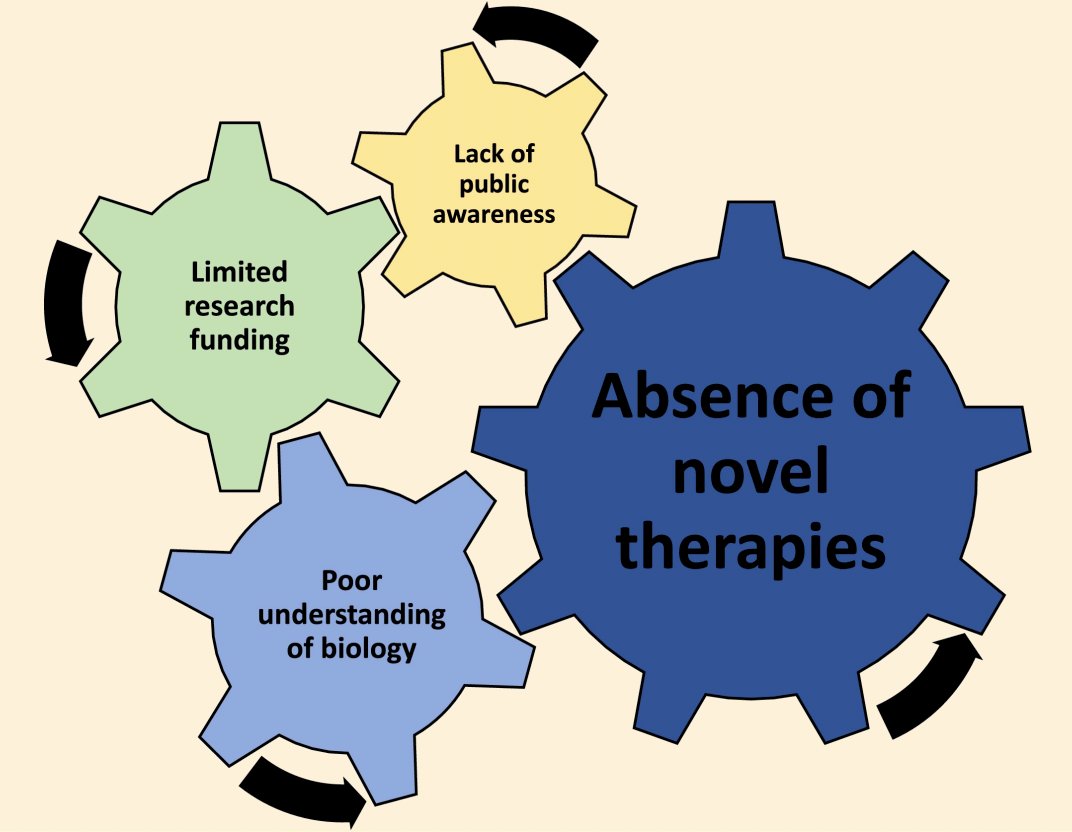
(UroToday.com) The 2025 EAU annual meeting featured a session on intravesical therapy for bladder cancer and a presentation by Dr. Felix Guerrero-Ramos discussing that the bladder as an ideal organ for cutting-edge, device-assisted intravesical drug delivery. Dr. Guerrero-Ramos started his presentation by emphasizing that the reason we are having this debate at EAU is because of (i) a poor understanding of biology, leading to (ii) an absence of novel therapies, leading to (iii) a lack of public awareness, leading to (iv) limited research funding:
Dr. Guerrero-Ramos noted that BCG is a vaccine, and standard of care for high risk non muscle invasive bladder cancer since the 1970s. However, since, then there have been several FDA approvals, including:
- 2020: approval of pembrolizumab for BCG-unresponsive, high risk non muscle invasive bladder cancer based on the KEYNOTE-057 trial (complete response rate of 41% at 3 months)1
- 2022: approval of nadofaragene firadenovec for patients with high risk BCG unresponsive non muscle invasive bladder cancer with CIS +/- papillary tumors (complete response rate of 53.4% at 3 months)2
- 2024: approval of nogapendekin alfa inbakicept for BCG unresponsive non muscle invasive bladder cancer based on the QUILT trial (complete response rate of 71% at any time)3
Additionally, there are several exciting therapeutic options in the pipeline, including (i) cretostimogene grenadenorepvec (75.2% complete response rate at 3 months), (ii) T3011 (71.4% complete response rate at 3 months), (iii) cretostimogene grenadenorepvec + pembrolizumab (82.9% complete response rate at 3 months), and (iv) TAR-200 (83.5% any time complete response rate). Dr. Guerrero-Ramos emphasized that based on a press release from January 15, 2025, a new drug application was initiated with the FDA for TAR-200, the first and only intravesical drug releasing system for patients with BCG-unresponsive non muscle invasive bladder cancer.
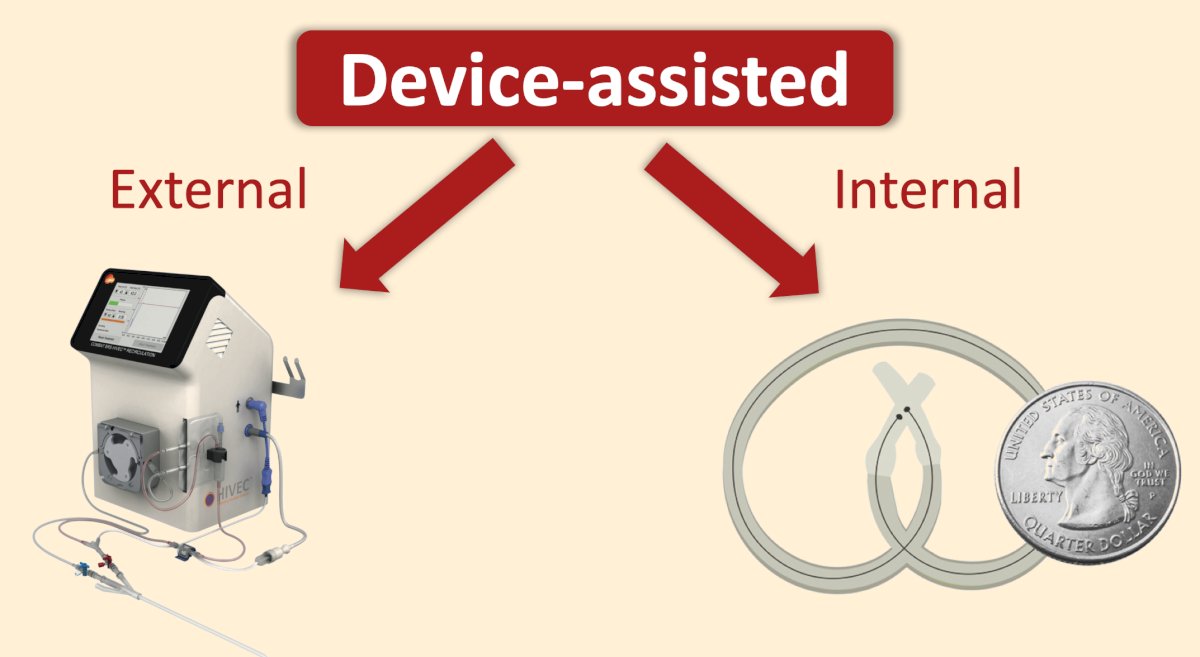
With regards to device-assisted intravesical delivery, there are external and internal options:
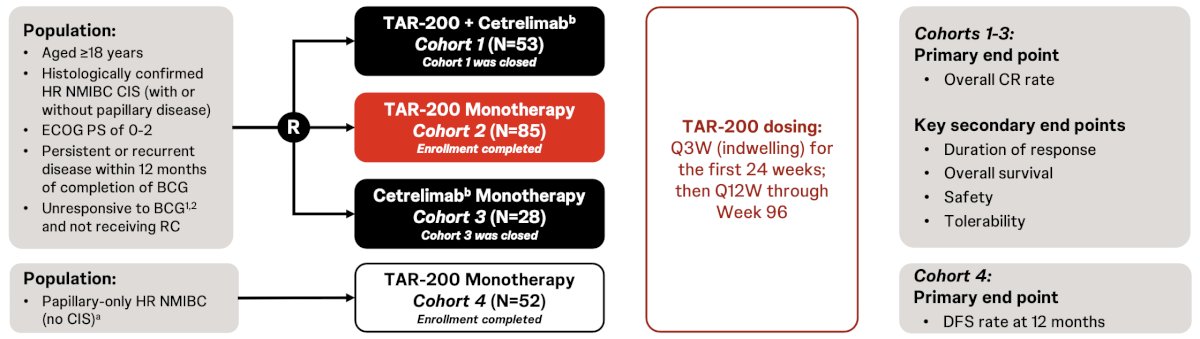
Dr. Guerrero-Ramos then discussed the SunRISe-1 trial, which is an ongoing, randomized, phase 2b study assessing the efficacy and safety of TAR-200 + cetrelimab (anti-PD1) (cohort 1), TAR-200 alone (cohort 2), or cetrelimab alone (cohort 3) in patients with BCG-unresponsive high risk non-muscle invasive bladder cancer non-muscle invasive bladder cancer with CIS ± papillary disease, ineligible for/refusing radical cystectomy. TAR-200 alone is also being assessed in patients with papillary disease only (cohort 4). Eligible patients aged ≥18 years had histologically confirmed CIS ± papillary disease (high-grade Ta, any T1) after adequate BCG, and ECOG performance status 0-2. TAR-200 was dosed every 3 weeks through Week 24, then every 12 weeks until Week 96. Response was assessed by cystoscopy and centrally-assessed urine cytology, CT/MRI, and bladder biopsy (Weeks 24, 48, and as clinically indicated). The primary endpoint was overall complete response rate, and secondary endpoints included duration of response and safety. The SunRISe-1 trial design is as follows:
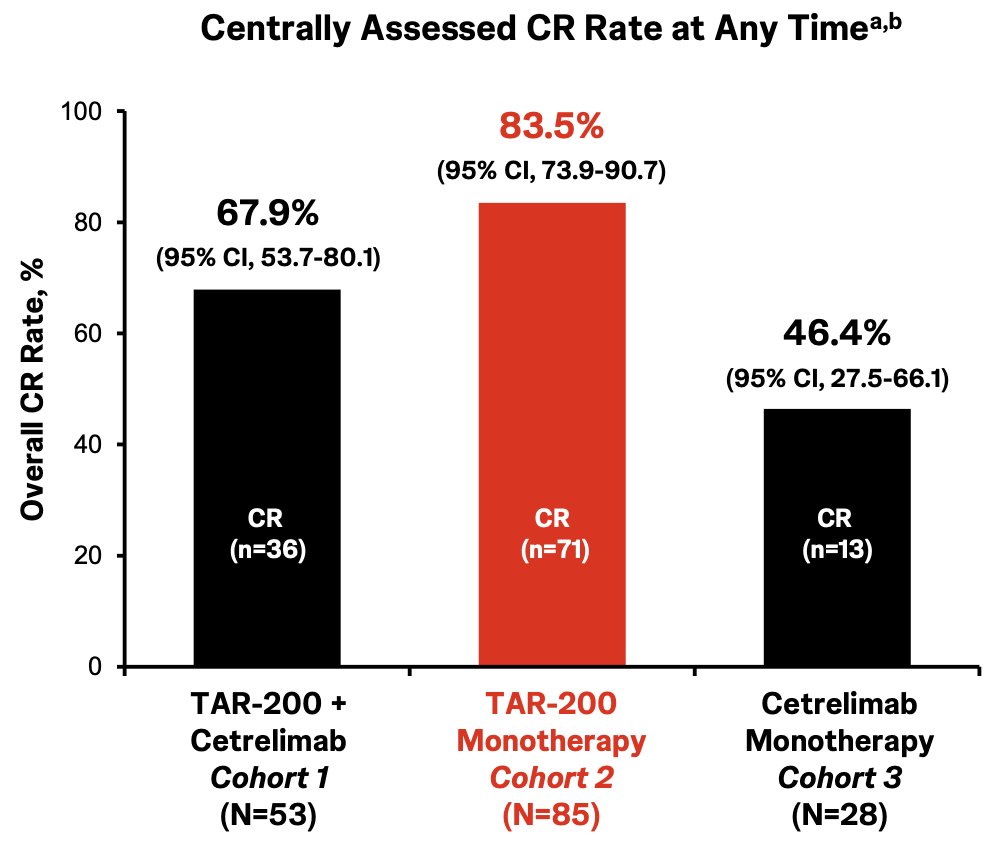
Centrally confirmed complete response rates in Cohort 1, Cohort 2, and Cohort 3 were 67.9%, 83.5%, and 46.4%, respectively:
In Cohort 2, the estimated 12-month complete response rate was 57.4%, the estimated 12-month duration of response rate was 65.7%, median follow-up in responders was 9.2 months (range: 3.7-36.6), and patients remaining in response was 81.6%:

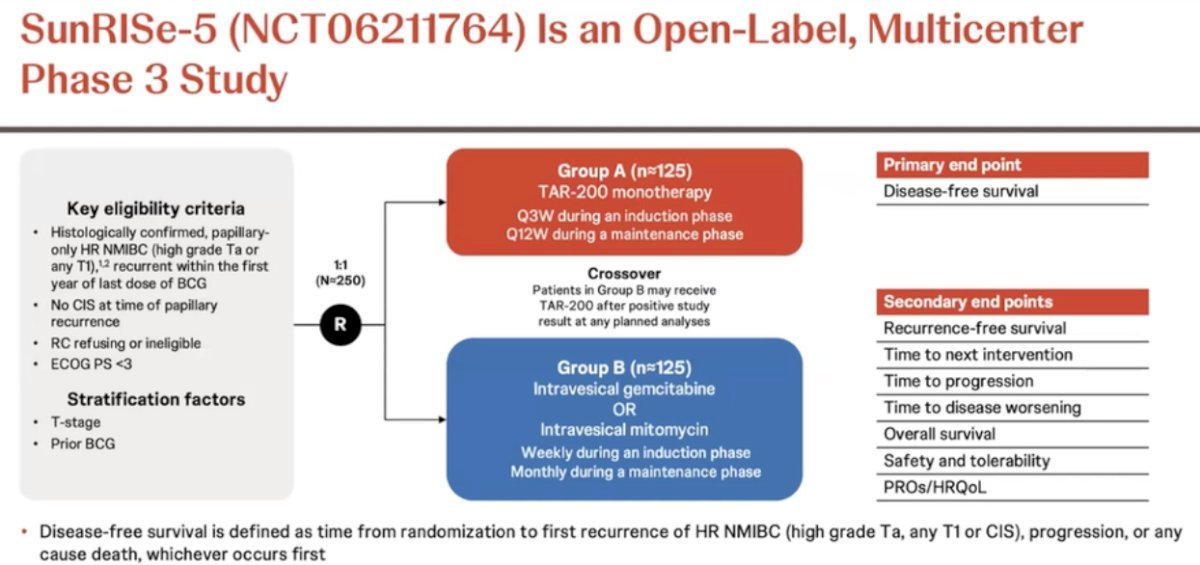
Also part of the SunRISe platform is SunRISe-5, a randomized, open-label, multicenter phase III trial that is evaluating the safety and efficacy of TAR-200 compared with investigator’s choice of intravesical chemotherapy in patients with papillary-only, high-risk NMIBC that recurs within the first year of BCG treatment who either refuse or are ineligible for radical cystectomy. Eligible patients are ≥18 years of age, have an ECOG performance status of 0–2, and were diagnosed ≤90 days of consent with histologically confirmed recurrent, papillary-only high-risk NMIBC (high-grade Ta, any T1, without carcinoma in situ) with last dose of BCG ≤12 months, and who are ineligible for or decline radical cystectomy. Eligible patients (n = 250) will undergo 1:1 randomization to either:
- TAR-200 monotherapy is given every 3 weeks during induction and every 12 weeks during the maintenance phase
- Intravesical gemcitabine or intravesical mitomycin (weekly during induction, monthly during maintenance)
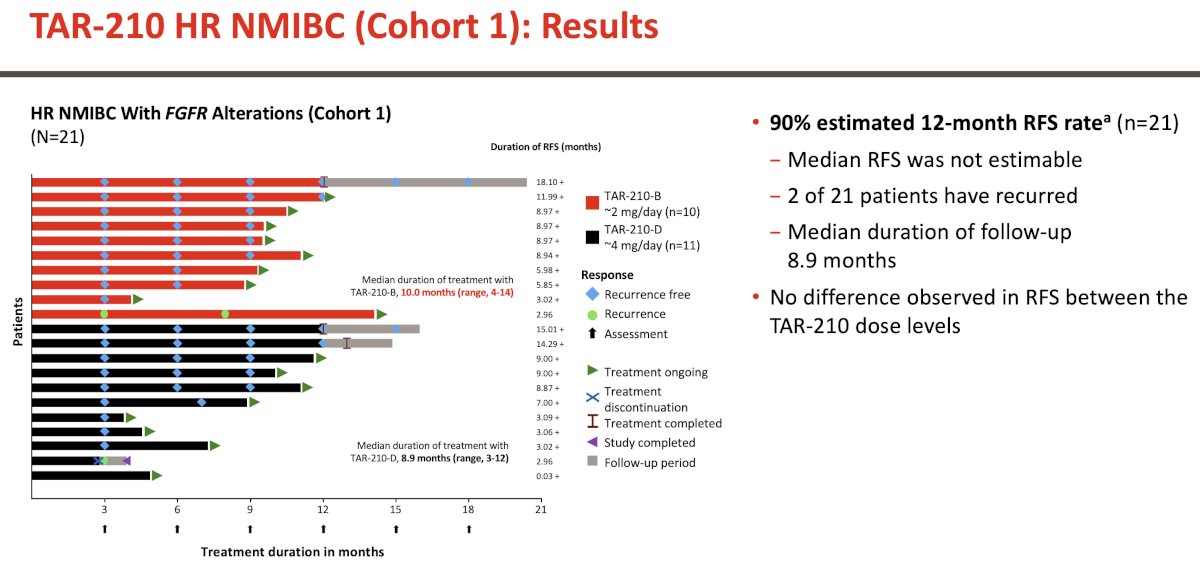
Next, Dr. Guerrero-Ramos discussed TAR-210, a novel erdafitinib intravesical system designed to provide local, sustained release of erdafitinib within the bladder over 12-week cycles while limiting systemic toxicities. A recent open-label, multicenter phase 1 study evaluated the safety, pharmacokinetics, and efficacy of TAR-210 in patients with non-muscle invasive bladder cancer whose tumors harbor select FGFR alterations. In cohort 1, 90% of patients were recurrence free at 12 months, the median recurrence free survival was not estimable, and the median duration of follow-up was 8.9 months:
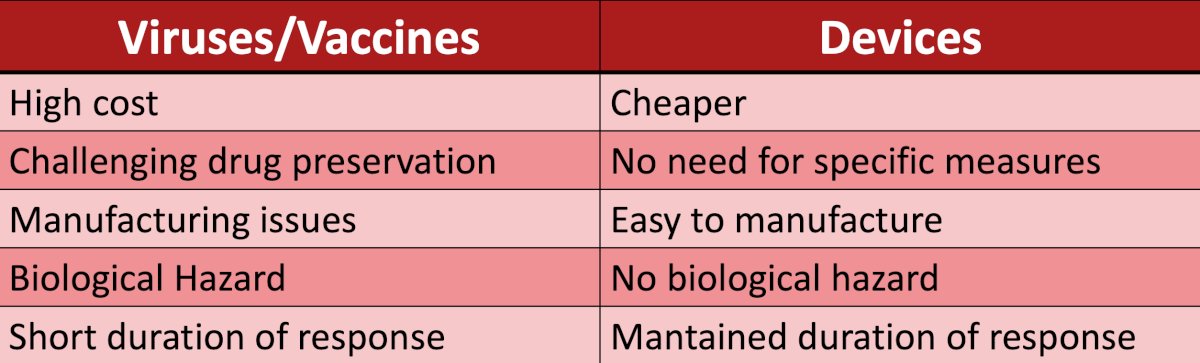
The following table compares viruses/vaccines and devices:
Finally, Dr. Guerrero-Ramos highlighted that there are more “device assisted” options coming, including urease-powered nanobots for radionuclide bladder cancer therapy.
Dr. Guerrero-Ramos concluded his presentation discussing that the bladder as an ideal organ for cutting-edge, device-assisted intravesical drug delivery with the following take home points:
- There are internal versus external assisted devices
- There are currently scarce alternatives, but more options are coming
- Device assisted intravesical delivery is easy to manufacture and preserve, there is no risk of biological hazard, and there is very promising data coming
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain between March 21st and 24th 2025
References:
- Balar AV, Kamat AM, Kulkarni GS, et al. Pembrolizumab monotherapy for the treatment of high-risk non-muscle-invasive bladder cancer unresponsive to BCG (KEYNOTE-057): An open-label, single-arm, multicenter, phase 2 study. Lancet Oncol. 2021 Jul;22(7):919-930.
- Boorjian SA, Alemozaffar M, Konety BR, et al. Intravesical nadofaragene firadenovec gene therapy for BCG-unresponsive non-muscle-invasive bladder cancer: A single-arm, open-label, repeat-dose clinical trial. Lancet Oncol. 2021 Jan;22(1):107-117.
- Chamie K, Chang SS, Kramolowsky E, et al. IL-15 Superagonist NAI in BCG-Unresponsive Non-Muscle-Invasive Bladder Cancer. NEJM Evid 2022; 2(1)