermediate risk patients with gemcitabine + docetaxel:
- There are excellent results observed with 2 year maintenance therapy in terms of high grade recurrence and progression
- Patients receiving maintenance therapy show significantly improved results compared to induction-only therapy
- Patients who have undergone previous intravesical therapies have worse outcomes compared to those receiving gemcitabine + docetaxel as first line treatment
Next, Dr. Moschini discussed the use of gemcitabine + docetaxel in high risk, BCG naïve patients. The Hopkins experience included a prospective phase 2 trial of 25 BCG naïve patients with a median follow-up of 20 months.5 There was a 100% complete response rate at 3 months, with a 12 month recurrence free survival of 92%, with no progression and no patients requiring radical cystectomy. The Iowa experience with high risk disease included treatment of 107 BCG-naïve patients.6 The 1 year recurrence free survival rate was 85%, the 2 year recurrence free survival rate was 82%, the 1 year high grade recurrence free survival rate was 87%, and the 2 year high grade recurrence free survival rate was 84%. One patient underwent a radical cystectomy secondary to end stage lower urinary tract symptoms.
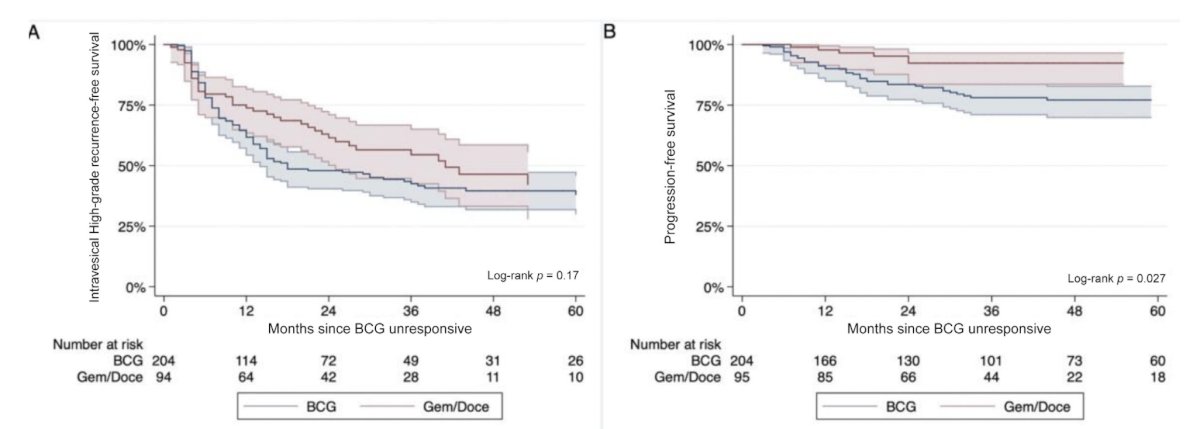
For BCG treated high risk disease, Dr. Moschini discussed a multicenter experience of 299 patients with a median follow-up of 40 months.7 Of these patients, 95 were treated with gemcitabine + docetaxel, reporting a 1 year high grade recurrence free survival rate of 74%, and a 1 year progression free survival rate of 96%. Of note, further BCG was associated with a higher progression risk (HR 2.6):
Earlier in 2025, Scilipoti and colleagues reported the experience of gemcitabine + docetaxel for the EuroGemDoce group, of which there were 75 patients previously exposed to BCG and followed for a median of 9 months.8 In this experience, the 1 year outcomes were as follows:
- Disease free survival: 73%
- High grade recurrence free survival: 79%
- Progression free survival: 96%
- Bladder intact event free survival: 95%
Dr. Moschini concluded his presentation discussing that the combination of gemcitabine and docetaxel is the ideal combination therapy with the following take home points:
- BCG-naïve high risk non muscle invasive bladder cancer shows excellent outcomes with gemcitabine + docetaxel, but most studies report a short median follow-up (~20 months)
- Patients with BCG-unresponsive disease demonstrate promising efficacy, with recent cohorts outperforming earlier reports
- There is a lack of prospective randomized comparative studies that limit definitive treatment strategies
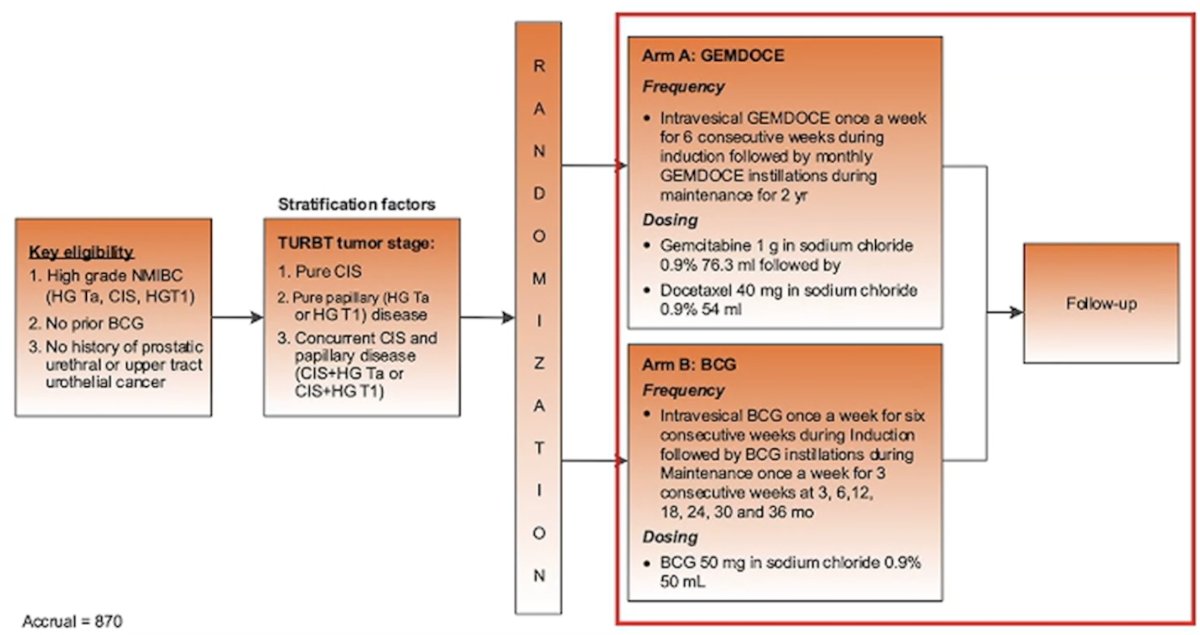
With regards to future perspectives, the BRIDGE trial has a primary objective of evaluating whether gemcitabine + docetaxel is non-inferior to BCG for event free survival in BCG naïve patients:
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain between March 21st and 24th 2025
References:
- Steinberg RL, Thomas LJ, O’Donnell MA, et al. Sequential intravesical gemcitabine and docetaxel for the salvage treatment of non-muscle invasive bladder cancer. Bladder Cancer. 2015 Apr 30;1(1):65-72.
- Steinberg RL, Thomas LJ, Brooks N, et al. Multi-Institution Evaluation of Sequential Gemcitabine and Docetaxel as Rescue Therapy for Nonmuscle Invasive Bladder Cancer. J Urol. 2020 May;203(5):902-909.
- Kolanukuduru KP, Ben-David R, Lidagoster S, et al. Comparative effectiveness of Bacillus Calmette-Guerin and Sequential Intravesical Gemcitabine and Docetaxel for Treatment-naïve Intermediate-risk non-muscle-invasive bladder cancer. Eur Urol Focus. 2024 Sep 20:S2405-4569(24)00173-1.
- Tan WS, McElree IM, Davaro F, et al. Sequential intravesical gemcitabine and docetaxel is an alternative to Bacillus Calmette-Guerin for the treatment of intermediate-risk non-muscle invasive bladder cancer. Eur Urol Oncol. 2023 Oct;6(5):531-534.
- Patel SH, Gabrielson AT, Chan S, et al. A phase 2 trial of intravesical gemcitabine and docetaxel in the treatment of Bacillus Calmette-Guerin-naïve nonmuscle-invasive urothelial carcinoma of the bladder. J Urol. 2024 Jul;212(1):95103.
- McElree IM, Steinberg RL, Martin AC, et al. Sequential intravesical gemcitabine and docetaxel for bacillus Calmette-Guerin-naïve high-risk nonmuscle-invasive bladder cancer. J Urol. 2022 Sep;208(3):589-599.
- Taylor J, Kamat AM, Annapureddy D, et al. Oncologic outcomes of sequential intravesical gemcitabine and docetaxel compared with Bacillus Calmette-Guerin in patients with Bacillus Calmette-Guerin-unresponsive non-muscle invasive bladder cancer. Eur Urol Oncol. 2025 Apr;8(2):469-476.
- Scilipoti P, Longoni M, de Angelis M, et al. Gemcitabine and docetaxel for high-risk non-muscle-invasive bladder cancer: EuroGemDoce group results. BJU Int. 2025 Jan 11 [Epub ahead of print].