(UroToday.com) The 2025 European Association of Urology (EAU) Annual Congress held in Madrid, Spain between March 21st and 24th 2025, was host to a thematic session of rapid-fire debates about common problems and controversies in bladder cancer. Drs. Comron Hassanzadeh and Andrea Necchi debated radiation therapy versus systemic therapy as the optimal approach for the management of isolated pelvic recurrences following a radical cystectomy in patients with positive soft tissue surgical margins.
Dr. Hassanzadeh began with a case presentation of a 72-year-old male with an excellent performance status, history of hypertension and gout, who presented with gross hematuria in July 2023. He underwent a cystoscopy and CT urogram with evidence of bulky muscle invasive bladder cancer (MIBC) in September 2023. MRI demonstrated likely cT3 disease possibly involving a peritoneal fold.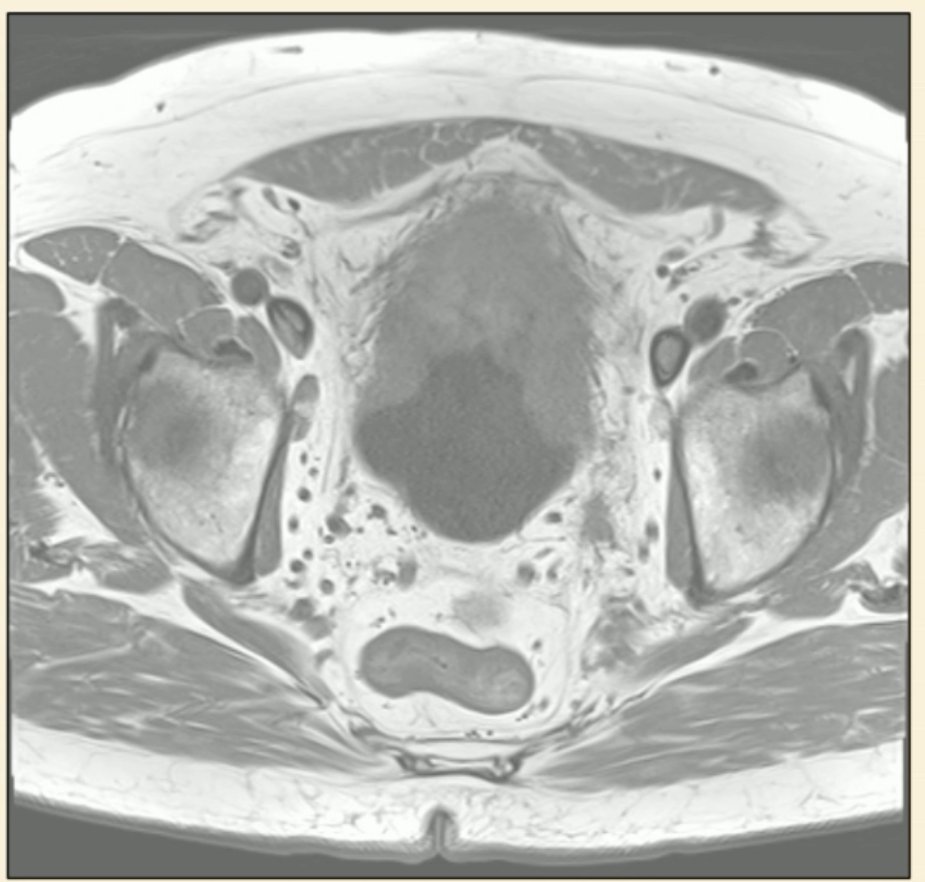
The patient subsequently developed severe, recurrent gross hematuria requiring multiple admissions and proceeded directly to radical cystectomy without neoadjuvant therapy in December 2024. The final pathology was pT3bN0R1, with residual disease present at the left circumferential margin.
There was no evidence of disease recurrence on surveillance CT imaging performed at 3 and 6 months post-operatively. However, at 12 months, the patient was found to have a left pelvic recurrence (no other sites of disease spread) and was otherwise asymptomatic.
Dr. Hassanzadeh briefly argued that this patient likely should have been recommended for adjuvant radiotherapy given his high-risk pathologic features. The current EAU MIBC guidelines recommend offering adjuvant radiotherapy following radical cystectomy to patients with pT3b-4, pN+, and/or positive surgical margins to improve locoregional relapse-free survival, although overall survival benefits for such an approach are unclear.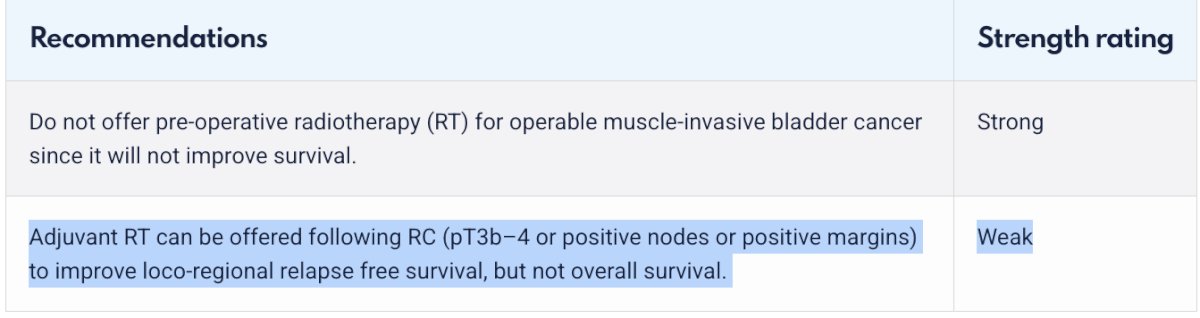
One of the common arguments against the routine use of adjuvant radiotherapy in this setting has been concerns regarding the bowel toxicity of pelvic radiotherapy. With the removal of the bladder/prostate in men undergoing a cystoprostatectomy, there have long been concerns that the bowel being displaced into the vacant pelvis would receive a prohibitively high amount of radiation leading to significant bowel toxicity.
However, at ASTRO 2024, Dr. Vedang Murthy presented the Bladder Adjuvant RadioTherapy (BART) trial, an Indian multicenter phase III trial that randomized 153 high-risk muscle-invasive bladder cancer patients to either adjuvant radiotherapy (50.4 Gy in 28 fractions) or observation. All patients were treated with intensity-modulated, image-guided radiotherapy, and contouring was performed according to the 2016 IJROBP consensus guidelines.
From a toxicity standpoint, in the acute setting., none of the patients had to discontinue radiotherapy secondary to toxicity. Grade 2 acute toxicity was observed more commonly in the radiotherapy arm (17.5% versus 1.4%) and were most commonly bowel symptoms that self-resolved and did not require surgical intervention or inpatient hospitalization. Grade 3 events were observed less frequently in the radiotherapy arm (1.6% versus 4.1%). Notably, 67% of patients who received radiotherapy experienced no symptoms. At a median follow-up of 27 months, late grade 2 adverse events were observed in 15% of radiotherapy-treated patients and 7% of patients in the observation arm. Conversely, grade 3/4 adverse events were observed less frequently in the radiotherapy arm (8.4% versus 10.5%).1
Based on these results, Dr. Hassanzadeh argued that adjuvant/salvage radiotherapy using contemporary contouring and dose modulating approaches in this setting has a more favorable side effect profile than has been historically reported and is safe approach for patients with high-risk pathologic features, such as the patient in this case presentation.
Next, Dr. Andrea Necchi argued in favor of systemic therapy. He noted that current international guidelines, including the ESMO guidelines summarized below, all recommend systemic therapy for this patient, who, by definition, has now developed metastatic disease, and, thus, should be treated with 1st line systemic therapy.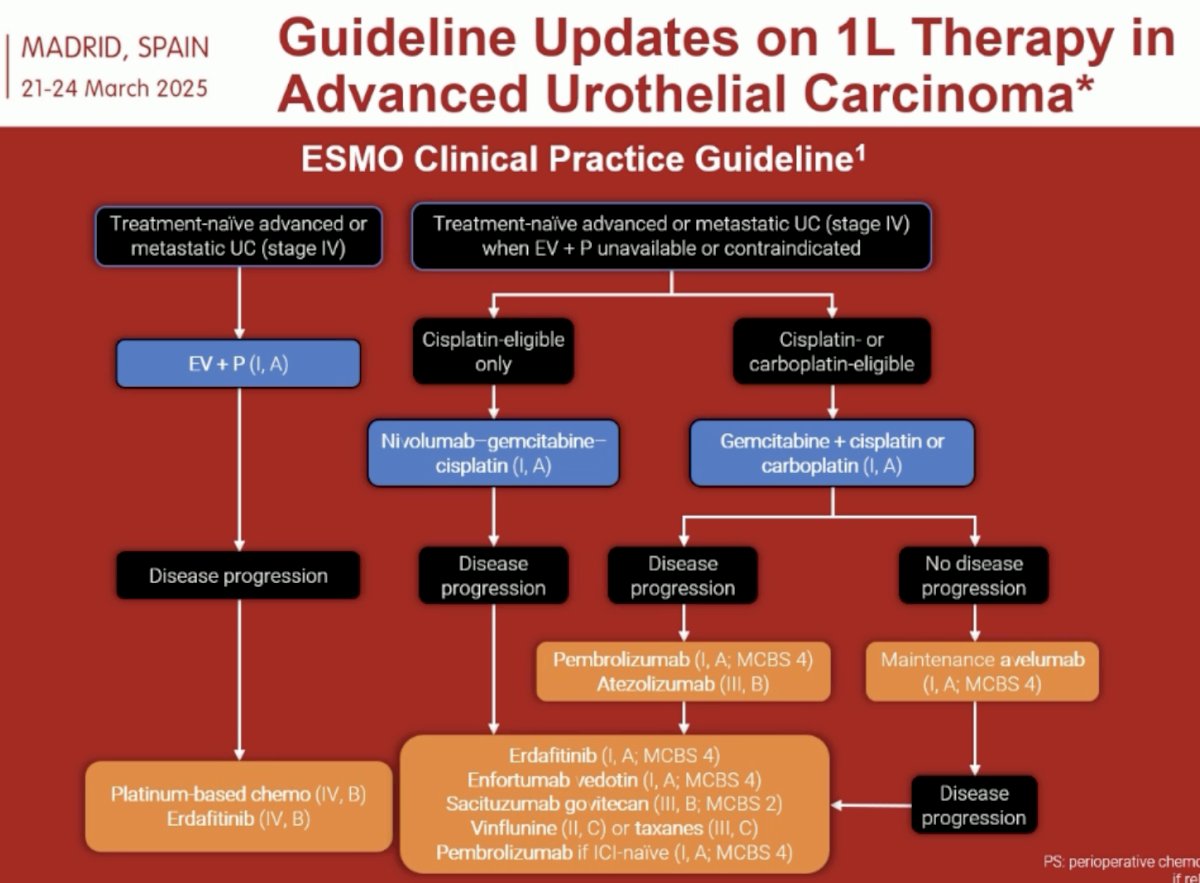
While some may argue that this patient has oligometastatic urothelial carcinoma, and thus should receive metastasis-directed therapy alone, Dr. Necchi argued that we cannot draw exact parallels from the oligometastatic prostate cancer paradigm, given that these patients have a more aggressive underlying biology with worse prognoses. Irrespective of whether these patients present with de novo or recurrent oligometastases following radical cystectomy, they should receive 1st line systemic therapy for metastatic disease, with metastasis-directed therapy reserved for patients who demonstrate a favorable response to systemic therapy.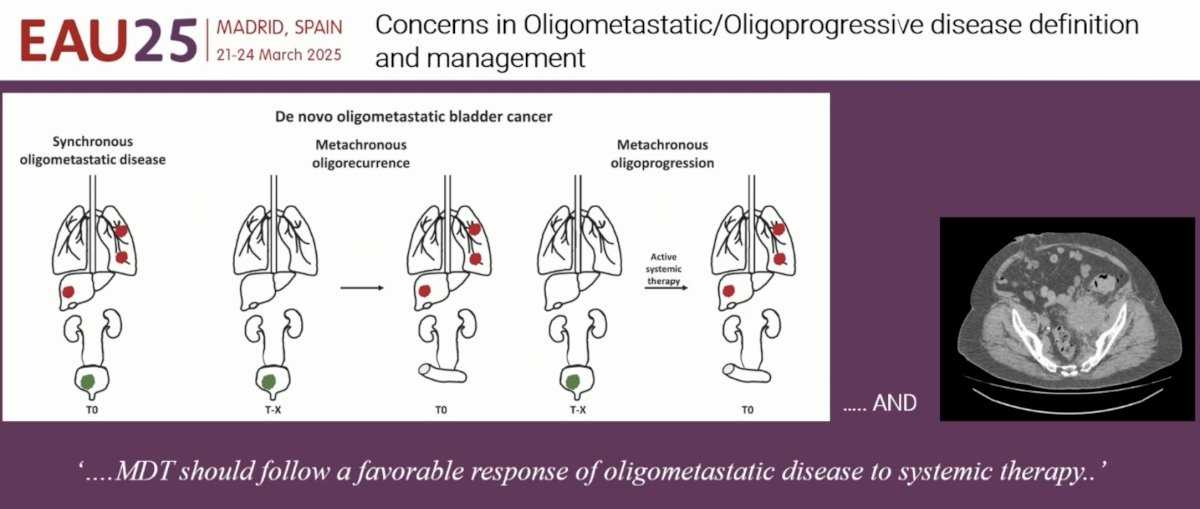
Dr. Necchi noted that these patients with limited metastatic disease, including lymph node-only disease, do well with currently available systemic therapy options. In the CheckMate-901 trial of Gem-Cis +/- nivolumab and EV-302 of enfortumab vedotin + pembrolizumab, patients with lymph node-only disease had excellent objective response rates in the intervention arms of both trials,2,3 as shown below, supporting the use of current 1st line systemic therapy options for these patients.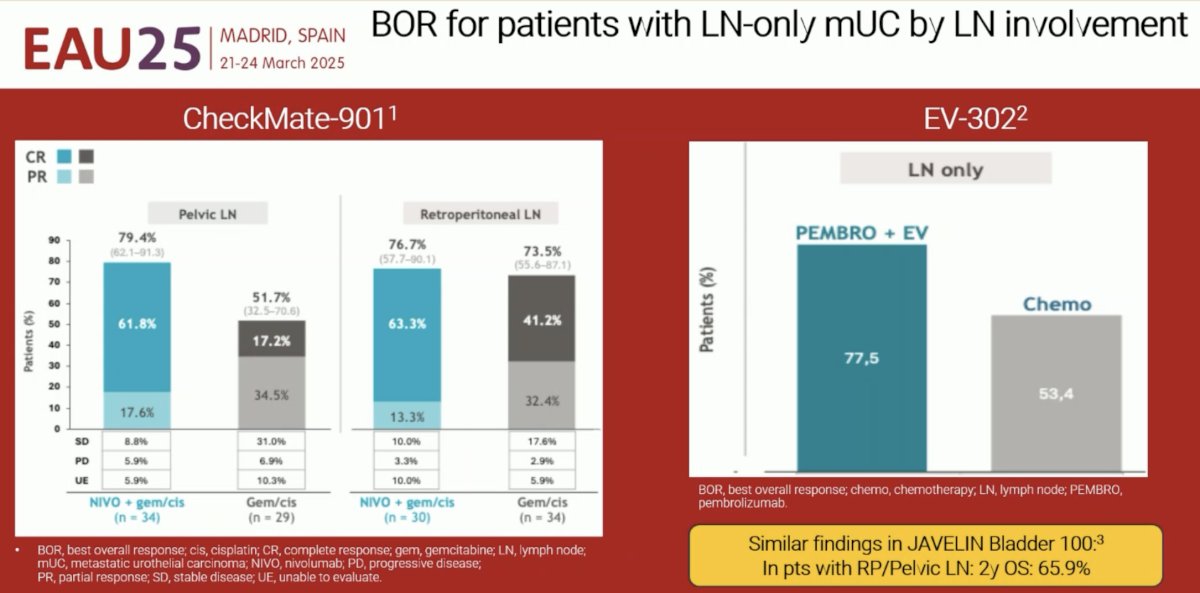
What does the oncology community believe is the best approach for this patient? Dr. Necchi highlighted data from an X (formerly Twitter) poll that suggests that systemic therapy alone is the preferred choice (33.3%), with 30% recommending radiotherapy only if there is a response with systemic therapy 1st.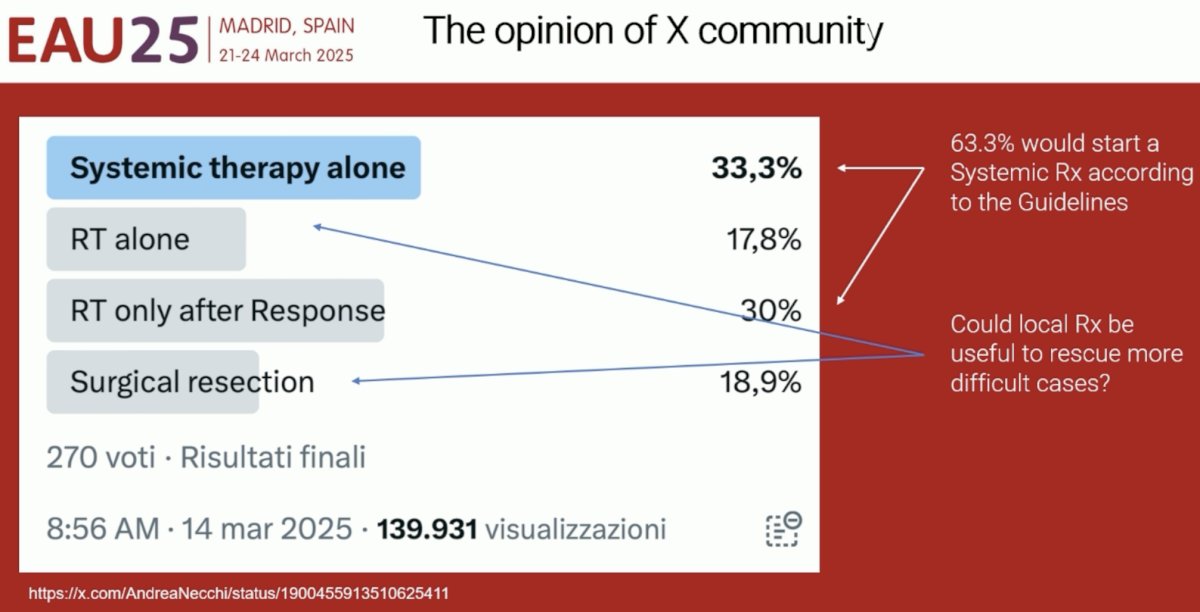
With an eye to the future, Dr. Necchi warned that as systemic therapy options, as outlined in the slide below, become increasingly used in the earlier, including non-muscle invasive, settings, we are going to be ‘exhausting’ options earlier in the treatment paradigm, and these patients with metastatic disease, including pelvic-only disease, are going to have less options available. This may open up the avenue for rescue with local treatment for patients who develop oligorecurrences following effective induction therapy.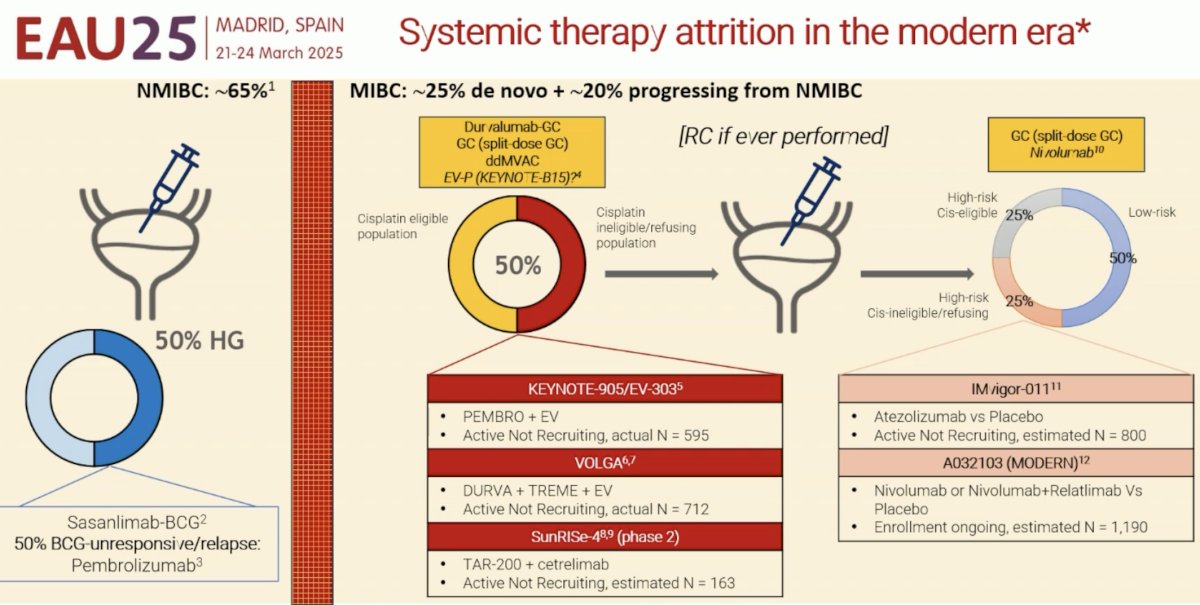
Dr. Necchi concluded as follows:
- MIBC is a systemic disease
- The 5-year overall survival of MIBC is 50% with radical therapy alone
- Therefore, pelvic oligometastatic/recurrent bladder cancer remains largely incurable
- Patients with cT4bN0M0, N1-3, or M1 MIBC should primarily be offered the best systemic therapy option, according to the guidelines, or should be included in clinical trials
- Complete response with newer systemic therapies is endowed with a possibility of cure in select cases
- However, we should acknowledge an opportunity for treatment personalization in select cases. Rescue with local treatment may become a more pressing need as a number of patients will develop oligorecurrences after effective induction therapy.
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 European Association of Urology (EAU) Annual Congress held in Madrid, Spain between March 21st and 24th, 2025
Related content: Radiation vs Systemic Therapy for Isolated Pelvic Recurrence After Cystectomy - Andrea Necchi & Comron Hassanzadeh
- Murthy V, Maitre P, Bakshi G, et al. Bladder Adjuvant Radiation Therapy (BART): Acute and Late Toxicity From a Phase III Multicenter Randomized Controlled Trial. Int J Radiat Oncol Biol Phys. 2025; 121(3): 728-36.
- Van der Heijden MS, Sonpavde G, Powles T, et al. Nivolumab plus Gemcitabine–Cisplatin in Advanced Urothelial Carcinoma. N Engl J Med. 2023; 389: 1778-9.
- Powles T, Valderrama BP, Gupta S, et al. Enfortumab Vedotin and Pembrolizumab in Untreated Advanced Urothelial Cancer. N Engl J Med. 2024; 390: 875-88.