(UroToday.com) The 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain between March 21st and 24th 2025, was host to the Biomarkers to guide peri-operative management in Uro-oncology Plenary Session. Dr. Lars Dyrskjøt delivered the State-of-the-art lecture Biomarker discovery: From bench to bedside.
Dr. Dyrskjøt began his presentation by highlighting that biomarkers are paving the way for precision tools in urologic oncology. They can serve as diagnostic, prognostic, or predictive biomarkers, helping to personalize and optimize perioperative decisions while reducing both overtreatment and undertreatment.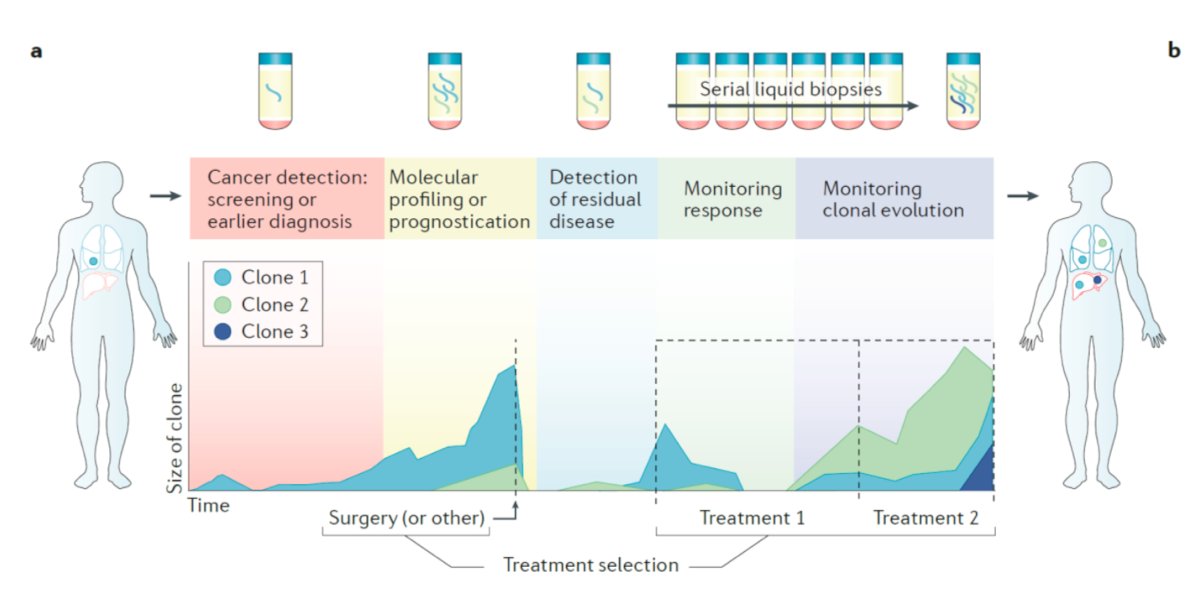
The history of tumor biomarkers dates to 1847, when Henry Bence Jones discovered the Bence-Jones protein (BJP), marking the first identified tumor biomarker. Since then, analytical methods have continued to evolve, with indications and potential applications expanding significantly over the past decades.1,2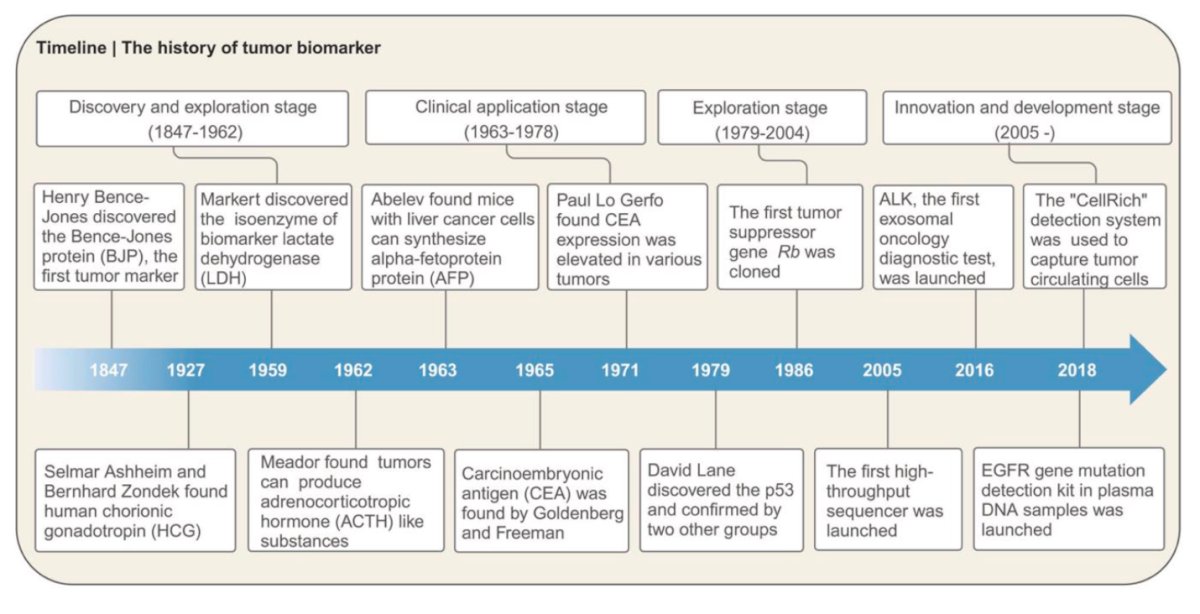
Biomarker discovery and methods.
Novel technologies have significantly advanced the identification of biomarkers. Genomics, transcriptomics, proteomics, and other "omics" approaches are playing a crucial role in discovering and characterizing novel biomarkers. Various cutting-edge technologies, including next-generation sequencing (NGS), artificial intelligence (AI), and specialized analytical techniques, are now available to assess different biological analytes, further refining biomarker discovery and application.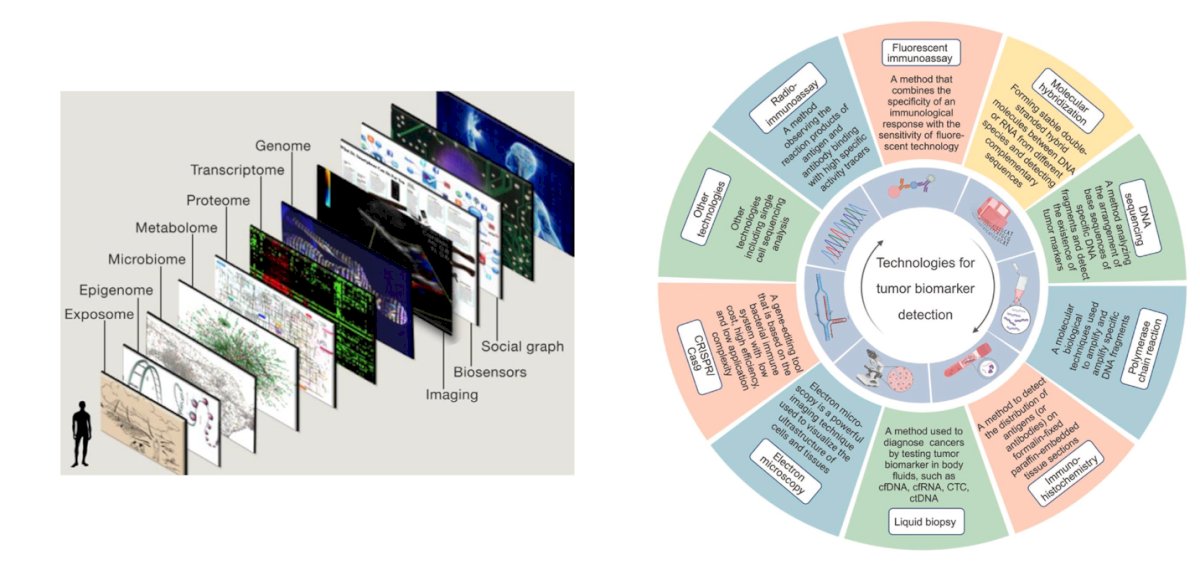
The benchmark process for developing a tumor biomarker progresses through several key stages: discovery, analytical validation, clinical validation, and qualification. These stages occur in different settings, starting in the laboratory, followed by clinical application, and ultimately leading to commercialization, as illustrated below.3 There are different hurdles along the way to discover and validate these biomarkers.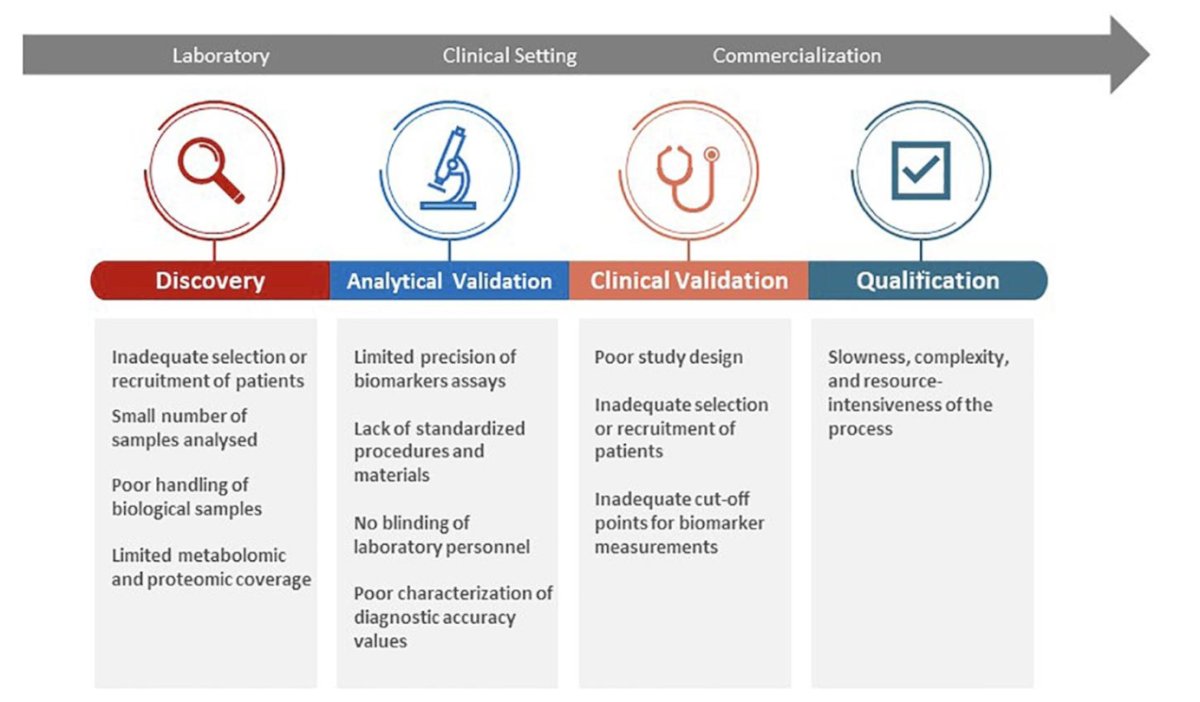
Dr. Dyrskjøt provided a historical overview of the development of circulating tumor DNA (ctDNA). Initially discovered in blood plasma in 1948, its significance in oncology became apparent in 1977 when elevated levels of cell-free DNA were identified in cancer patients. Today, we are launching multiple prospective randomized clinical trials evaluating ctDNA as a biomarker to guide clinical decision-making across various cancer types and disease stages.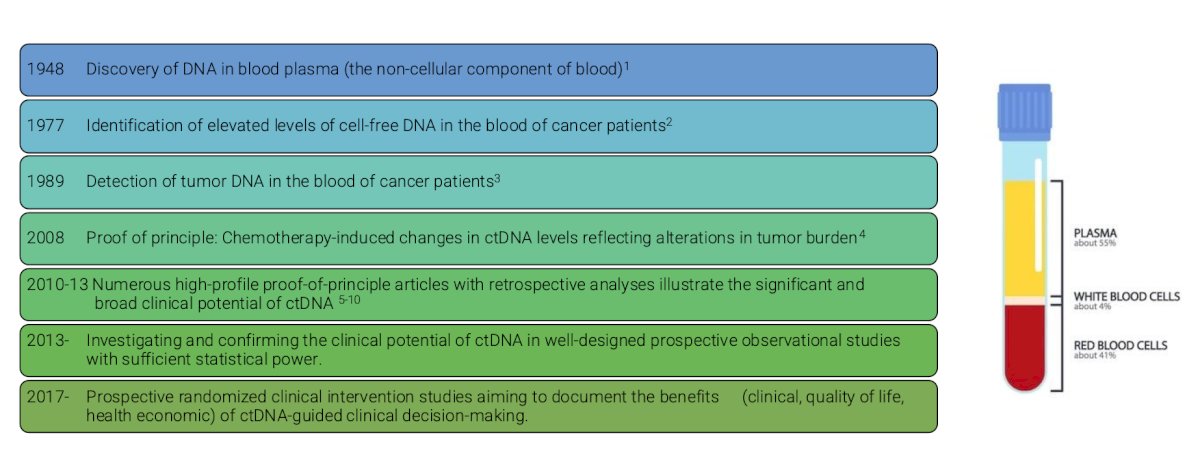
Dr. Dyrskjøt explored the challenges that delay biomarkers from reaching clinical practice. These include biological complexity, such as tumor heterogeneity, small study cohorts, and biomarker stability. Technical limitations, including assay sensitivity, specificity, and lack of standardization, also pose significant barriers. Additionally, clinical validation requires large patient cohorts and long follow-up periods to generate robust evidence. Finally, stringent regulatory requirements further extend the timeline for approval and implementation in clinical settings.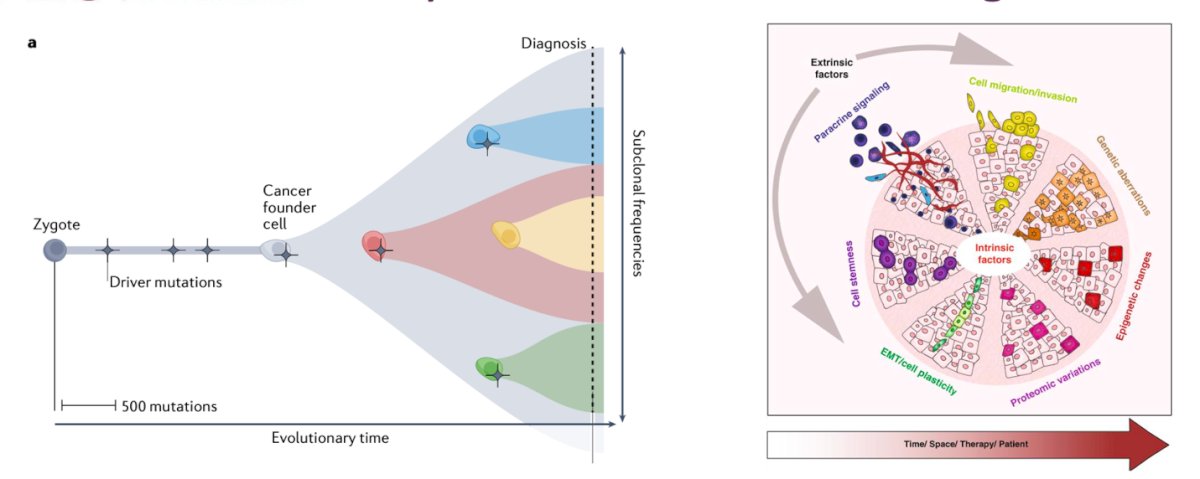
Strategies to accelerate clinical implementation include:
- Collaborative Networks: National and international consortia can be used for standardizing protocols and rapidly generate validation data.
- Public-Private Partnerships: Industry collaboration accelerates assay development, standardization, and also financial risk-sharing in the work.
- Innovative Clinical Trial Designs: Basket trials, umbrella trials, and platform trials help validate biomarkers across multiple cancers.
- Harmonization and Standardization: Global efforts (BLOODPAC, ctMoniTR, GuideMRD) align analytical methods, quality controls, and regulatory pathways.
- Real-World Evidence: Integration into routine care continuously validates biomarkers, speeding adoption.
- Early Regulatory Engagement: Is important to engage in proactive discussions with FDA/EMA help clarify validation requirements and reduce regulatory delays.
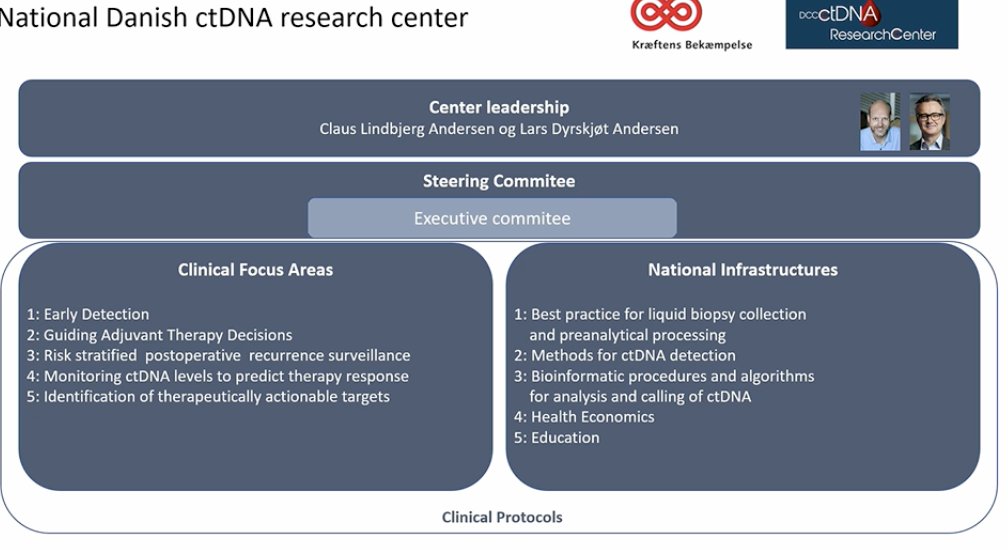
Dr. Dyrskjøt highlighted the National Danish ctDNA Research Center (DCCC). This serves as a model for accelerating the clinical implementation of ctDNA worldwide. They have different clinical focus areas including early detection, guiding adjuvant therapy decisions, and monitoring ctDNA levels. The most important are of these infrastructures is that they are looking at different pipelines to standardize biomarker analysis and avoid people making the same mistakes repeatedly.
The National Danish ctDNA research centre has implemented over 40 national clinical protocols and included more than 3,000 patients across 50+ departments and multiple specialties.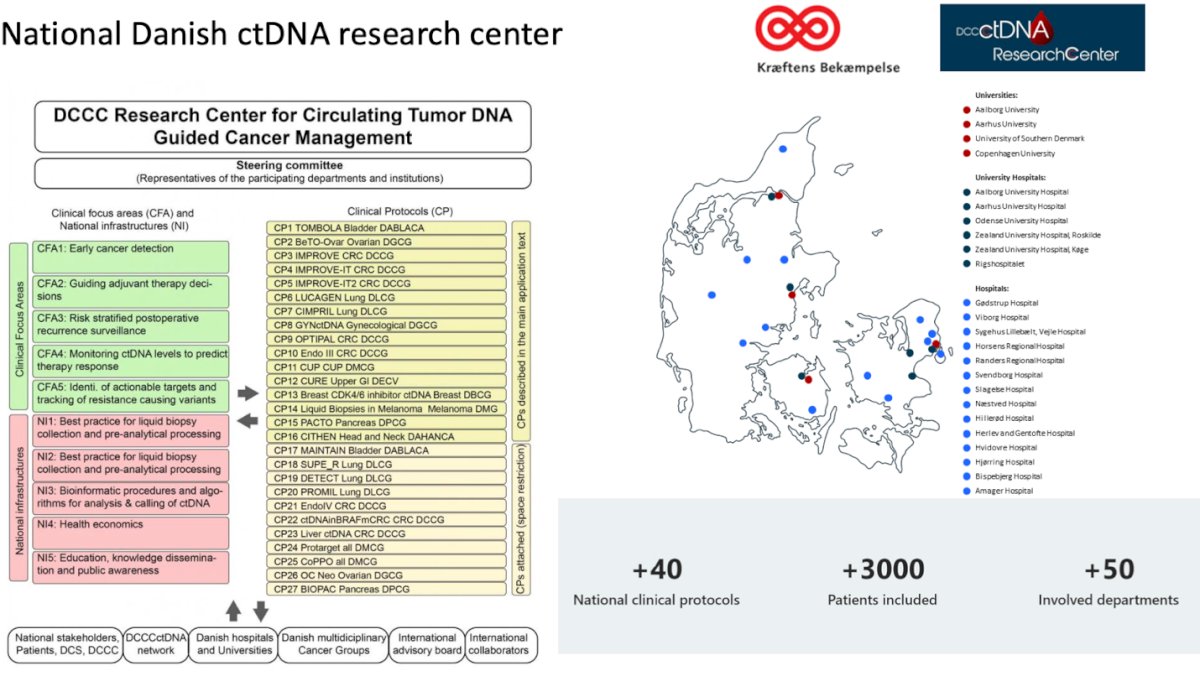
One key study from the DCCC Research Center on ctDNA is the TOMBOLA study in muscle-invasive bladder cancer (MIBC). This real-world, national, non-randomized ctDNA-based intervention study was conducted at five centers in Denmark. Eligible patients had cT2-4aN0-1M0 MIBC, were cisplatin- and immunotherapy-eligible, and underwent neoadjuvant chemotherapy (NAC) followed by radical cystectomy (RC). Patients underwent serial ctDNA testing postoperatively, and those with detectable ctDNA were recommended one year of atezolizumab therapy. The study demonstrated that patients with positive ctDNA post-RC who were under surveillance had significantly shorter survival.4
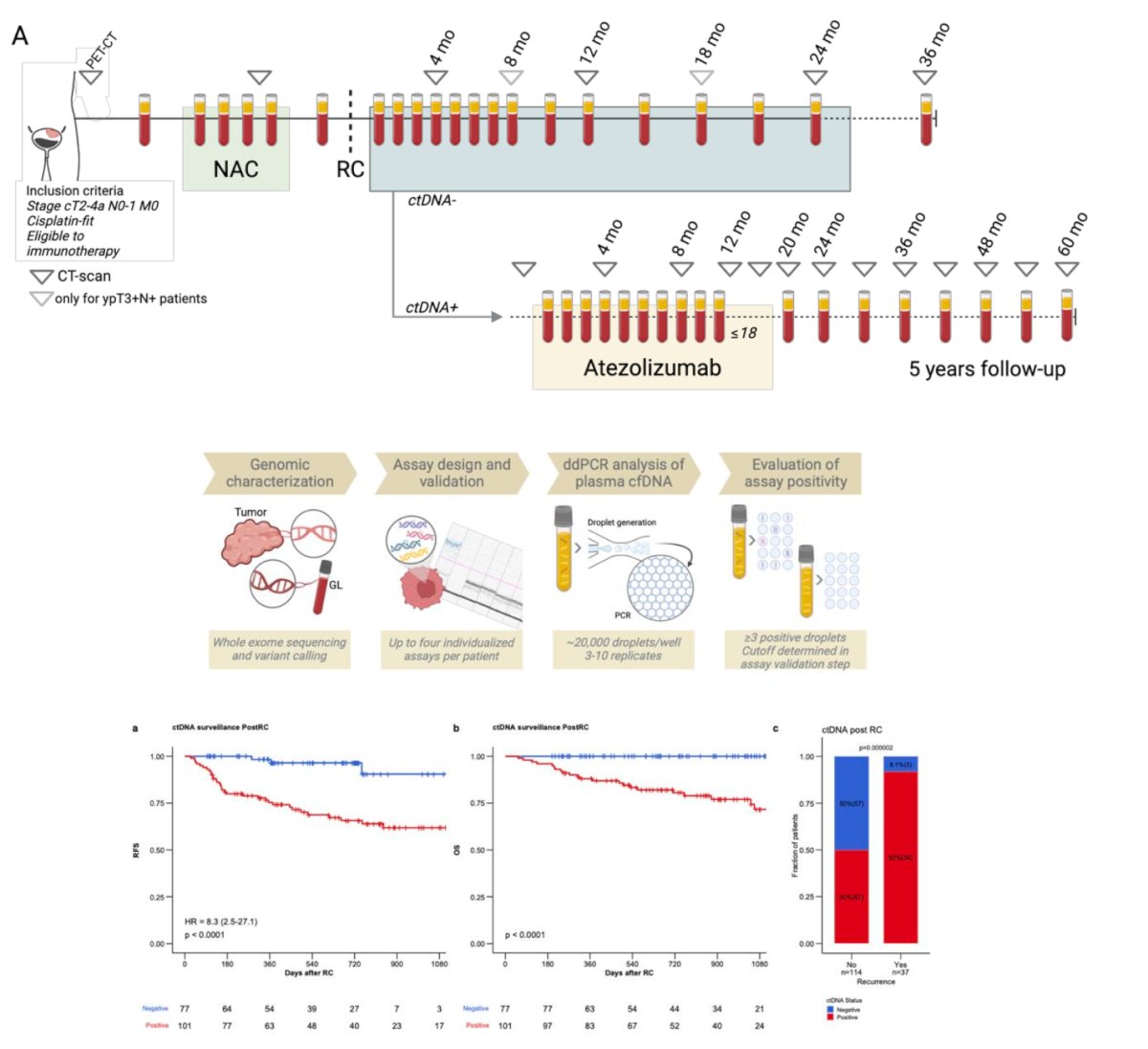
Moreover, this study helped refine analytic methods by comparing tumor fraction measurements. ctDNA was detected using both digital droplet PCR (ddPCR) and whole-genome sequencing, allowing for a comprehensive evaluation of detection techniques.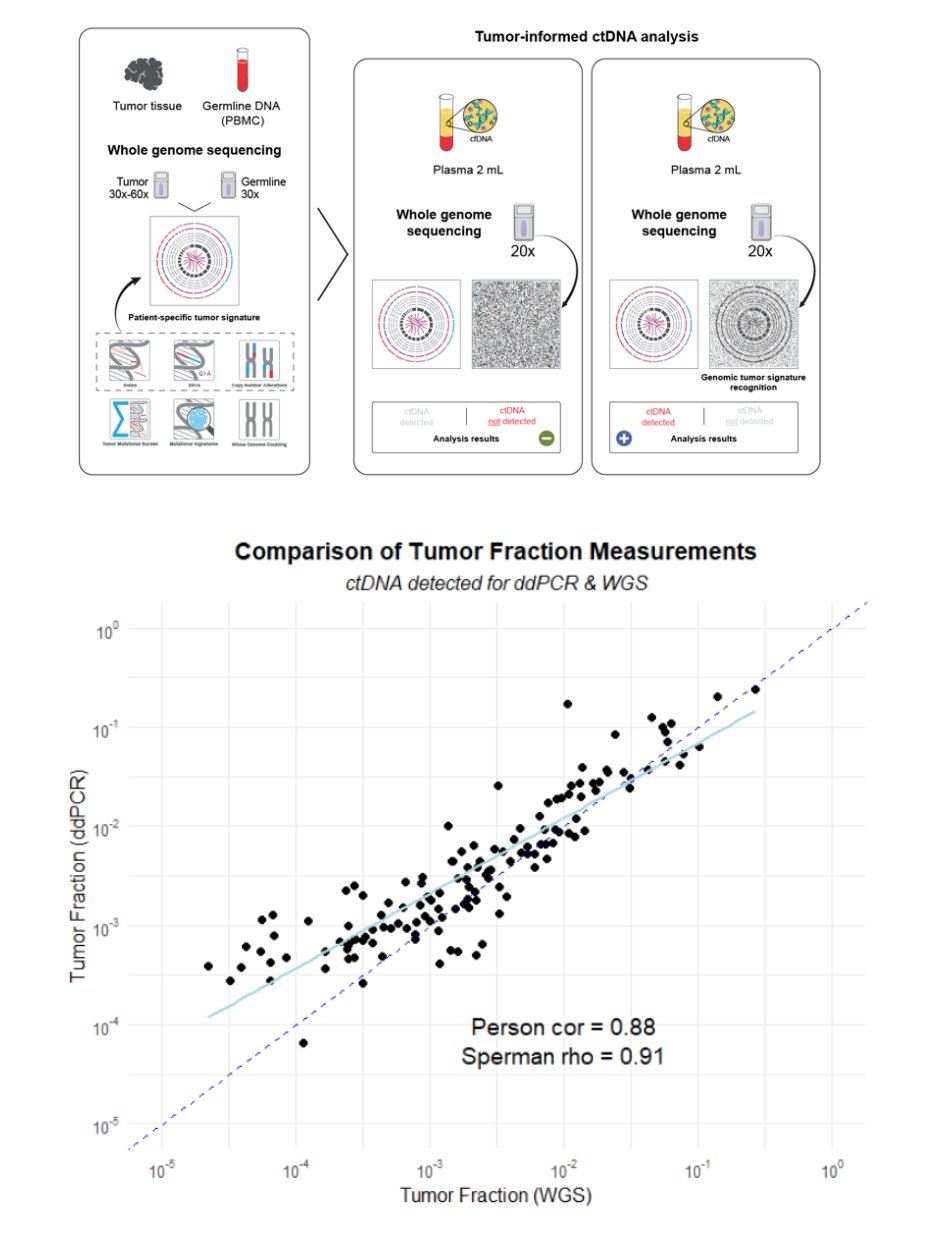
Key lessons learned from biomarker implementation across different therapeutic areas. For PD-L1 in immunotherapy, there needs to be a clear clinical need and this accelerates implementation, early assay standardization is critical, and regulatory guidance from agencies like the FDA and EMA is essential early in development. For BRCA and HR biomarkers used with PARP inhibitors, a strong biological rationale supports adoption, but robust analytical validation and patient education are crucial for acceptance. Finally, in the case of ctDNA for minimal residual disease (MRD) detection and monitoring, standardizing assays improves clinical trust, prospective validation studies are essential, and advances in sensitivity are critical for broad clinical adoption.
Dr. Dyrskjøt concluded his presentation with the following key points:
- Biomarkers are essential tools for improving peri-operative management in urologic oncology.
- Biomarker translation is challenging due to biological complexity, technical issues, clinical validation, and regulatory barriers.
- We need collaboration, this accelerates implementation through national/international networks, public-private partnerships, standardized protocols, and innovative clinical trials.
- Real-world evidence demonstrates clinical impact and feasibility in guiding personalized treatment, these trials are clearly very important.
- Multidisciplinary engagement is crucial for rapid clinical adoption and patient benefit.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain between March 21st and 24th 2025
References:- Topol EJ. Individualized medicine from prewomb to tomb. Cell. 2014 Mar 27;157(1):241-53. doi: 10.1016/j.cell.2014.02.012. PMID: 24679539; PMCID: PMC3995127.
- Landry V, Coburn P, Kost K, Liu X, Li-Jessen NYK. Diagnostic Accuracy of Liquid Biomarkers in Airway Diseases: Toward Point-of-Care Applications. Front Med (Lausanne). 2022 Jun 6;9:855250. doi: 10.3389/fmed.2022.855250. PMID: 35733871; PMCID: PMC9207186.
- Seferbekova Z, Lomakin A, Yates LR, Gerstung M. Spatial biology of cancer evolution. Nat Rev Genet. 2023 May;24(5):295-313. doi: 10.1038/s41576-022-00553-x. Epub 2022 Dec 9. PMID: 36494509.
- Bjerggaard Jensen, J. et al.1960O Identification of bladder cancer patients that could benefit from early post-cystectomy immunotherapy based on serial circulating tumour DNA (ctDNA) testing: Preliminary results from the TOMBOLA trial. Annals of Oncology, Volume 35, S1133