(UroToday.com) The 2025 European Association of Urology (EAU) Annual Congress held in Madrid, Spain was host to a thematic session of rapid-fire debates regarding common problems and controversies in bladder cancer. For patients with cT2N3 bladder cancer who achieve a complete or partial response after 6 cycles of gemcitabine + cisplatin, Drs. Shilpa Gupta and Félix Guerrero-Ramos debated whether continued systemic therapy versus surgical consolidation is the optimal approach in this setting.
Dr. Marek Babjuk began with a case presentation of a 71-year-old female with a past medical history of cerebral ischemia (2011), hypertension, and a remote smoking history who was diagnosed with muscle invasive bladder cancer (MIBC; cT2 – incomplete TURBT) and on staging scans found to have enlarged right internal and common iliac lymph nodes measuring ~2.5 cm.
She received 5 cycles of gemcitabine + cisplatin, with the 6th cycle aborted due to the development of neutropenia. Repeat staging scans following chemotherapy demonstrated a complete response. Dr. Babjuk posed the following questions:
- What is the best approach for this patient with a complete response?
- Alternatively, if this patient had only a partial response or had persistently positive para-aortic lymph nodes, what is the best next step?
Dr. Gupta began her argument in favor of continued systemic therapy in this patient highlighting the following key points:
- Patients with cN+ urothelial carcinoma of the bladder have a high risk of distant metastases and poor prognoses
- The standard of care is poorly defined for cN+ urothelial carcinoma patients
- Available evidence mainly stems from observational studies with marked heterogeneity in outcomes
- Despite advancements in systemic therapies for metastatic urothelial carcinoma, there is a lack of consensus regarding the optimal management of cN+ patients
What are the challenges with defining standard therapy for cN+ patients?
- cN+ urothelial carcinoma patients remain a rare population (<10%)
- Our current knowledge of the true oncologic benefit of consolidative surgery is limited due to a lack of randomized trials
- There is a selection bias regarding the definition and extent of nodal involvement in observational surgical studies
- The data on outcomes following pathologic downstaging after induction chemotherapy in cN+ patients is limited to retrospective data
- These patients are historically excluded from neoadjuvant trials
- In trials of 1st line systemic therapy, the outcomes of these patients are classically pooled with those of patients with metastatic urothelial carcinoma
- cN+ patients have accounted for up to 28% of the study populations of key trials, including KEYNOTE-361, DANUBE, and IMvigor130
- The role of consolidative local therapy remains unaddressed in these patients
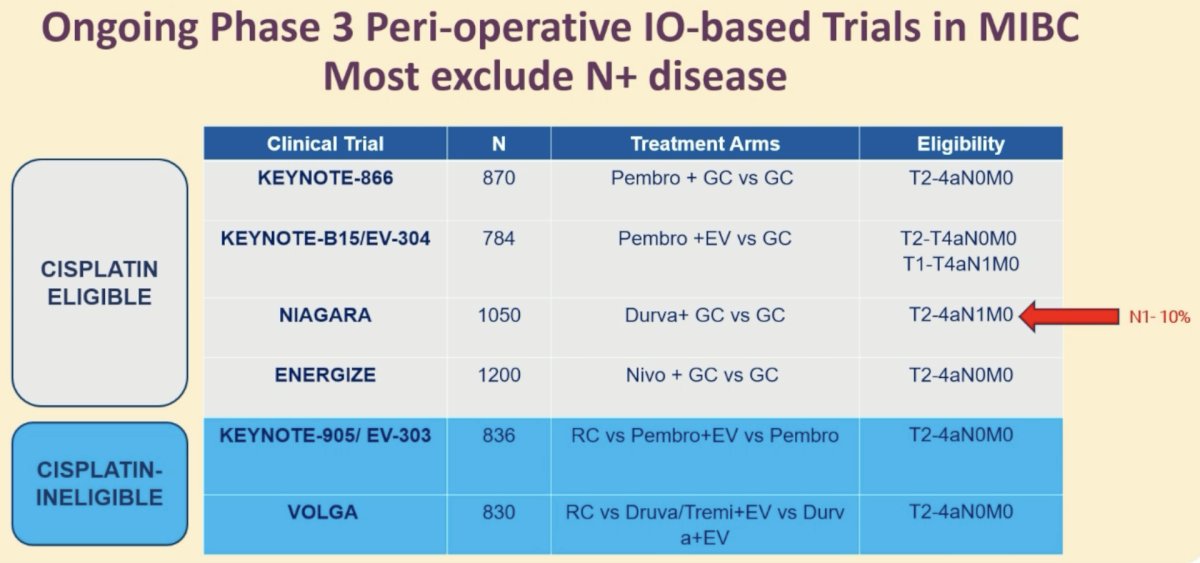
While cN+ patients have accounted for a significant proportion of study populations from key trials, the majority of ongoing phase III trials of perioperative immunotherapy in MIBC exclude patients with cN+ disease. An exception to this is the NIAGARA trial,1 whereby cN1 patients accounted for ~10% of the study cohort.
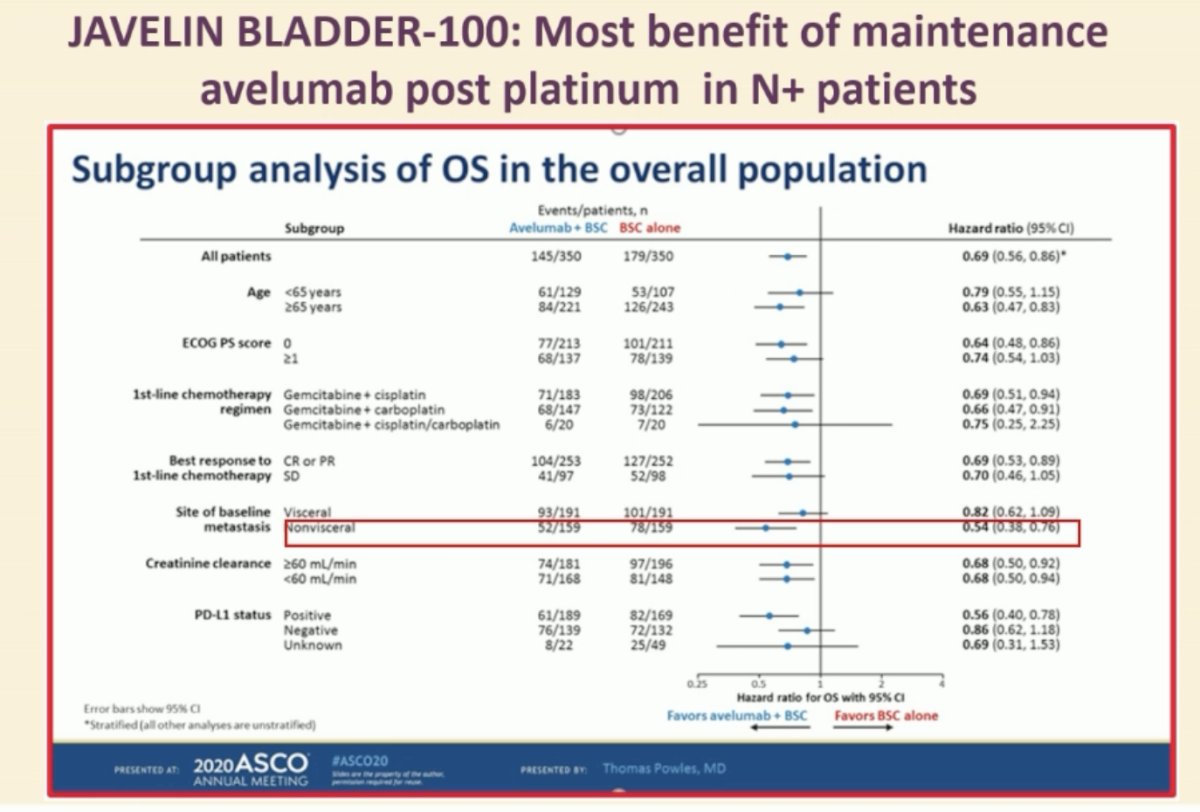
With regards to optimal consolidative therapy following a complete or partial response to cisplatin-based chemotherapy, Dr. Gupta highlighted the JAVELIN-100 trial of maintenance avelumab in MIBC patients who did not experience disease progression following Gem-Cis or Gem-Carbo. As seen in the forest tree below, patients with non-visceral (i.e., nodal or bone) metastases derived a significant overall survival benefit with maintenance avelumab versus best supportive care (HR: 0.54, 95% CI: 0.38–0.76).2
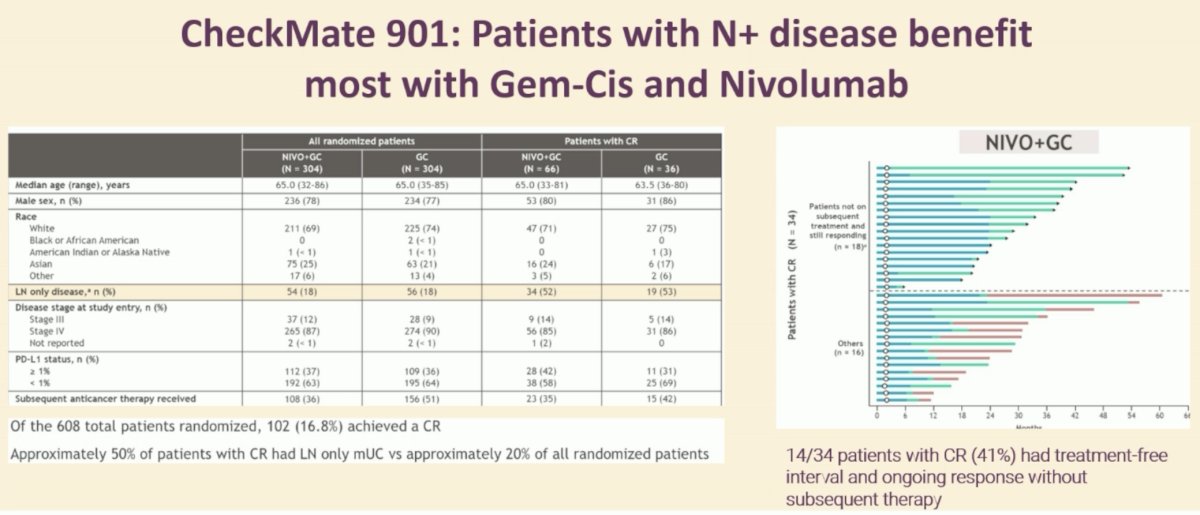
In the CheckMate-901 trial of Gem-Cis +/- nivolumab, patients with LN-only disease had excellent outcomes with systemic therapy, whereby a complete response was observed in just over half of patients (52–53%) in both the intervention and control arms. Significantly, 14/34 (41%) patients with a CR remain treatment-free with no evidence of disease recurrence.3
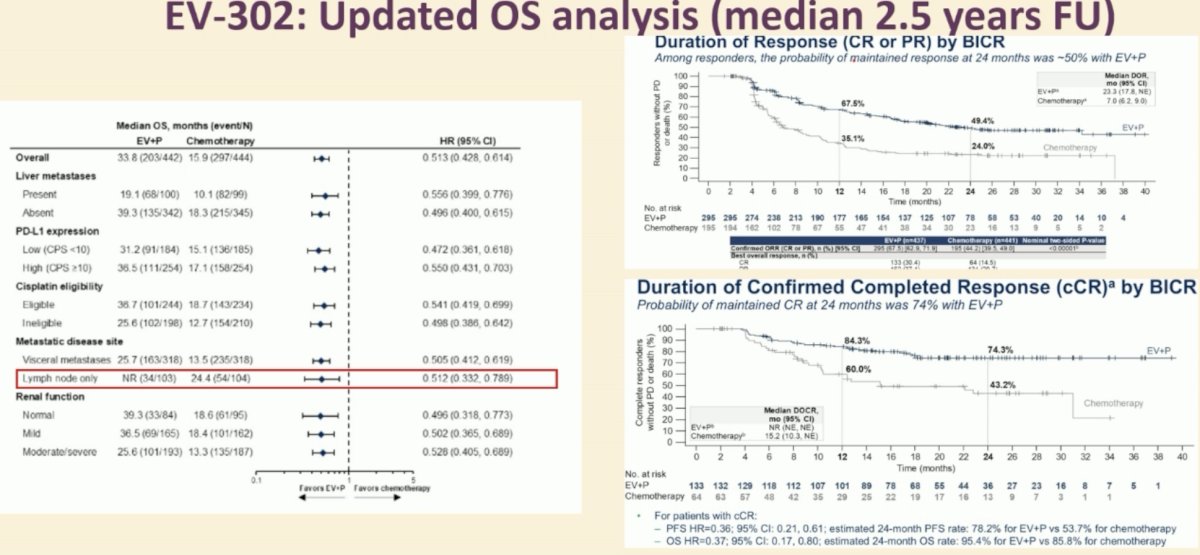
In the EV-302 trial, a survival benefit with enfotumab vedotin + pembrolizumab was observed in all subgroups, including patients with lymph node only disease (HR: 0.51, 95% CI: 0.33–0.79), with improved durations of complete response, compared to platinum-based combination chemotherapy.4
To conclude her argument in favor of systemic therapy, Dr. Gupta emphasized that:
- This patient who achieved a complete response with Gem-Cis should be offered maintenance avelumab, with no role for surgery.
- Based on the practice changing data from phase III trials (JAVELIN 100, EV-302, CheckMate-901), systemic therapy improves overall survival in patients with locally advanced disease.
- Therefore, surgery is redundant for patients with cN+ disease achieving a complete or partial response in the current therapeutic era.
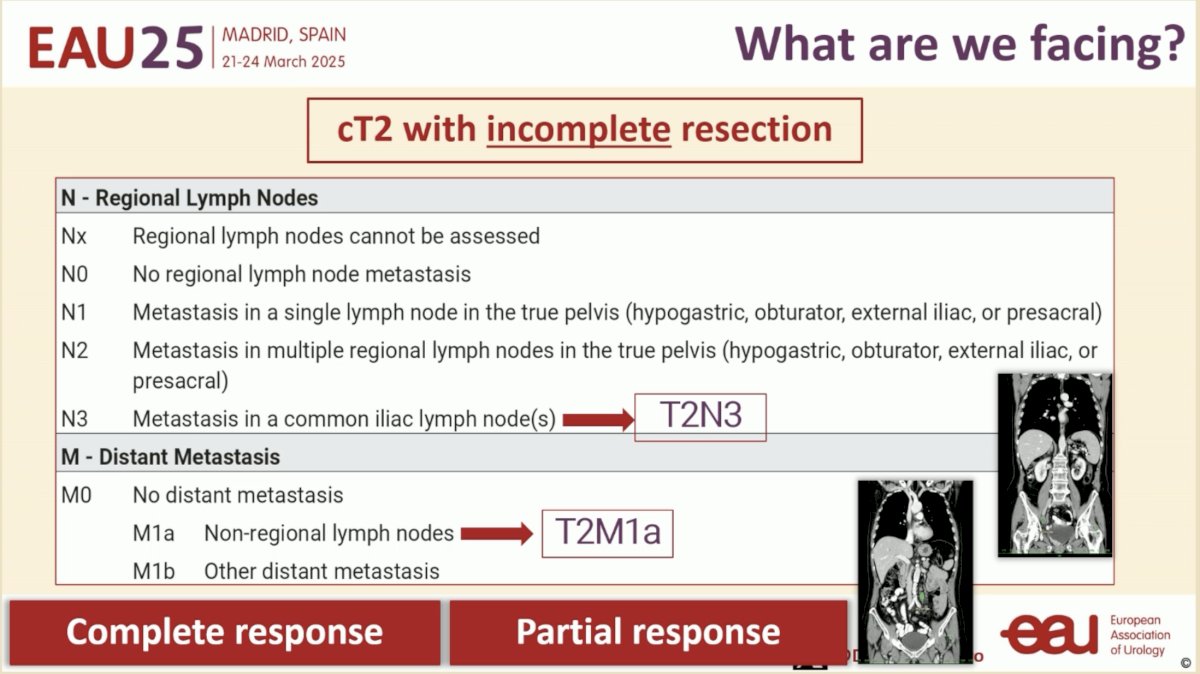
Next, Dr. Félix Guerrero-Ramos argued in favor of surgical consolidation in this setting. What is the issue we are facing with this patient? This is a patient with either cT2N3 disease or cT2M1a disease, depending on whether disease is limited to the pelvic lymph nodes or extends to the retroperitoneum. However, irrespective of clinical staging, this patient with a ‘complete’ or ‘partial’ response on imaging still likely has residual disease in her bladder following an incomplete TURBT.
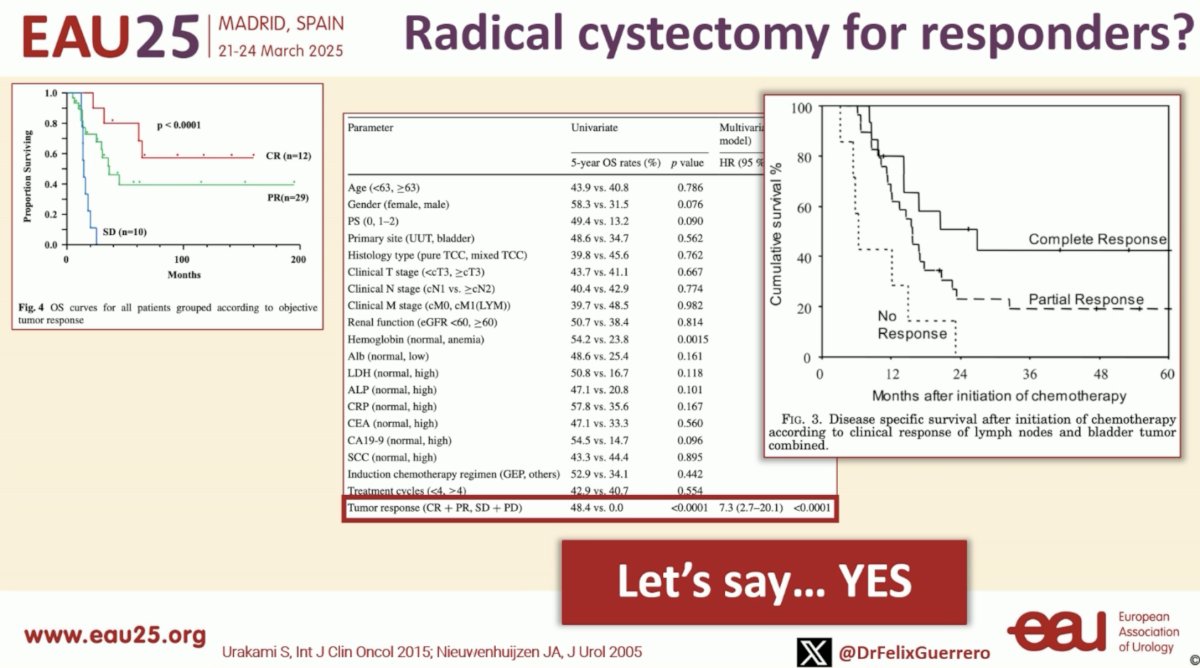
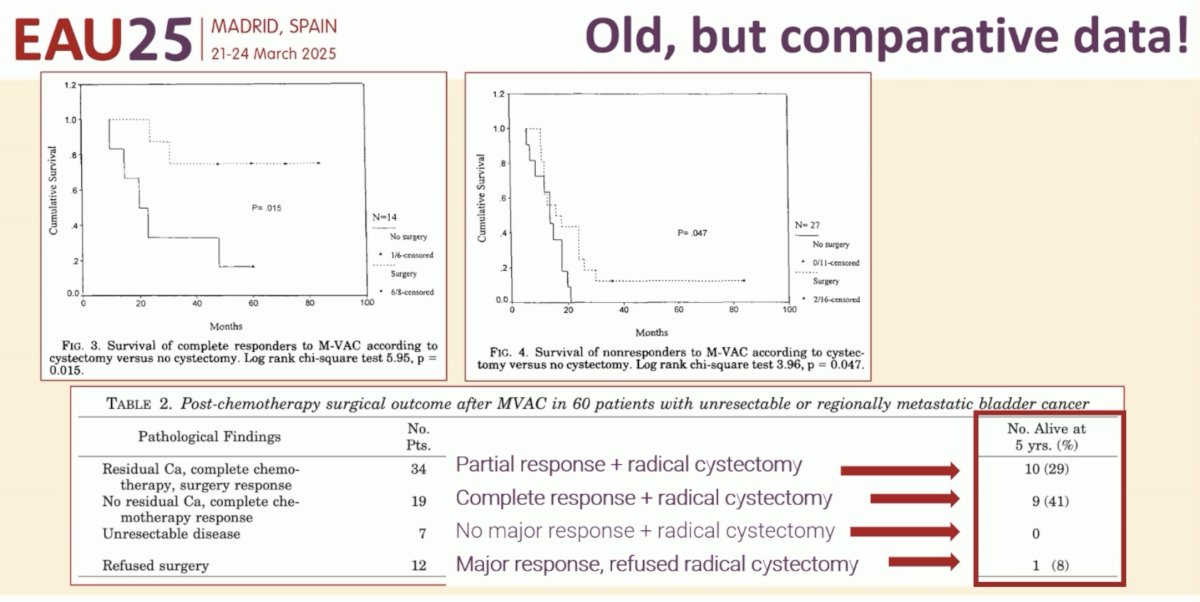
He argued that these are the patients that benefit the most from consolidative therapy with a radical cystectomy. Data from observational studies have demonstrated that patients with a complete or partial response who undergo a radical cystectomy have significantly better survival outcomes, compared to those with stable/progressive disease who undergo surgery (median 5-year overall survival: 48.4 versus 0 months, p<0.0001).
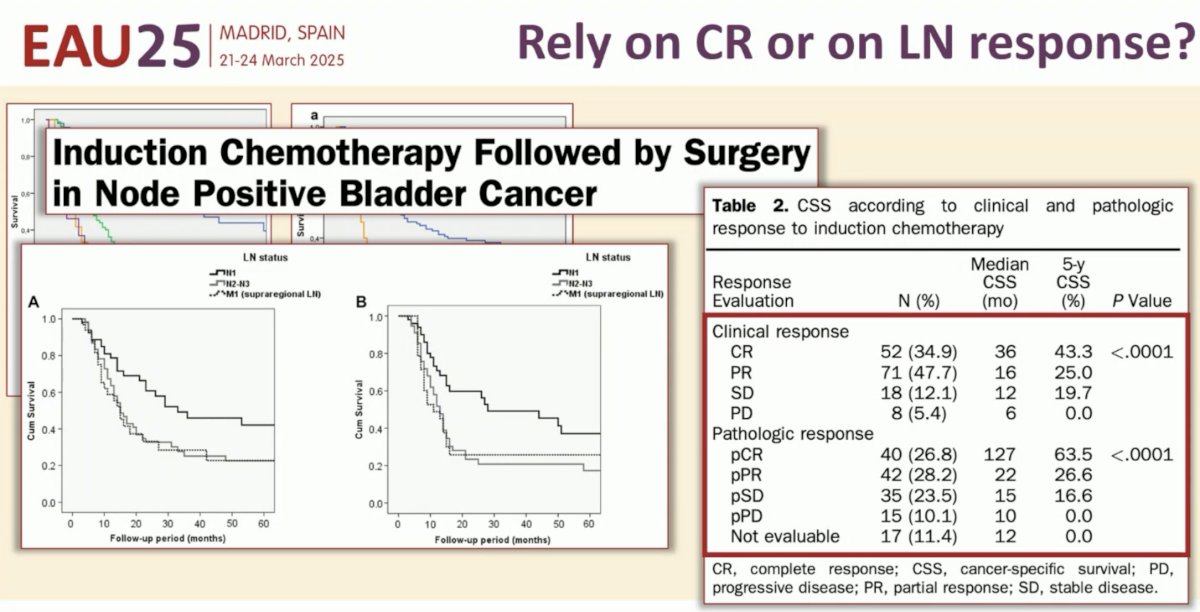
Irrespective of whether patients have a clinical or pathologic complete response, induction chemotherapy followed by surgery in node-positive bladder cancer patients is associated with excellent survival outcomes.
But some may argue that surgery may be overtreatment for these patients with a pathologic complete response. Dr. Guerrero-Ramos countered that argument by noting that:
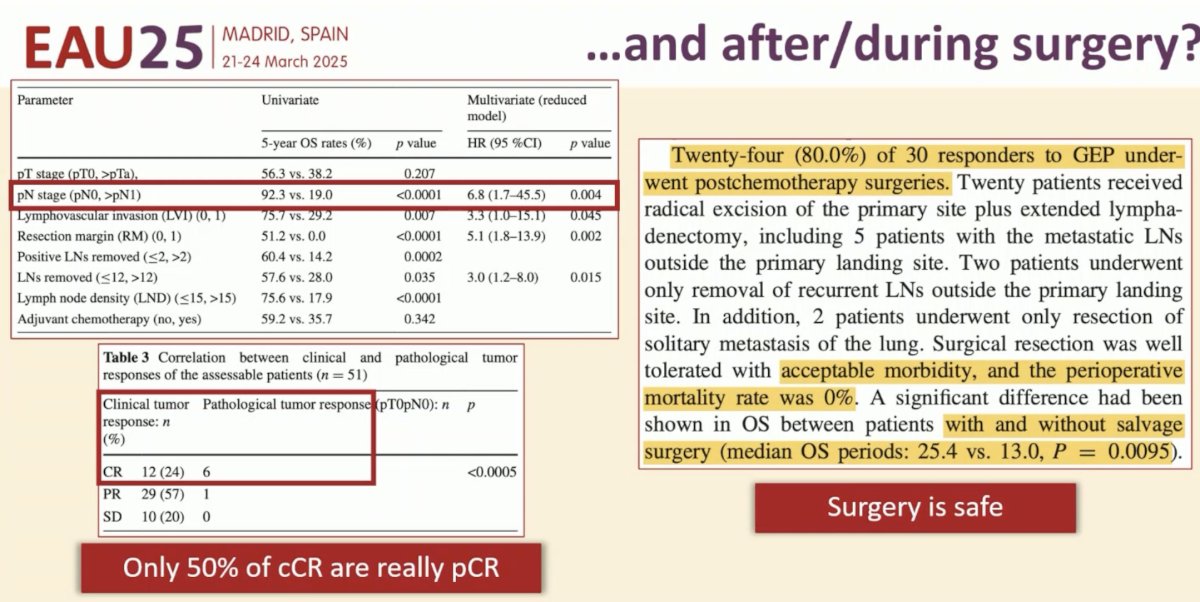
- Patients with pN0 disease who undergo radical cystectomy have superior survival outcomes with radical cystectomy, compared to those with ≥pN1 disease
- Only 50% of clinical complete responders actually have a pathologic complete response Cannot reliably identify patients appropriate for bladder-sparing approaches at the current time
- Surgery in these patients is safe
Further support for radical cystectomy in this setting comes from the MSKCC series with reports demonstrating that a significant proportion of MIBC patients with a complete or partial response following MVAC chemotherapy can experience long-term survival.
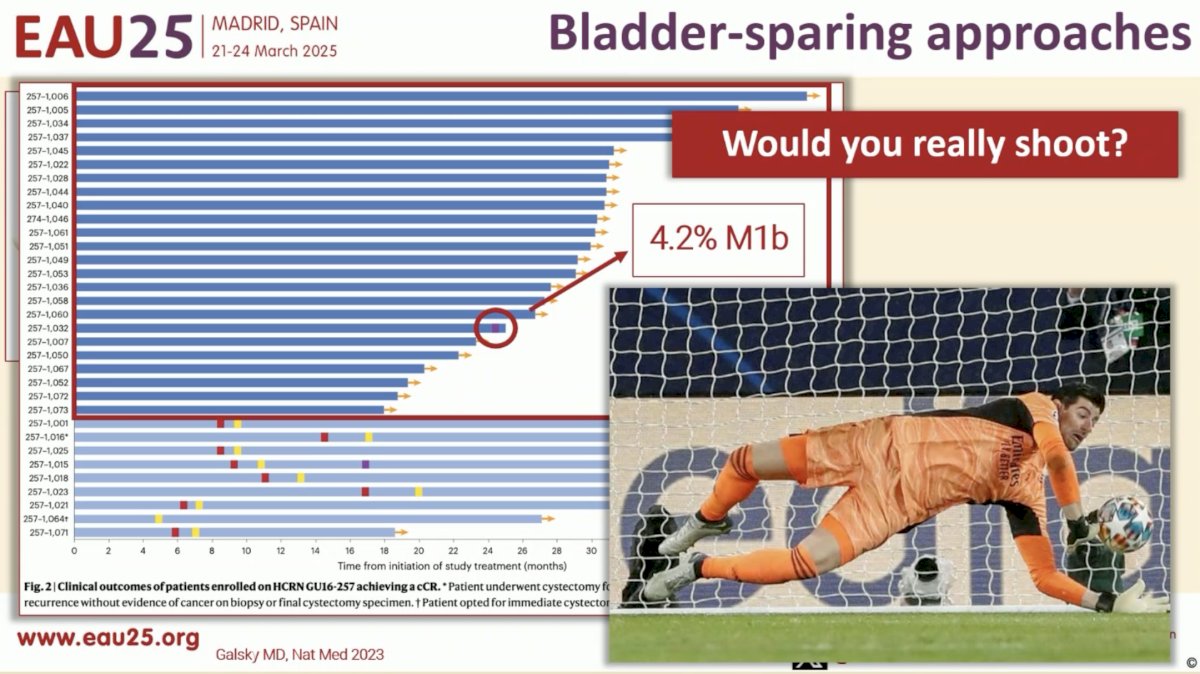
He further argued that we should apply lessons learned from earlier MIBC stages in patients who have achieved a complete response to the patient in the case example. In the HCRN GU 16-257 phase II trial, cisplatin-eligible cT2-T4aN0M0 urothelial bladder cancer patients received 4 cycles of gemcitabine, cisplatin, plus nivolumab followed by clinical restaging with urine cytology, MRI/CT of the bladder, cystoscopy and bladder biopsies. Patients achieving a complete response (normal cytology, imaging, and cT0/Ta) were eligible to proceed without cystectomy and received nivolumab every 2 weeks x 8 followed by surveillance. Patients not achieving a clinical complete response were recommended to undergo cystectomy. Notably, in this trial, 4.2% of ‘complete responders’ who forgoed a radical cystectomy developed subsequent M1b disease,5 with Dr. Guerrero-Ramos arguing that this proportion is much higher than what is acceptable in this setting and supports radical cystectomy for this patient.

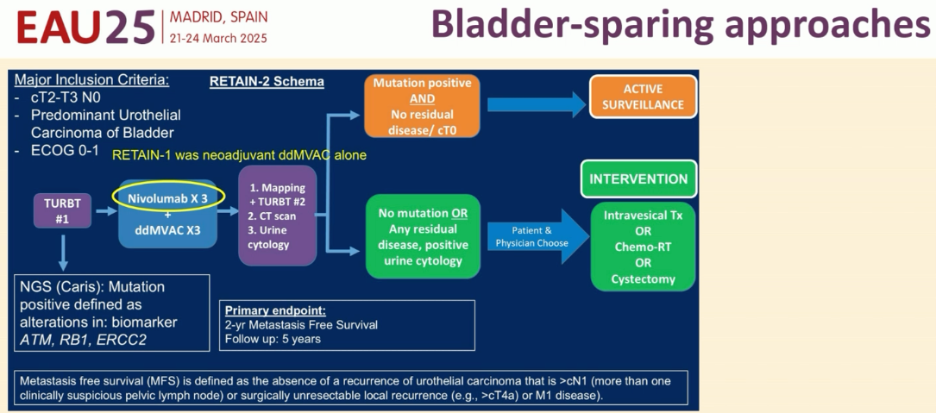
In the bladder-sparing RETAIN-2 trial of ddMVAC + nivolumab, 18% of patients opting for surveillance following systemic therapy developed metastatic disease, again suggesting that current tools available for assessing complete responses are not yet ‘ready for primetime’, and these lessons should be applied to patients with cN+ disease who similarly ‘respond’ to systemic therapy.
Dr. Guerrero-Ramos concluded his argument in favor of surgical consolidation for cN+ patients with a complete/partial response to systemic therapy as follows:
- Surgery is recommended for complete responders and debatable for partial responders
- The lymph node response is relevant
- Surgery is safe
- Decisions should be individualized within the context of a multidisciplinary approach
- We need better tools to assess for complete clinical responses
- Future trials of systemic therapy for locally advanced or metastatic urothelial carcinoma patients should incorporate randomization to radical cystectomy if a complete/partial response is achieved.
Presented by:
- Shilpa Gupta, MD, Professor, Director of the Genitourinary Medical Oncology at Taussig Cancer Institute and Co-Leader of the Genitourinary Oncology Program at Cleveland Clinic, Cleveland, OH
- Félix Guerrero-Ramos, MD, PhD, FEBU, Department of Urology, Hospital Universitario 12 de Octubre, Madrid, Spain
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain between March 21st and 24th 2025
References:
- Powles T, Catto JWF, Galsky MD, et al. Perioperative Durvalumab with Neoadjuvant Chemotherapy in Operable Bladder Cancer. N Engl J Med. 2024; 391(19): 1773-86.
- Powles T, Park SH, Voog E, et al. Avelumab Maintenance Therapy for Advanced or Metastatic Urothelial Carcinoma. N Engl J Med. 2020; 383: 1218-30.
- Van der Heijden MS, Sonpavde G, Powles T, et al. Nivolumab plus Gemcitabine–Cisplatin in Advanced Urothelial Carcinoma. N Engl J Med. 2023; 389: 1778-9.
- Powles T, Valderrama BP, Gupta S, et al. Enfortumab Vedotin and Pembrolizumab in Untreated Advanced Urothelial Cancer. N Engl J Med. 2024; 390: 875-88.
- Galsky MD, Daneshmand S, Izadmehr S, et al. Gemcitabine and cisplatin plus nivolumab as organ-sparing treatment for muscle-invasive bladder cancer: a phase 2 trial. Natt Med. 2023; 29(11): 2825-34.