(UroToday.com) The 2025 EAU annual meeting featured a session on intravesical therapy for bladder cancer and a state of the art lecture by Dr. Peter Black discussing definitions, outcomes, and treatment of BCG unresponsive non muscle invasive bladder cancer. Dr. Black started his presentation by defining the non muscle invasive bladder cancer disease states, in particular, the subgroups of high risk disease:
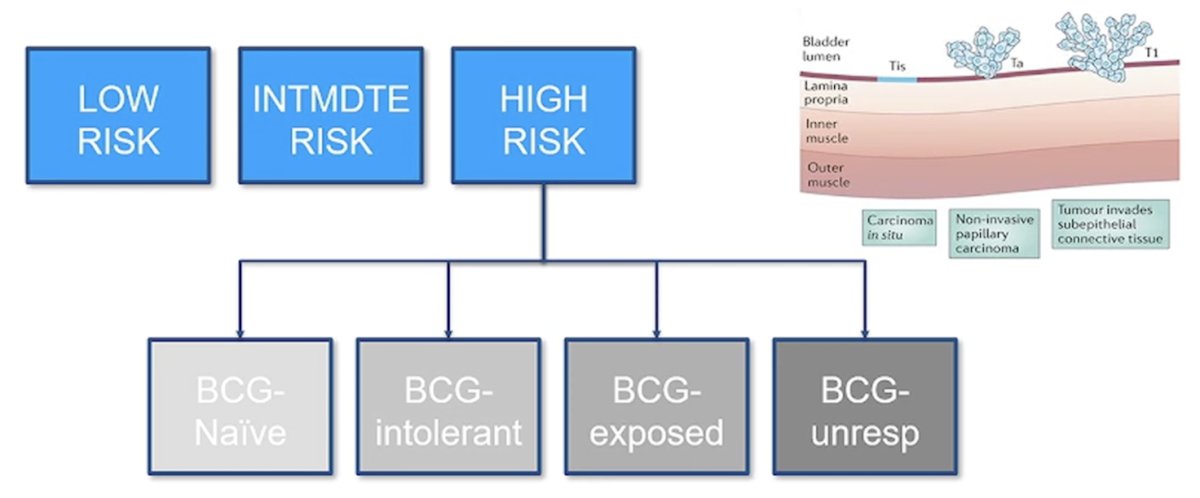
Importantly, treatments and trials are determined by disease state.
In 2018, the FDA provided guidance for the industry regarding developing drugs and biologics for the treatment of BCG-unresponsive non muscle invasive bladder cancer. This resulted in several important definitions for BCG unresponsive disease:
- Persistent Ta/CIS after induction and one round of maintenance BCG (BCG refractory disease), or
- Persistent T1 after induction BCG (BCG refractory), or
- After response to BCG, relapse of high grade Ta/T1 within 6 months or CIS within 12 months of the last dose of BCG (early relapse)
Dr. Black notes that the standard treatment of BCG unresponsive non muscle invasive bladder cancer is radical cystectomy, however (i) many patients are ineligible for a radical cystectomy, (ii) many patients prefer bladder preserving therapy, and (iii) many urologists offer bladder preserving therapy. Second line treatment options for BCG-unresponsive non muscle invasive bladder cancer include the following:
- Single agent chemotherapy
- Gemcitabine + docetaxel
- Pembrolizumab
- Nadofaragene firadenovec
- N803
- Trimodality therapy
- Novel therapy in clinical trials
In the wake of the BCG shortage over the last several years, intravesical gemcitabine + docetaxel has emerged as a combination therapy for patients with NMIBC. In 2020, Steinberg et al.1 investigated intravesical gemcitabine/docetaxel as rescue therapy for NMIBC. Among 276 patients over a median follow-up of 22.9 months, 39% of patients were CIS alone, 26% were Ta high grade, 21% were T1 high grade, and 13% were Ta low grade. Overall, 53% had one BCG induction course, 46% had 2+ BCG induction courses, and 38% were “BCG unresponsive.” Of note, some responders went on to maintenance therapy (monthly versus the SWOG schedule) for 24 months. One and 2-year recurrence-free survival rates were 60% and 46%, and high grade recurrence-free survival rates were 65% and 52%, respectively:
Ten patients (3.6%) had disease progression on transurethral resection, and 43 patients (15.6%) went on to cystectomy (median 11.3 months from induction), of whom 11 (4.0%) had progression to muscle invasion.
With regards to immune checkpoint inhibitors, KEYNOTE-0572 showed that among 96 patients with CIS +/- Ta/T1, pembrolizumab lead to a complete response rate of 41% at 3 months, 19% at 12 months, and a grade 3+ adverse event rate of 13%, which led to FDA approval. The SWOG S1605 trial3 showed that among 74 patients with CIS +/- Ta/T1, atezolizumab led to a compete response rate of 42% at 3 months, 24% at 12 months, and a grade 3+ adverse event rate of 13%. The sample size was too small for FDA approval. Finally, presented at ESMO 2024, SunRISe-1 showed that among 28 patients with CIS +/- Ta/T1, cetrelimab had a 46% complete response rate at any time, 23% at 12 months, and a Grade 3+ adverse event rate of 7%. Notably, TAR-200 alone was superior and safer than cetrelimab.
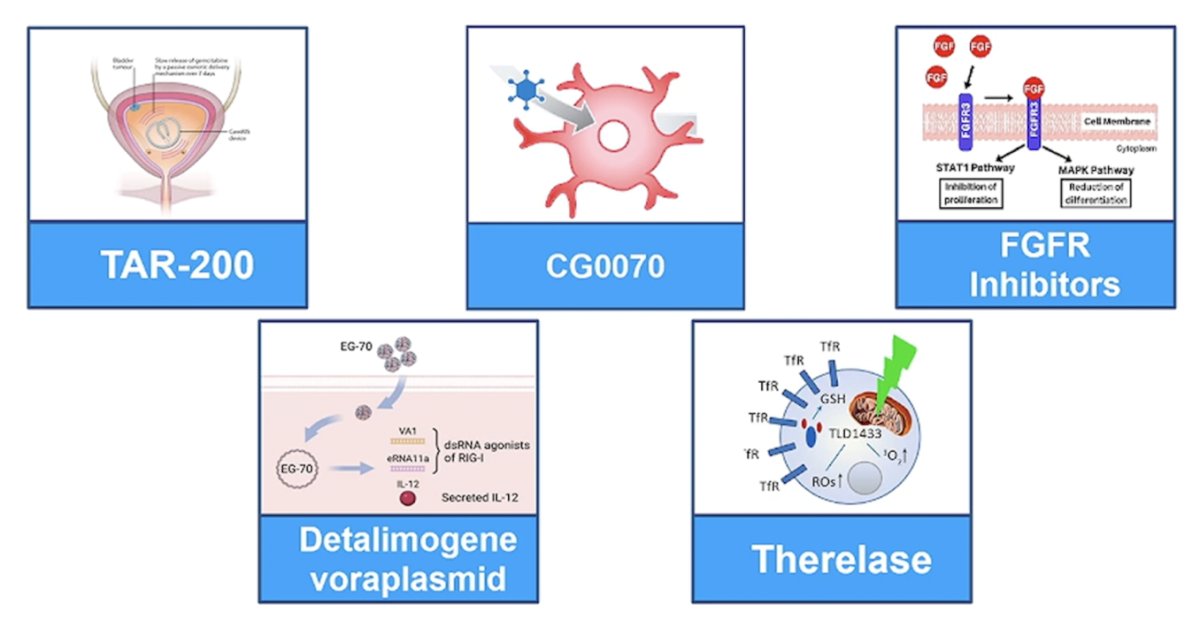
In December 2022, the FDA approved nadofaragene firadenovec based on phase 3 results that showed a complete response rate at 3 months of 53%, and 24% at 12 months.4 In April 2024, the FDA approved N-803 in combination with BCG based on phase 3 results that showed a complete response at 3 or 6 months of 62%, and 58% of complete responses durable 12+ months.5 Novel therapies for BCG unresponsive non muscle invasive bladder cancer include: (i) TAR-200, (ii) CG0070, (iii) FGFR inhibitors, (iv) detalimogene voraplasmid, and (v) therelase:
The latest trial results from new agents are as follows:
- SunRISe-1 (ESMO 2024): TAR-200 (n = 85) led to an 83.5% complete response rate at 3 or 6 months, with a Kaplan Meier estimated 57% complete response rate at 12 months
- BOND-3 (SUO 2024): Cretostimogene grenadenorepvec (n = 110; re-induction allowed) led to a 74.5% complete response rate at 3 or 6 months, with a Kaplan Meier estimated 50% complete response rate at 12 months
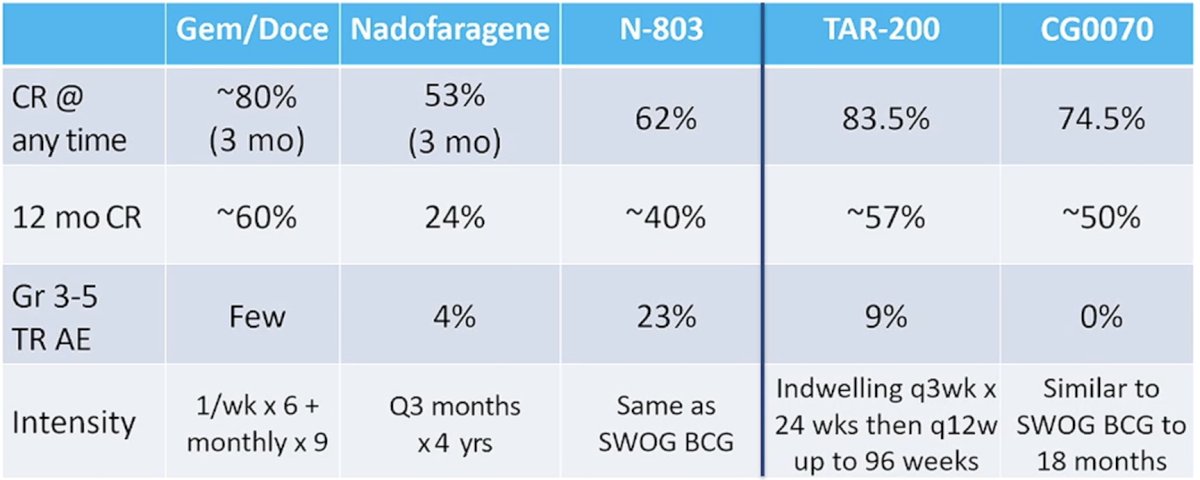
The following table summarizes the current trials and data for intravesical therapy for BCG unresponsive non muscle invasive bladder cancer:
Dr. Black concluded his state of the art lecture by discussing definitions, outcomes, and treatment of BCG unresponsive non muscle invasive bladder cancer by highlighting what’s next:
- Sequential therapy
- Combination therapy
- Randomized multi-arm trials
- Implementation across disease states
- What are the downstream repercussions of change in first line therapy?
- We cannot forget the utility of radical cystectomy
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain between March 21st and 24th 2025
References:
- Steinberg RL, Thomas LJ, Brooks N, et al. Multi-Institution Evaluation of Sequential Gemcitabine and Docetaxel as Rescue Therapy for Nonmuscle Invasive Bladder Cancer. J Urol. 2020 May;203(5):902-909.
- Balar AV, Kamat AM, Kulkarni GS, et al. Pembrolizumab monotherapy for the treatment of high-risk non-muscle-invasive bladder cancer unresponsive to BCG (KEYNOTE-057): An open-label, single-arm, multicenter, phase 2 study. Lancet Oncol. 2021 Jul;22(7):919-930.
- Black PC, Tangen CM, Singh P, et al. Phase 2 trial of Atezolizumab in Bacillus Calmette-Guerin-unresponsive high risk non-muscle-invasive bladder cancer: SWOG S1605. Eur Urol. 2023 Dec;84(6):536-544.
- Boorjian SA, Alemozaffar M, Konety BR, et al. Intravesical nadofaragene firadenovec gene therapy for BCG-unresponsive non-muscle-invasive bladder cancer: A single-arm, open-label, repeat-dose clinical trial. Lancet Oncol. 2021 Jan;22(1):107-117.
- Chamie K, Chang SS, Kramolowsky E, et al. IL-15 Superagonist NAI in BCG-Unresponsive Non-Muscle-Invasive Bladder Cancer. NEJM Evid 2022; 2(1)