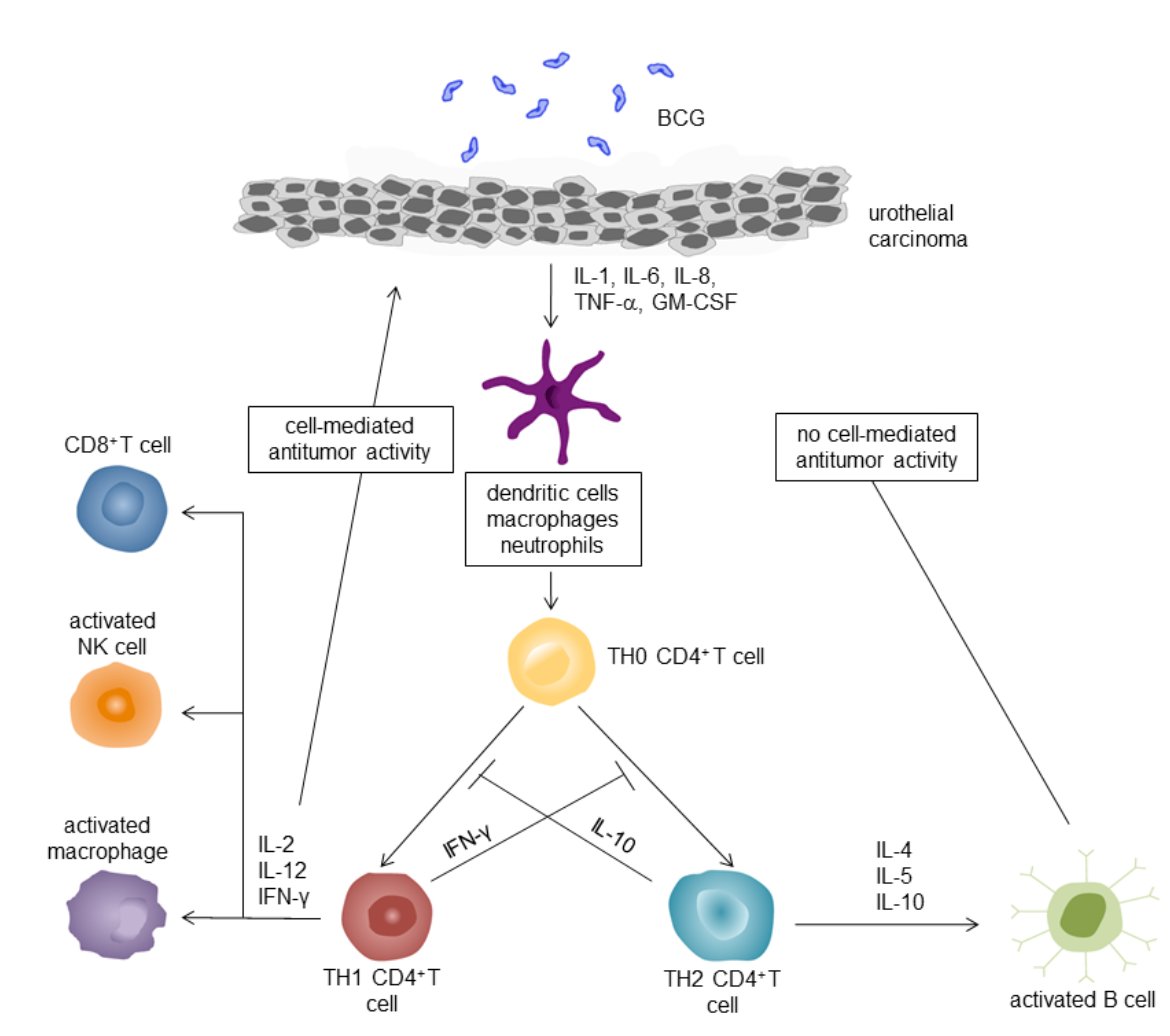
(UroToday.com) The 2025 EAU annual meeting featured a session on intravesical therapy for bladder cancer and a presentation by Dr. Trinity Bivalacqua discussing that BCG harnesses local immunomodulators for maximal impact. Dr. Bivalacqua started his presentation by highlighting the proposed intravesical BCG mechanism of action:
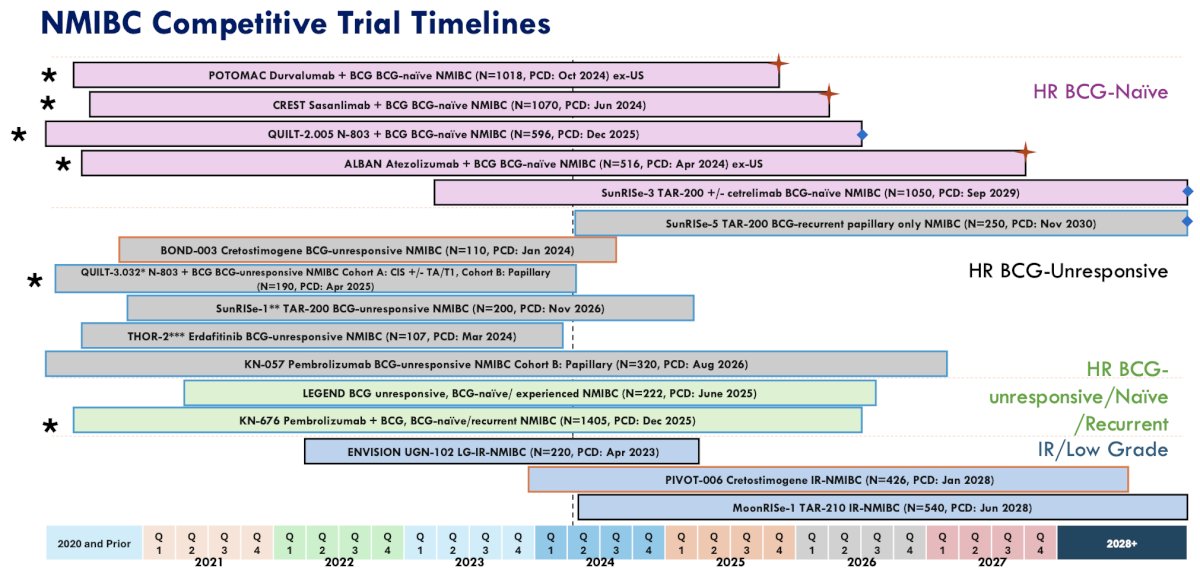
Since 2020, there have been a remarkable number of non muscle invasive bladder cancer clinical trials, in the (i) high risk BCG naïve, (ii) high risk BCG unresponsive, (iii) high risk BCG unresponsive/naïve/recurrent, and (iv) intermediate risk/low grade disease spaces:
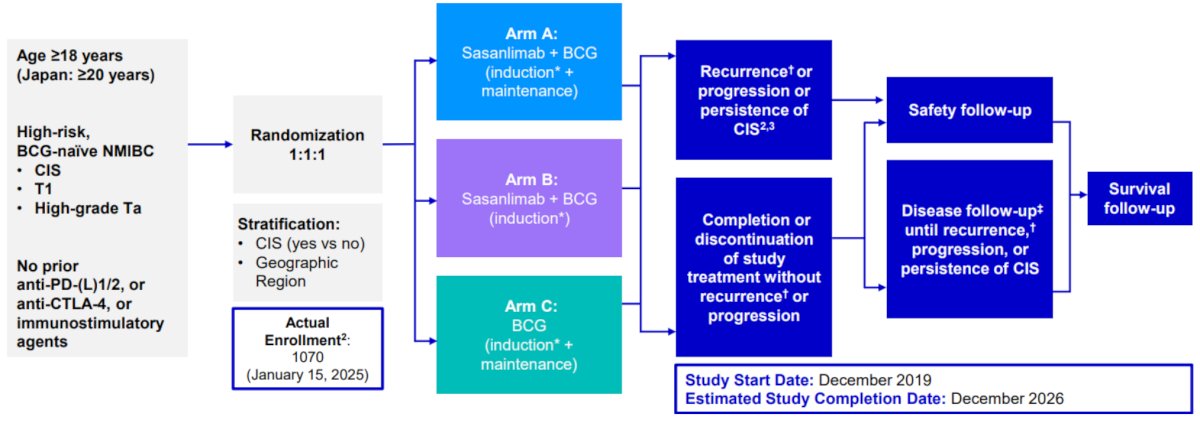
Dr. Bivalacqua then discussed the CREST phase 3 trial of BCG + sasanlimab (an anti-PD-1 antibody) given subcutaneously in BCG-naïve non muscle invasive bladder cancer. There is strong rationale for investigating PD-(L)1 inhibition + BCG in this disease space:
- A high unmet need: despite benefit from BCG induction + maintenance, ~50% of patients experience recurrence in <5 years or become BCG unresponsive
- Strong preclinical rationale: Preclinical data suggest a role for PD-1/PD-L1 axis in bladder cancer, and involvement of BCG in tumor PD-L1 expression
- PD-(L)1 inhibitor monotherapy in BCG unresponsive setting: clinical evidence supports the use of PD-1 or PD-L1 inhibitors as monotherapy in high risk BCG unresponsive non muscle invasive bladder cancer
- Benefits of BCG and PD(L)-1 inhibition combination: in preclinical rat models, combination BCG and PD(L)-1 inhibition activates a potent anti-tumor response and prolongs survival of bladder cancer versus either agent alone
- Demonstrating superiority of sasanlimab + BCG (induction) versus BCG monotherapy (induction + maintenance) in prolonging event free survival
- Demonstrating superiority of sasanlimab + BCG (induction without maintenance) versus BCG monotherapy (induction + maintenance) in prolonging overall survival
- Estimating the complete response rate and duration of complete response of sasanlimab + BCG (induction with or without maintenance) and BCG monotherapy (induction and maintenance) in patients with CIS at randomization
- For patients receiving sasanlimab + BCG or BCG monotherapy, evaluate health reported quality of life, time to cystectomy, disease specific survival, safety, pharmacokinetics, immunogenicity, and recurrence of low grade disease.
As of a January 13, 2025 press release, this phase III trial met its primary endpoint, noting a clinically meaningful and statistically significant improvement for sasanlimab + BCG versus BCG alone.
First published in 2022, Meghani et al.1 reported the first-in-human intravesical delivery of pembrolizumab, identifying immune activation in BCG unresponsive non muscle invasive bladder cancer. Specifically, they showed progressive remodeling of local immune contents over the course of treatment by urine analysis of immune cells and cytokines: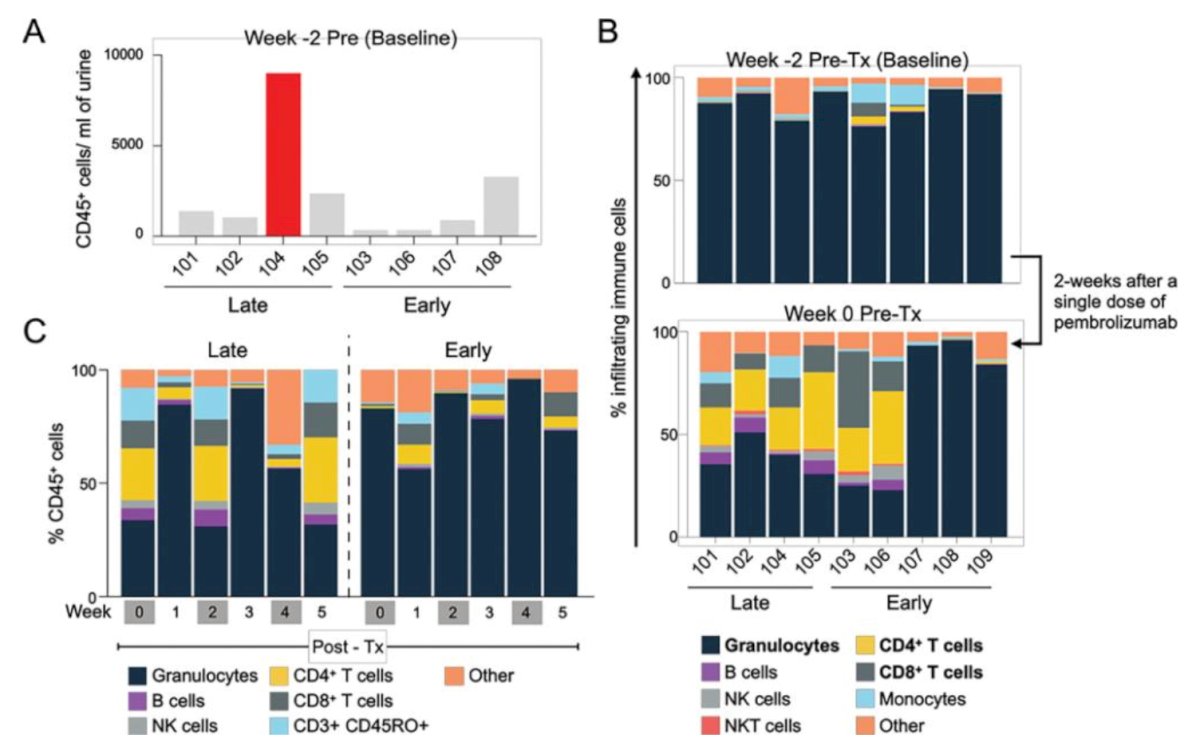
Currently, there are three FDA approved therapies for BCG unresponsive non muscle invasive bladder cancer:
- Pembrolizumab systemic monotherapy2
- Nadofaragene firadenovec intravesical monotherapy3
- N-803 + BCG combination intravesical agents4
N-803 is a IL-15 super agonist that forms a mutant IL-15 based immunostimulatory fusion protein complex from IL-15 agonism. It promotes proliferation and activation of natural killer cells and CD8+ T cells, thereby increasing the efficacy of BCG and cancer cell death: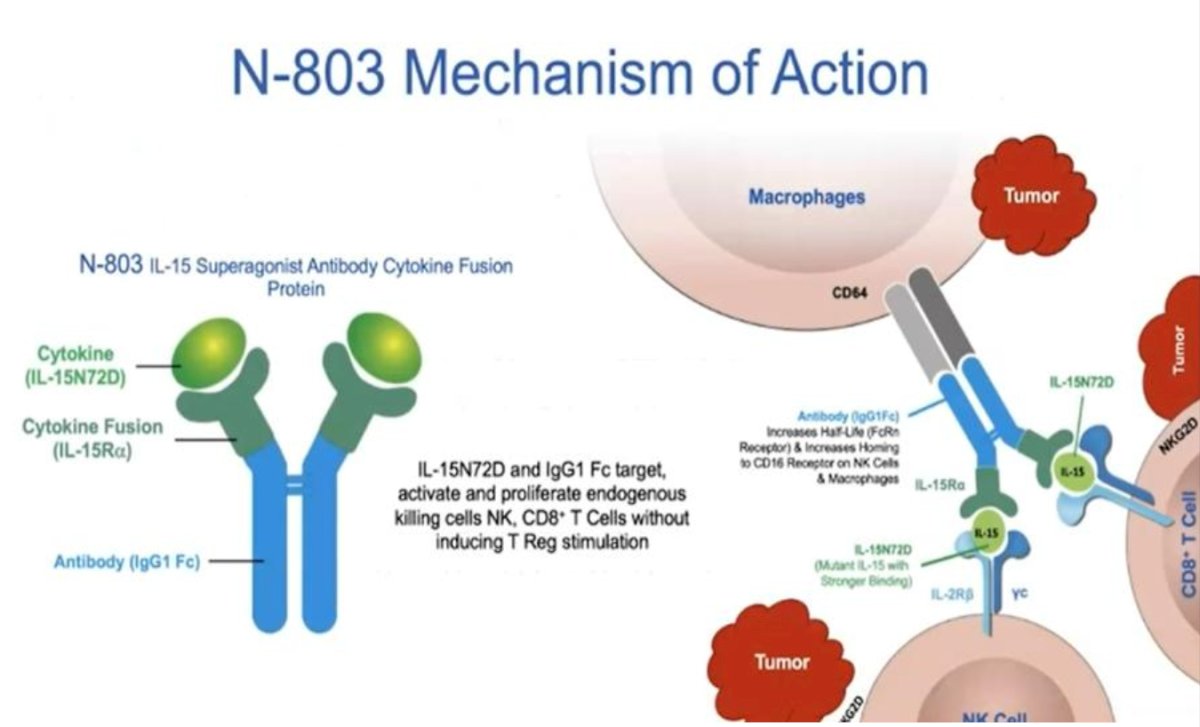
N-803 is given intravesically with an additional BCG course (weekly for 6 weeks), augmenting the immune response to BCG. There are several IL-15 superagonist proposed mechanisms to overcome BCG resistance:
- IL-15 superagonist: Anktiva is a complex that mimics the natural action of dendritic cells, delivering IL-15 to natural killer, CD4, and CD8 T cells
- Activation of immune cells: by binding to IL-15 receptors to immune cells, driving proliferation and activation of natural killer cells and CD8+ killer T cells
- Generation of memory T cells: enhances the generation of memory killer T cells, which are specifically trained to recognize and target cancer cells
- Enhanced immune response: the combination of activated natural killer cells, CD8+ killer T cells, and memory T cells results in a robust and long-lasting immune response against cancer
- Durable complete responses: this mechanism of action leads to durable complete responses, meaning that the cancer cells are effectively eliminated and the immune system remains vigilant against recurrence
QUILT-3.0324 is an ongoing, open label, multicenter, single arm trial that is evaluating intravesical N-803 + BCG or N-803 alone in patients with BCG-unresponsive, high-grade non muscle invasive bladder cancer. This study includes three patient cohorts:
- Cohort A (CIS +/- papillary disease): Intravesical N-803 (400 μg/instillation) + BCG (50 mg/installation) given once weekly for 6 consecutive weeks (induction)
- Cohort B (High grade Ta/T1 papillary disease): N-803 + BCG
- Cohort C (CIS +/- papillary): N-803 alone
In Cohort A, a complete response was observed in 71% of patients (13/58 responders required a re-induction). Response rates were as follows:
- 3 months: 55%
- 6 months: 56%
- 12 months: 45%
- 18 months: 33%
The median duration of response in complete responders was 26.6 months. The 24-month progression-free survival rates was 84.7%: 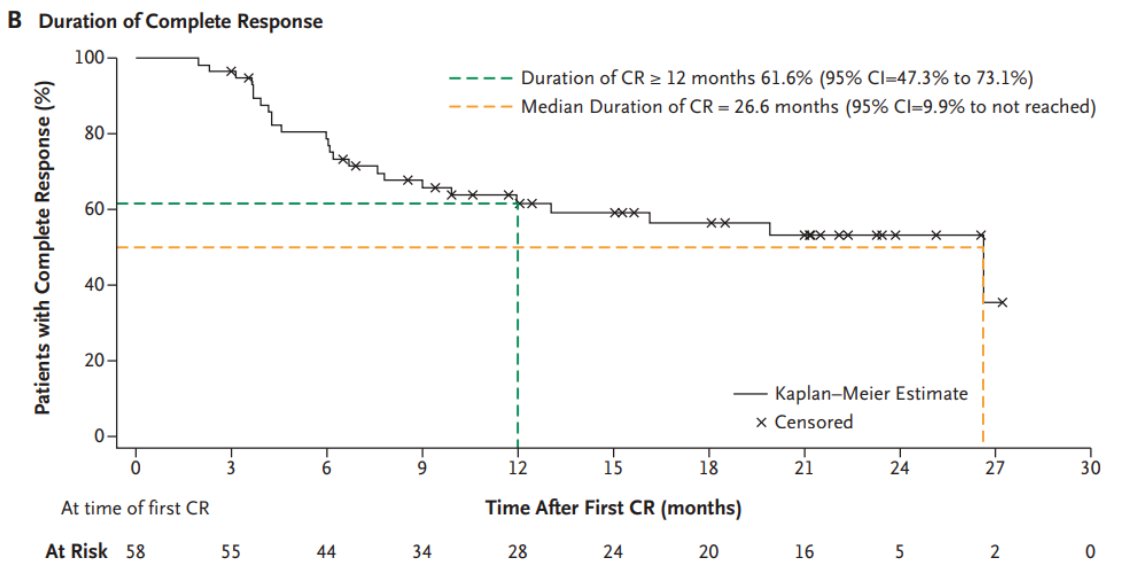
Re-induction therapy in 24 (29%) patients had a complete response rate of 54%.
In 72 evaluable patients in Cohort B, the median disease-free survival was 19.3 months (95% CI 7.4 – NR), with disease-free survival rates as follows:
- 12 months: 55.4% (95% CI 42.0 – 66.8)
- 24 months: 48.3% (95% CI 34.5 – 60.7)
In the 10 evaluable patients in Cohort C, a complete response at 3 months was observed in only 2 (20%) patients with N-803 alone. On the basis of protocol-defined stopping rules, the independent data monitoring committee recommended that cohort C be discontinued for futility. Overall, the probability estimates for cystectomy free survival at 12 months was 94% and at 24 months was 68%.
The most common treatment-related adverse events with the combination of N-803 + BCG were lower genitourinary in nature (dysuria, pollakiuria, hematuria). The incidence of grade 3 or worse adverse events was 23%, most frequently hematuria and urinary tract infections (2% each). One patient experienced a grade 5 treatment-related adverse event (cardiac arrest with subsequent death) and 3 had evidence of immune-related adverse events: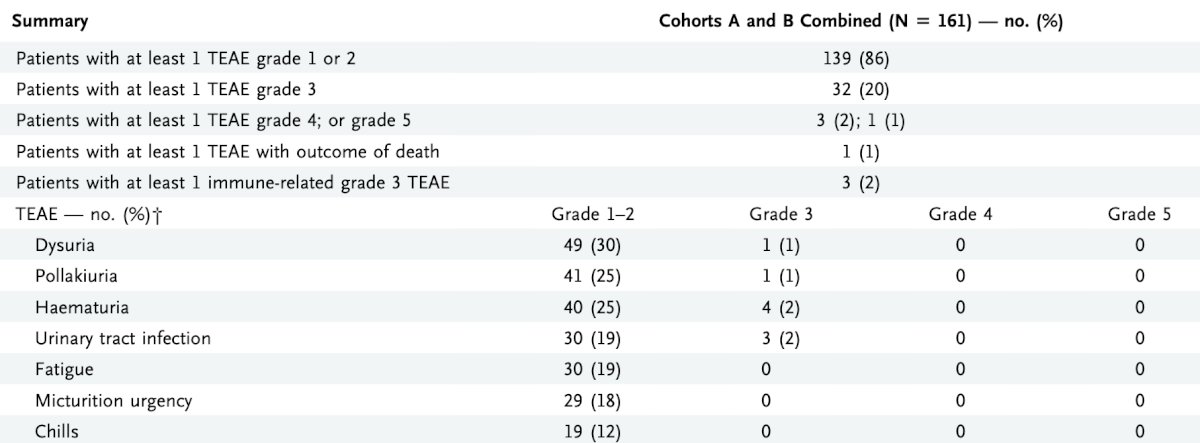
Dr. Bivalacqua then discussed recombination BCG, which is defined as a recombinant vaccine produced through recombinant DNA technology, which involves inserting the DNA encoding an antigen (such as a bacterial surface protein) that stimulates an immune response into bacterial or mammalian cells, expressing the antigen in these cells. VPM1002 has been assessed in a phase 1/2 trial, and is a recombinant, urease C-deficient, listeriolysin expression BCG vaccine strain that was generated in order to induce a broader immune response against mycobacterial antigens.
Recombinant BCG-STING is re-engineered to express a small STING agonist (CDN: c-di-AMP):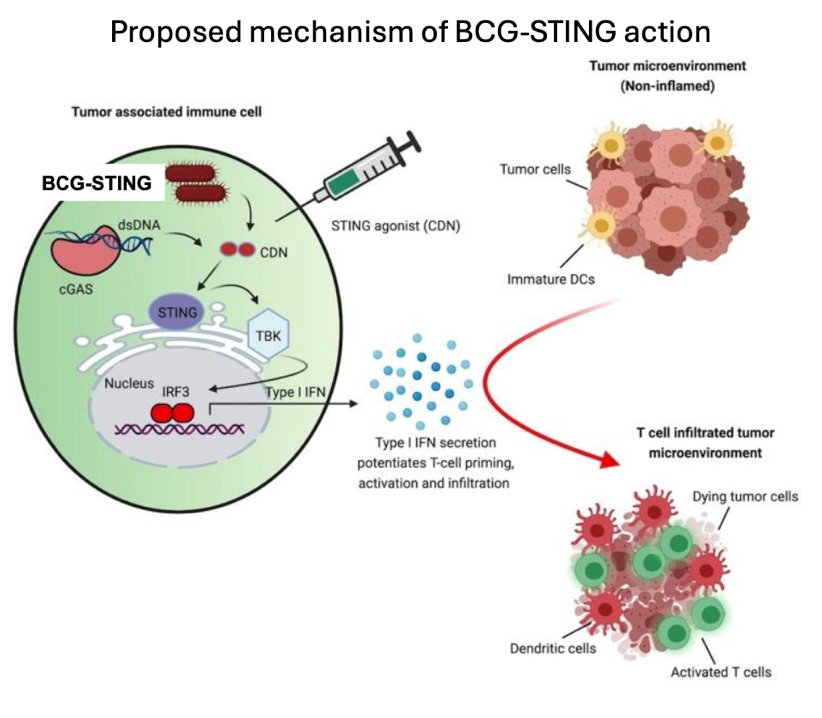
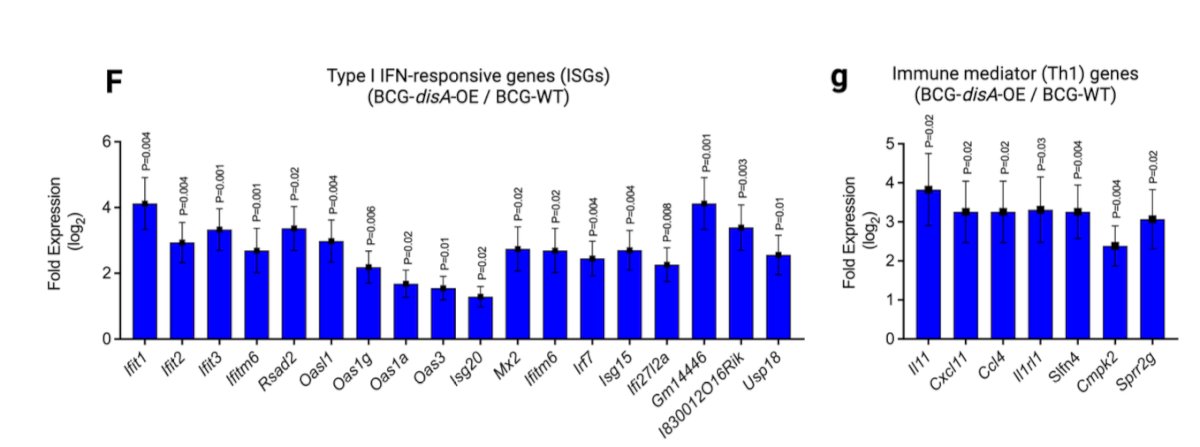
In work from Dr. Bivalacqua’s group, they showed that recombinant BCG-STING is a potent inducer of type I IFN in macrophages in a STING-dependent manner:5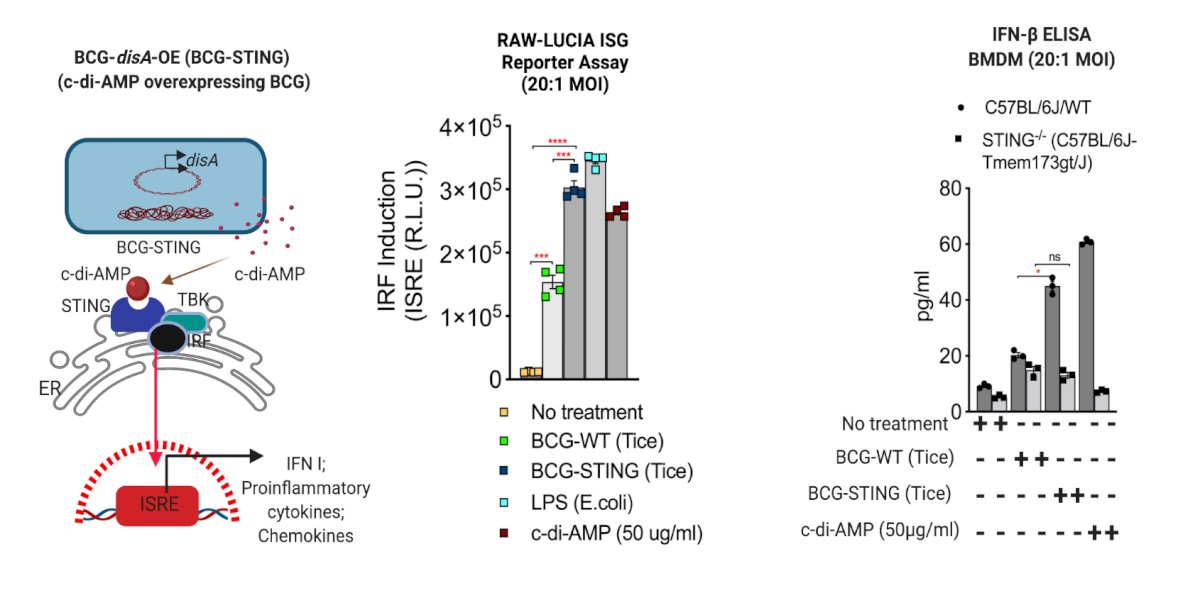
Moreover, BCG-STING treated immunogenic urothelial tumors are highly inflamed: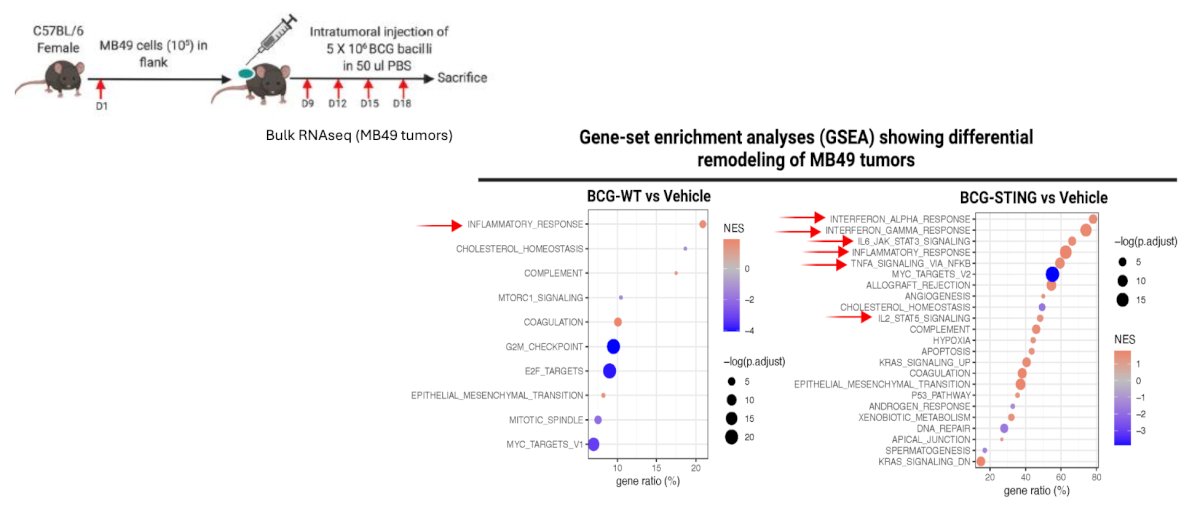
Currently, there is a phase 1/2a clinical trial using recombinant BCG-STING funded by the SBIR. This trial is manufacturing recombinant BCG-STING (OS-151) via a fermentation volume approach for capacity and economies of scale, with the intravesical agent available in the summer of 2025. The phase 1 clinical trial is in intermediate, BCG-unresponsive, and BCG-exposed non muscle invasive bladder cancer patients.
Dr. Bivalacqua concluded his presentation discussing that BCG harnesses local immunomodulators for maximal impact with the following take home points:
- There is a potential role for the combination of systemic (intravesical?) PD-1 inhibition with intravesical BCG, however at what cost (systemic side effects and economically) in BCG naïve (unresponsive?) disease states
- Combination intravesical agents (cytokine based therapy) can be used to augment the local immune response of BCG and is effective in the BCG unresponsive disease state
- Recombinant BCG technologies, like VPM1002 and BCG-STING, as monotherapy may improve to induce the most robust local tissue specific immune response and could be used in multiple disease states (BCG naïve, exposed, and unresponsive)
Presented by: Trinity Bivalacqua, MD, PhD, Director of Urologic Oncology, Co-Director of the Genitourinary Cancer Service Line, Abramson Cancer Center, Professor of Surgery at the Hospital of the University of Pennsylvania, Philadelphia, PA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the European Association of Urology (EAU) 2025 Annual Meeting, Madrid, Spain, Fri, Mar 21 – Mon, Mar 24, 2025.
References:
- Meghani K, Cooley LF, Choy B, et al. First-in-human intravesical delivery of pembrolizumab identifies immune activation in bladder cancer unresponsive to Bacillus Calmette-Guerin. Eur Urol. 2022 Dec;82(6):602-610.
- Balar AV, Kamat AM, Kulkarni GS, et al. Pembrolizumab monotherapy for the treatment of high-risk non-muscle-invasive bladder cancer unresponsive to BCG (KEYNOTE-057): An open-label, single-arm, multicenter, phase 2 study. Lancet Oncol. 2021 Jul;22(7):919-930.
- Boorjian SA, Alemozaffar M, Konety BR, et al. Intravesical nadofaragene firadenovec gene therapy for BCG-unresponsive non-muscle-invasive bladder cancer: A single-arm, open-label, repeat-dose clinical trial. Lancet Oncol. 2021 Jan;22(1):107-117.
- Chamie K, Chang SS, Kramolowsky E, et al. IL-15 Superagonist NAI in BCG-Unresponsive Non-Muscle-Invasive Bladder Cancer. NEJM Evid 2022; 2(1)
- Singh AK, Praharaj M, Lombardo KA, et al. Re-engineered BCG overexpressing cyclic di-AMP augments trained immunity and exhibits improved efficacy against bladder cancer. Nat Commun. 2022;13:878.