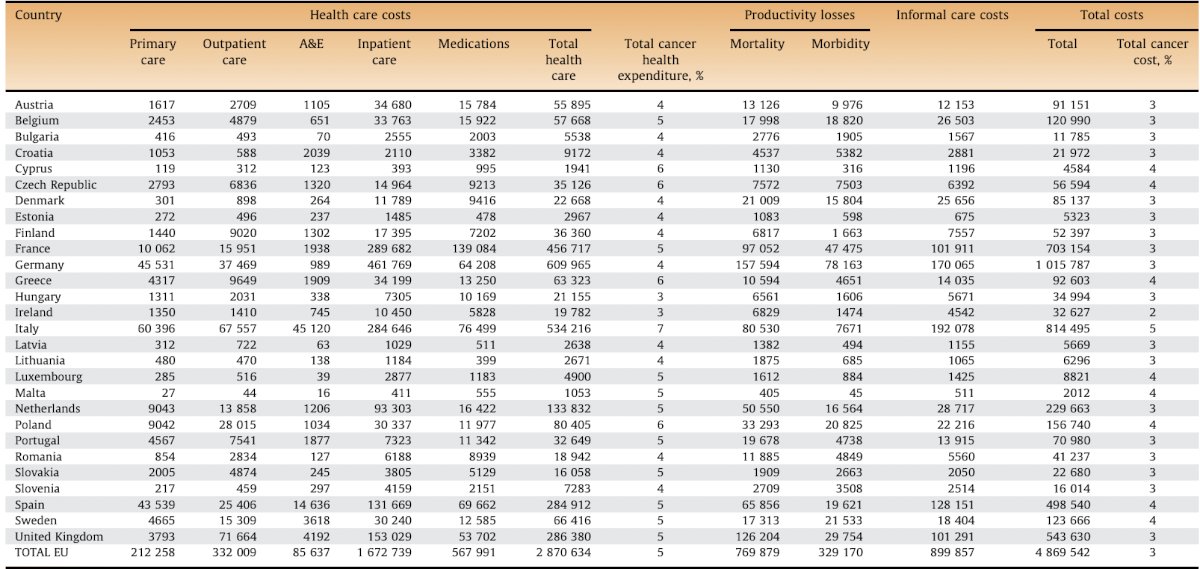
(UroToday.com) The 2025 EAU annual meeting featured a session on intravesical therapy for bladder cancer and a state of the art lecture by Dr. Evanguelos Xylinas discussing the use of urine diagnostics to de-escalate follow-up in the growing population of non muscle invasive bladder cancer patients. Dr. Xylinas started by emphasizing that there is a clinical unmet need, given the economical and patient burden of bladder cancer surveillance. Indeed, the cost of bladder cancer in the European Union is prohibitive, as highlighted in the following table:1
Part of the economic problem is that standard follow-up regimens include frequent cystoscopic examinations for both low risk and high risk disease, according to the AUA and EAU guidelines. In a Markov model from Mossanen et al.2 assessing cost by risk categories, the cumulative costs of care over a 5-year period were $52,125 for low-risk, $146,250 for intermediate-risk, and $366,143 for high-risk non muscle invasive bladder cancer. The primary driver of cost was progression to muscle-invasive disease requiring definitive therapy, contributing to 81% and 92% of overall cost for intermediate- and high-risk disease, respectively. In an assessment of cystoscopic surveillance practices among low risk non muscle invasive bladder cancer, Han et al.3 found that overuse occurred in 75% (852/1,135) of patients and an excess of 1,846 more cystoscopies performed than recommended.
Cystoscopy is an invasive endoscopic procedure and is easy to perform, but it can cause substantial discomfort and anxiety for patients. In fact, previous studies have suggested that 96% of patients would accept a urine test in place of cystoscopy if the sensitivity of the test was > 90-95%. Urine cytology is a non-invasive method, whereby exfoliated cells are inspected for morphological characteristics of malignancy in urine sediment. However, the diagnostic interpretation relies on the experience of the pathologist, which makes standardization difficult. Generally, the specificity of cytology is greater than other established biomarkers, but sensitivity is limited, especially in low grade tumors. Other old urinary commercially available biomarkers include:
- NMP22:
- Nuclear matrix proteins (NMP) are known to provide structural support to the cell nucleus
- NMP22 is elevated in malignant urothelial cells, excreted via the urine after cell death
- In a pooled analysis in surveillance of non muscle invasive bladder cancer, the overall sensitivity and specificity were 69% and 81%, respectively
- BTA
- Basement membrane complexes released by tumor cells after stromal invasion, in which the basement membrane is damaged
- There are a small number of studies, but the sensitivity and specificity for surveillance of non muscle invasive bladder cancer ranges from 40-72% and 29-96%, respectively
- UroVysion
- Molecular FISH to detect specific chromosomal abnormalities in urine sediments
- DNA probes are used to target centromeres of chromosomes 3, 7, 17, and the 9p21 locus
- The overall sensitivity and specificity ranges for surveillance of non muscle invasive bladder cancer are 73-81% and 96%-100%
- ImmunoCyt
- A microscopic immunofluorescence assay for detection of specific antigens on tumor cells in the urine
- There are a small number of studies, but the overall sensitivity and specificity for surveillance of non muscle invasive bladder cancer ranges from 50-85% and 62-86%, respectively
ADXBLADDER is an ELISA test that utilizes detection of minichromosome maintenance protein (MCM) 5, which is a member of a larger family of MCM proteins that play a pivotal role in the initiation of DNA replication. MCM5 is highly expressed in cells that are proliferating and in cells with proliferation potential, and expression is low or absent in healthy differentiated cells.4 In 2020, Roupret et al.5 performed a blinded, prospective cohort, multicenter European study of ADXBLADDER among 1,431 eligible patients of which 127 were diagnosed with a bladder cancer recurrence. The sensitivity and NPV were 45% and 93%, respectively, and among non pTa low grade tumors, the sensitivity was 44.9% and sensitivity was 75.6%. In a study comparing ADXBLADDER to urinary cytology, Gontero et al.6 reported that the overall performance of ADXBLADDER demonstrated a sensitivity of 51.9%, a specificity of 66.4%, and a NPV of 92%. The sensitivity of ADXBLADDER for low- and high-grade recurrences was 44.1% and 58.8%, respectively. By contrast, cytology sensitivity was 16.7%, specificity was 98% and NPV was 90.7%. Cytology sensitivity for both low- and high-grade disease was 17.6%.
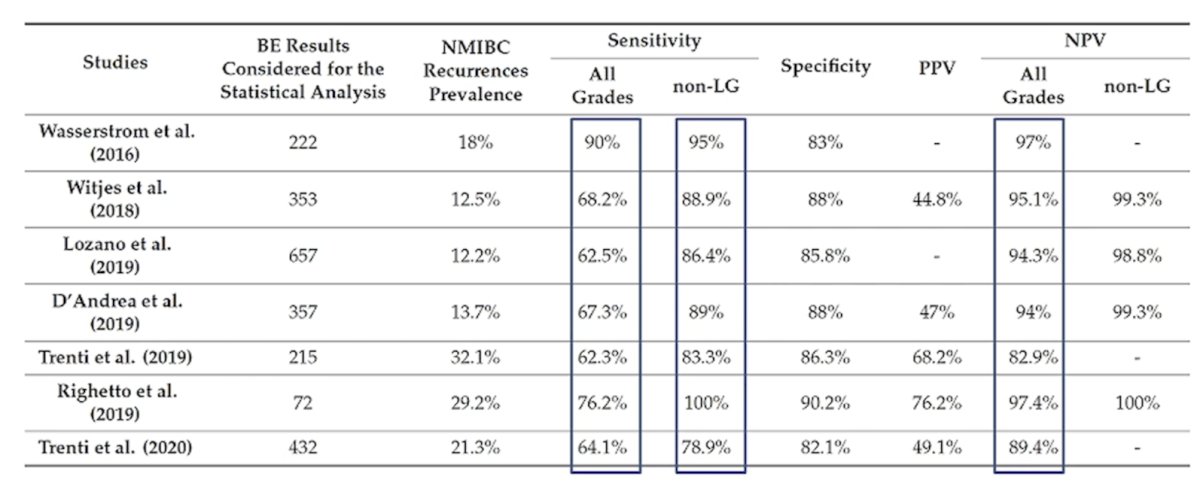
Next. Dr. Xylinas discussed Bladder EpiCheck, which is a real time PCR urinary test that detects changes in DNA methylation associated with bladder cancer in a panel of 15 genes. A numeric value between 0 to 100 (EpiScore) is based on the methylation pattern present, and an EpiScore >= 60 is considered positive. The following table summarizes the performance of Bladder EpiCheck in published studies:
Xpert Bladder Cancer Monitor is a test with 5 mRNA targets: ABL1, CRH, IGF2, UPK1B, and ANXA10. The assay is performed in a self contained cartridge using GeneXpert Systems (Cepheid), with a turnaround time of ~90 minutes. Studies suggest that Xpert has an overall sensitivity of 74% and 83% for high grade tumors, with a negative predictive value of 93% and 98% for high grade tumors.
Finally, Dr. Xylinas discussed VisioCyt, which is a machine learning platform for improving urinary cytology:

In the prospective VISIOCYT1 trial, Lebret et al.7 reported that VisioCyt's sensitivity was 80.9% (95% CI 73.9-86.4%) and specificity was 61.8% (95% CI 53.4-69.5%). In high-grade tumors, the sensitivity was 93.7% (95% CI 86.0-97.3%), and in low-grade tumors 66.7% (95% CI 55.2-76.5%).
Dr. Xylinas concluded his presentation by discussing the use of urine diagnostics to de-escalate follow-up in the growing population of non muscle invasive bladder cancer patients by asking if urinary markers are ready for prime time:
- For primary diagnosis? No
- In the surveillance setting? Yes, there is an unmet clinical need
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain between March 21st and 24th 2025
References:
- Leal J, Luengo-Fernandez R, Sullivan R, et al. Economic burden of bladder cancer across the European Union. Eur Urol. 2016 Mar;69(3):438-447.
- Mossanen M, Wang Y, Szymaniak J, et al. Evaluation the cost of surveillance for non-muscle-invasive bladder cancer: An analysis based on risk categories. World J Urol. 2019 Oct;37(10):2059-2065.
- Han DS, Lynch KE, Chang JW, et al. Overuse of cystoscopic surveillance among patients with low-risk non-muscle-invasive bladder cancer – A National study of patient, provider, and facility factors. Urology. 2019 Sep;131:112-119.
- Wolfs JRE, Hermans TJN, Koldewijn EL, et al. Novel urinary biomarkers ADXBLADDER and bladder EpiCheck for diagnostics of bladder cancer: A review. Urol Oncol. 2021 Mar;39(3):161-170.
- Roupret M, Gontero P, McCracken SR, et al. Diagnostic accuracy of MCM5 for the detection of recurrence in nonmuscle invasive bladder cancer followup: A blinded, prospective cohort, multicenter European study. J Urol. 2020 Oct;204(4):685-690.
- Gontero P, Montanari E, Roupret M, et al. Comparison of the performances of the ADXBLADDER test and urinary cytology in the follow-up of non-muscle-invasive bladder cancer: A blinded prospective multicentric study. BJU Int. 2021 Feb;127(2):198-204.
- Lebret T, Paoletti X, Pignot G, et al. Artificial intelligence to improve cytology performance in urothelial carcinoma diagnosis: Results from validation phase of the French, multicenter, prospective VISIOCYT1 trial. World J Urol. 2023 Sep;41(9):2381-2388.