(UroToday.com) The 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain between March 21st and 24th 2025, was host to the Biomarkers to guide peri-operative management in Uro-oncology Plenary Session. Dr. Philippe Spiess delivered a presentation discussing the role of Perioperative Neoadjuvant/Adjuvant Therapy in the Management of Bladder and Kidney Cancer.
Dr. Spiess began his presentation by emphasizing that for many genitourinary malignancies, traditional treatment approaches, such as upfront surgery or conventional systemic chemotherapy for aggressive or locally advanced cancers like bladder and kidney cancer, have been suboptimal. However, the evolution of immunotherapy from metastatic to localized disease through innovative trials, such as PURE-01 in muscle-invasive bladder cancer (MIBC), has demonstrated its potential to redefine the neoadjuvant treatment paradigm.1 In PURE-01, up to 42% of patients achieved a pathological complete response (pT0) after three cycles of pembrolizumab before radical cystectomy.1 The rationale behind this approach is that immunotherapy enhances the host immune response, helping to consolidate the localized treatment effect, improve regional control of micrometastatic disease, and often achieve favorable toxicity profiles with predictable safety.2
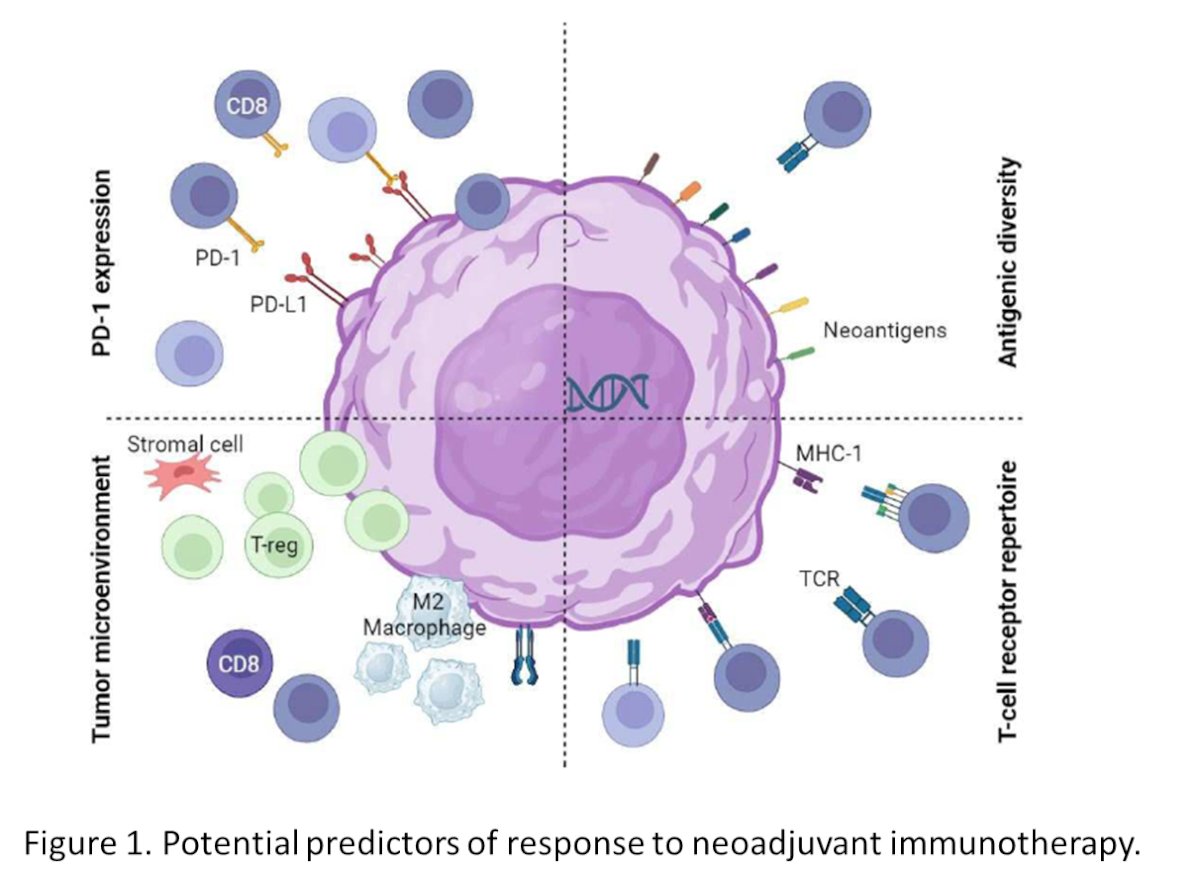
Perioperative immunotherapy in Bladder cancerNotably, potential predictors of response to neoadjuvant immunotherapy include PD-1 or PD-L1 expression, which may influence sensitivity to treatment. The tumor microenvironment whether this is an immune hot or cold also plays a role, with CD8⁺ T-infiltrating lymphocytes associated with sensitivity and regulatory T cells linked to resistance. Additionally, antigenic diversity—such as high tumor mutation burden or microsatellite instability—may enhance immunotherapy sensitivity. The diversity of the T-cell receptor repertoire could further improve treatment efficacy, as illustrated in the figure below.3
The European Association of Urology (EAU) 2024 Guidelines on Muscle-Invasive and Metastatic Bladder Cancer recommend offering neoadjuvant immunotherapy only within a clinical trial setting. Additionally, adjuvant nivolumab is recommended for selected patients with pT3/4 and/or pN+ disease who are either ineligible for or have declined adjuvant cisplatin-based chemotherapy but the strength of the recommendation is weak. In 2025 the guidelines remain the same.4
Dr. Spiess went on to discuss the AMBASSADOR trial led by Andrea Apolo, as illustrated in the study schema below. Patients with muscle-invasive bladder cancer (MIBC) or upper tract urothelial carcinoma (UTUC) who underwent cystectomy or nephroureterectomy were randomized to receive pembrolizumab 200 mg every three weeks for one year or observation. Notably, pembrolizumab demonstrated a significant benefit in reducing disease progression or death (HR 0.73, 95% CI 0.59–0.90).5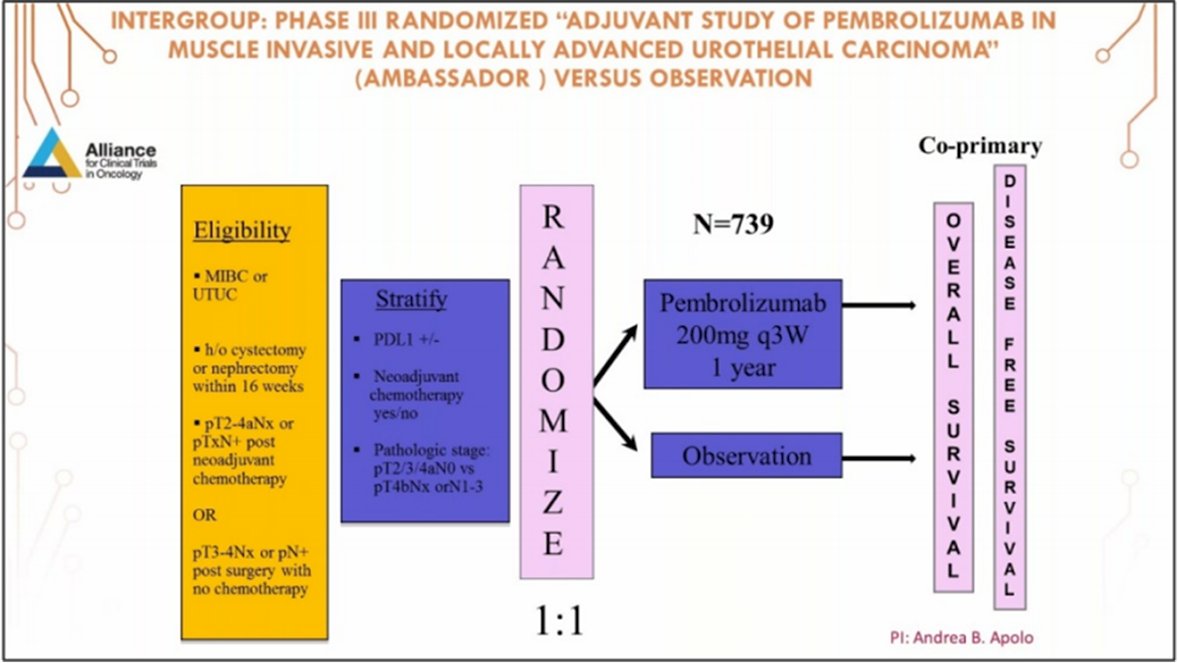
Moreover, the NIAGARA study was the first phase 3 trial testing perioperative immune checkpoint inhibitor (Durvalumab) combined with NAC (Gemcitabine + cisplatin alone) in cisplatin-eligible patients with MIBC (cT2-TaN0/1M0). The study design is illustrated below.

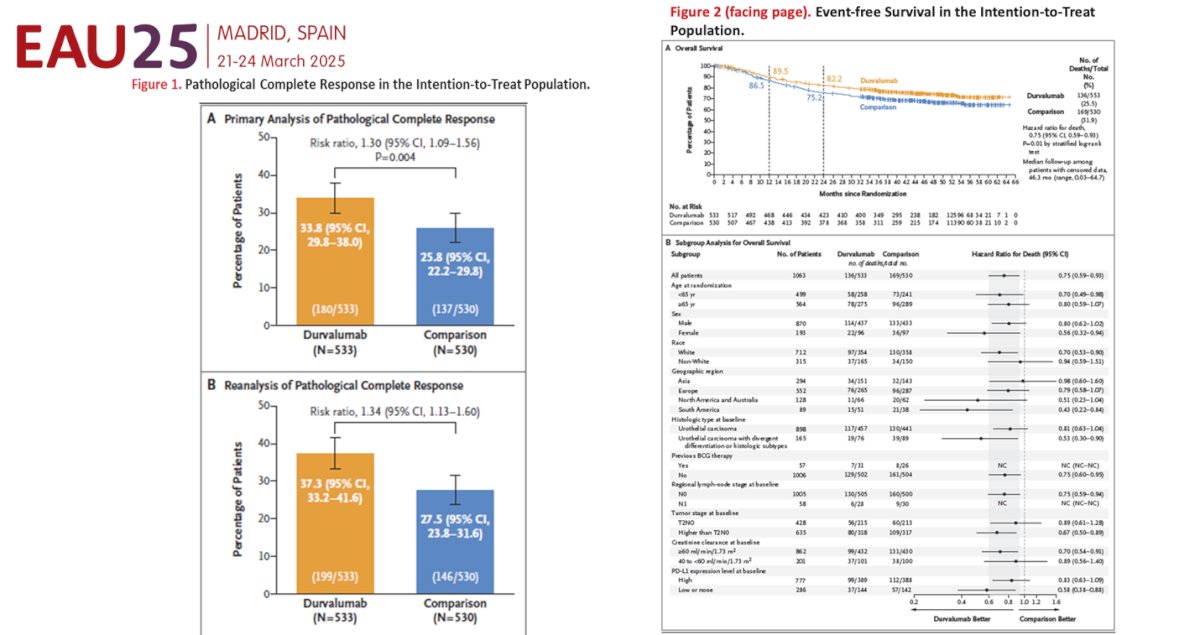
The event-free survival at 2 years was 67.8% in the Durvalumab arm compared to 59.8% in the comparator arm. The hazard ratio (HR) for EFS was 0.68 (95% CI: 0.56–0.82, p<0.0001). Moreover, the pCR was reported in two separate analyses: a formal analysis in January 2022 and a re-analysis in April 2024. The planned formal analysis for pCR was not statistically significant (p=0.0038) as the threshold for significance was a p-value of 0.001. However, this analysis incorrectly classified 59 evaluable samples as non-responders rather than their true result. The re-analysis, which included these 59 samples and identified 28 additional pCRs, showed statistical significance in favor of the Durvalumab arm (p=0.0005).6 The Forest plot shows improvement in all subsets of patients.
Dr. Spiess summarized neoadjuvant immunotherapy (IO) and IO + IO combinations for MIBC, highlighting that pathological complete response (pCR, pT0N0) is as high as 46%, as shown below. He posed the question: among these trials, is there an interim signal of clinical activity? He believes there is. However, when considering whether these results are sufficient to envision a bladder-sparing opportunity, his conclusion was that it is not yet feasible—at least in unselected patients.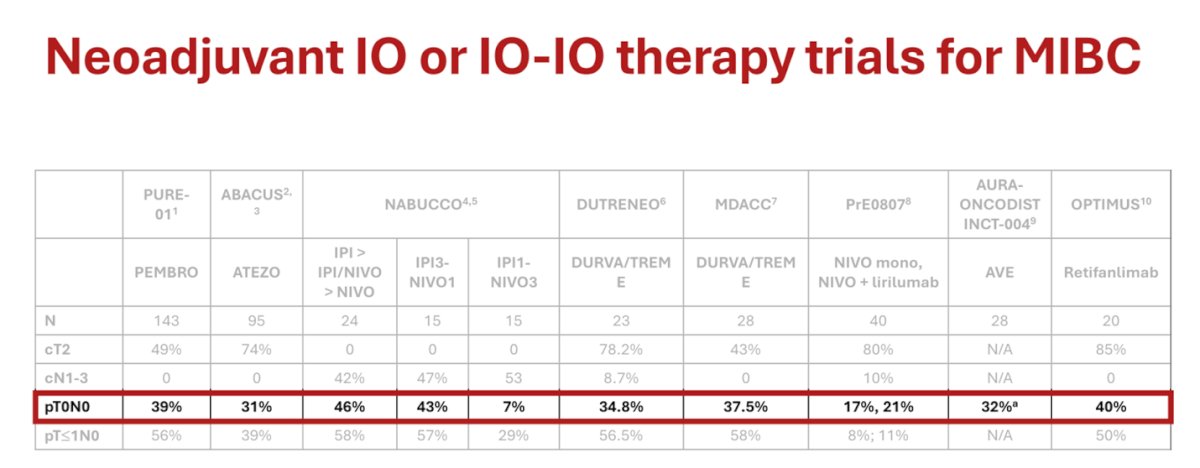
Moreover, when comparing neoadjuvant IO + chemotherapy trials for MIBC, there does not appear to be an interim signal of additive or synergistic effect, at least with cisplatin-based chemotherapy, as pCR rates remain similar across these trials, as shown below.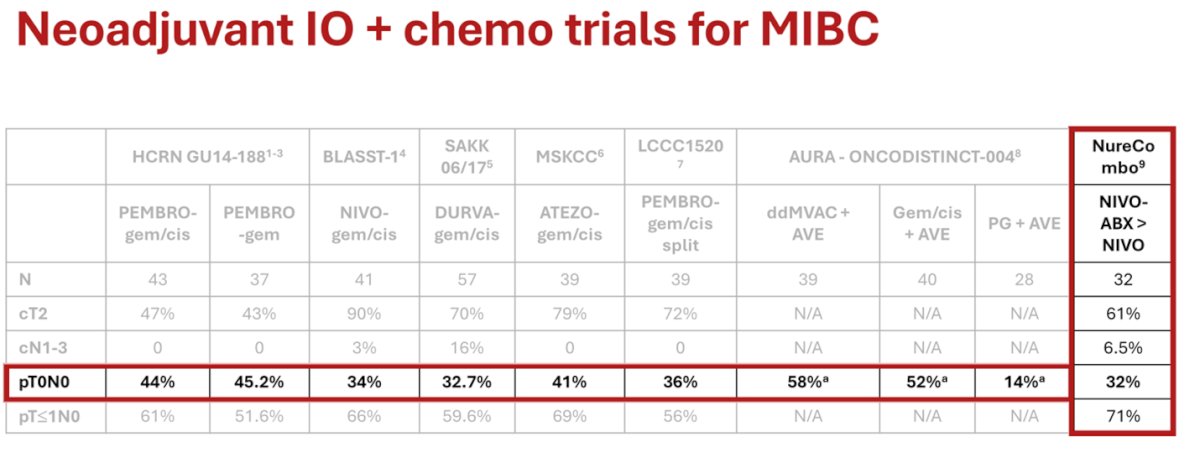
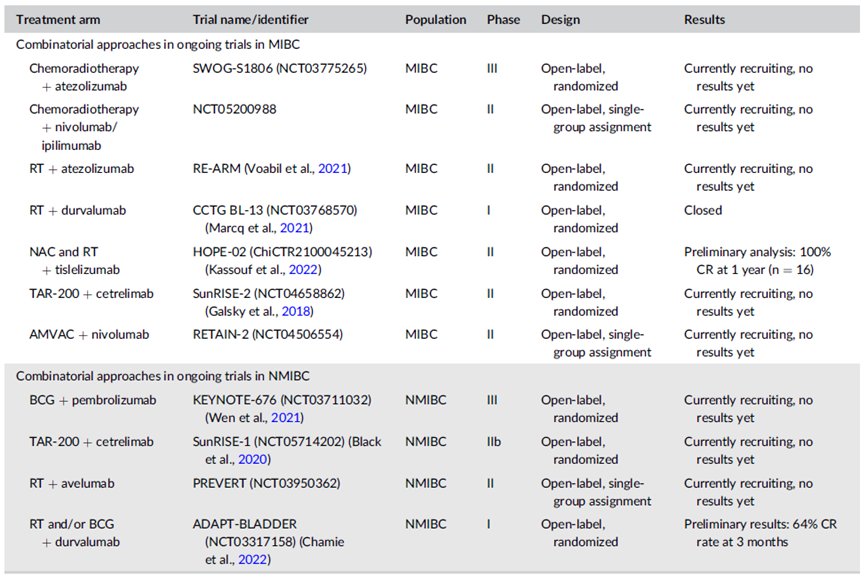
Dr. Spiess highlighted multiple trials evaluating the integration of novel immunotherapeutic approaches in combination with other organ-sparing therapies for both MIBC and NMIBC.
Notably, the LCCC1520 (NCT02690558) phase 2 single-arm trial evaluated neoadjuvant chemoimmunotherapy (gemcitabine and cisplatin plus pembrolizumab; NAC-ICI) for MIBC. Treatment was associated with changes in the tumor mutational profile, immune gene signatures, and RNA subtype switching. Clinical response correlated with an increase in plasma IL-9 from pre-treatment to the initiation of cycle 2, while higher pre-treatment tumor PD-L1 and TIGIT RNA expression were linked to complete response. Additionally, the IL-8 signature, and stroma-rich subtype were associated with improved response. These findings further strengthen the evidence that immune features play a key role in response to neoadjuvant chemoimmunotherapy for MIBC.7
Lastly, Dr. Spiess highlighted that the future of MIBC treatment lies in individualization and improved patient selection. He discussed a study utilizing minimal residual disease (MRD)-based clinical decision-making in patients undergoing neoadjuvant therapy and MRD testing. Based on MRD status and urinary tumor DNA (utDNA) response, patients may proceed with continued neoadjuvant therapy, surveillance, radical cystectomy, or personalized therapy guided by actionable biomarkers.
There are two roles, one in the neoadjuvant setting and the other one in the adjuvant setting. The goals of neoadjuvant therapy include tumor shrinkage to reduce surgical morbidity and extent, as well as to address other underlying conditions. Similarly, the goal of adjuvant therapy is to reduce the likelihood of recurrence or cancer progression after resection, whether in the setting of locally advanced disease or following metastasectomy.
Dr. Spiess highlighted four key trials in the perioperative setting for renal cell carcinoma (RCC): three in the adjuvant setting: KEYNOTE-564, CHECKMATE-914, and IMmotion010, and one in the perioperative setting: PROSPER (ECOG-ACRIN EA8143). The study design of each trial is detailed below.

Notably, the only positive trial was KEYNOTE-564, which evaluated adjuvant pembrolizumab for up to 17 cycles. This trial demonstrated a significant overall survival benefit for pembrolizumab vs. placebo and has changed the treatment paradigm for these patients.8 This led to the FDA and EMA approval of pembrolizumab for the adjuvant treatment of patients with RCC at intermediate-high or high risk of recurrence following nephrectomy or following nephrectomy and resection of metastatic lesions (NED).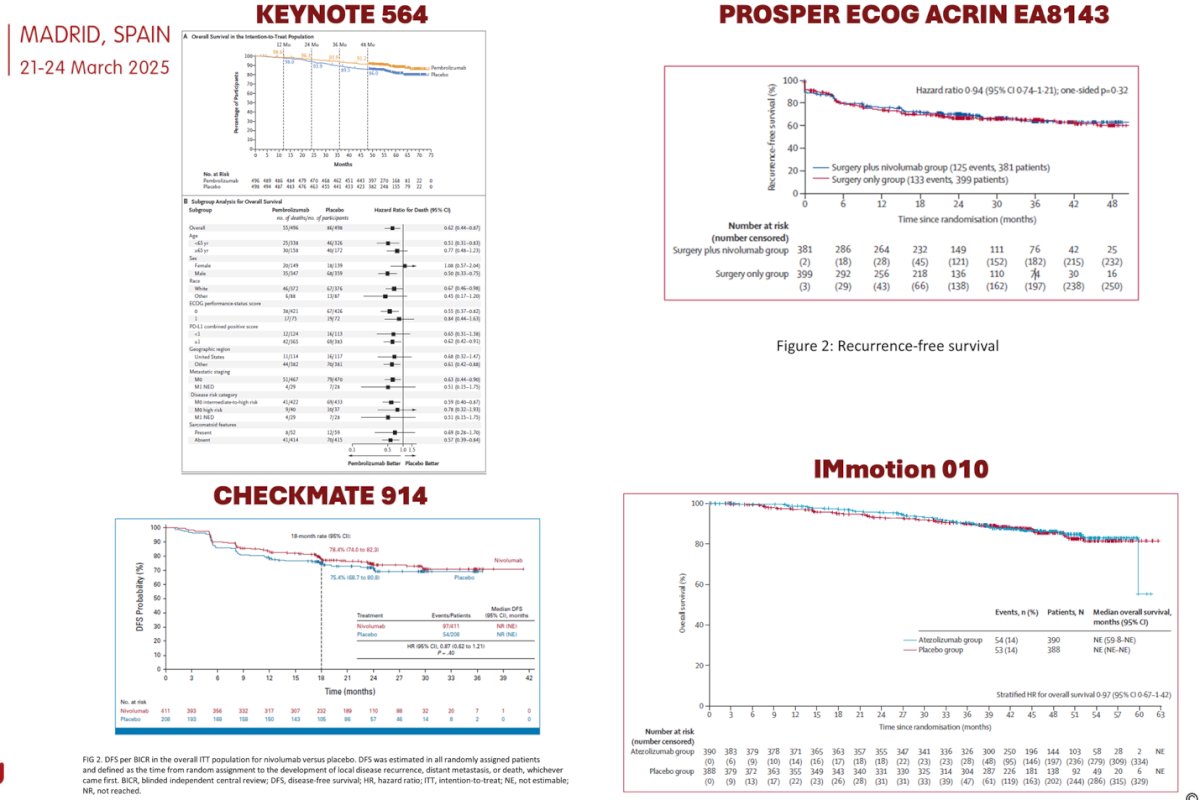
Based on this data, the EAU has updated its guidelines and now, albeit with a weak strength rating, recommends offering adjuvant pembrolizumab to patients with ccRCC at high risk of recurrence, as defined in the KEYNOTE-564 trial.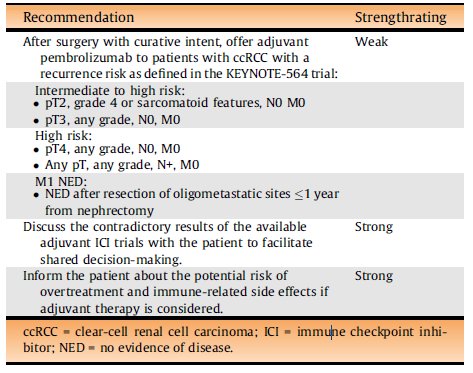
The future of perioperative treatment in RCC includes improved patient selection through AI-powered decision support engines and radiomics. Considering we have three negative and only one positive trial in adjuvant therapy for ccRCC. AI-driven models can help tailor treatment plans, improving efficacy and quality of life. In a study of 267 patients with ccRCC, including 26 who received targeted therapy, an AI model demonstrated high accuracy in predicting survival outcomes (93.66% in Group 1 and 94.14% in Group 2). Similarly, a systematic review of 27 studies (6,119 patients) assessed the clinical application of radiomics for predicting treatment outcomes and survival, with most studies using contrast-enhanced abdominal CT and reporting at least modest accuracy (AUC range: 0.55–0.99).
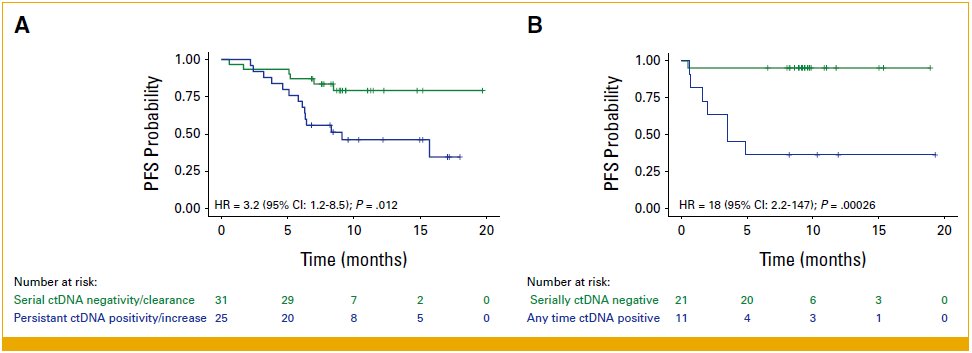
Circulating tumor DNA (ctDNA) may also play a role in RCC treatment monitoring. A multicenter retrospective analysis (n=92) using commercial ctDNA testing (Signatera) in metastatic RCC showed that serial ctDNA negativity or clearance correlated with improved progression-free survival (PFS) compared to patients who remained or became ctDNA positive during therapy, suggesting its potential as a biomarker for treatment response.9 Tailoring our treatment approach is clearly needed.
Neoadjuvant therapy may be particularly beneficial in RCC with tumor thrombus. A systematic review and meta-analysis of 29 single-arm studies and 5 cohort studies, including 204 patients, found that neoadjuvant therapy led to a thrombus level reduction in 29.4% of cases. Patients treated with neoadjuvant therapy experienced shorter operative times and reduced blood loss (p<0.05 for both).10 But this is something we should not be doing in most of our patient population.
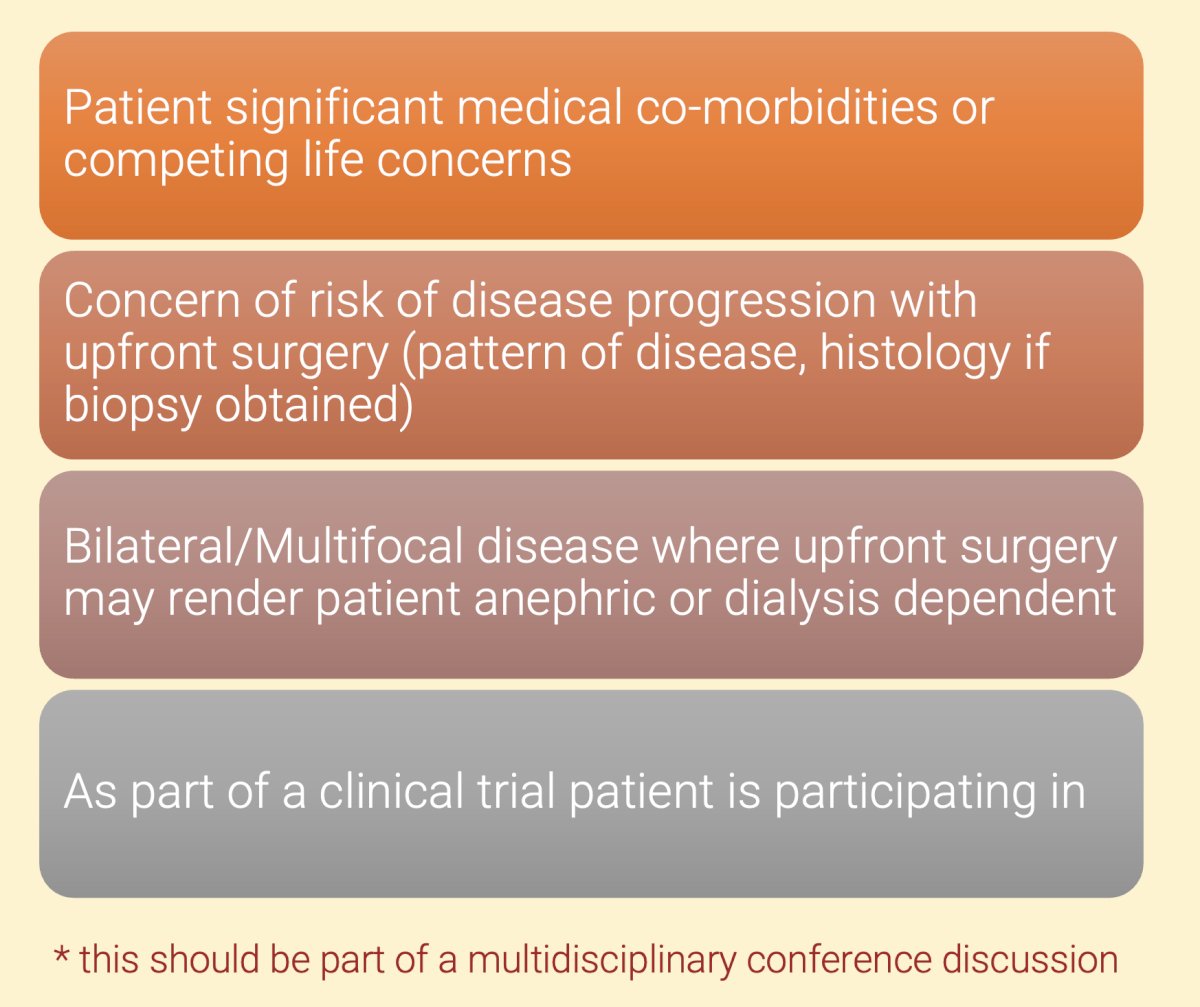
Scenarios where neoadjuvant immunotherapy (IO) may be a worthy consideration are outlined below. Importantly, all such cases should be discussed in a multidisciplinary cancer conference to ensure optimal patient selection and treatment planning.
Dr. Spiess concluded his presentation with the following key takeaways:
- The integration of immunotherapy in the management of bladder and kidney cancer, both in the neoadjuvant and adjuvant settings, is rapidly expanding, with novel agents—alone or in combination—offering new possibilities in clinical care.
- In terms of MIBC, the significant response rates to neoadjuvant IO agents raise the question of if and when consolidative surgery may be necessary for a subset of patients. Ongoing research is focused on better defining complete response (CR) to these agents.
- For locally advanced RCC, adjuvant Pembrolizumab, most notably pembrolizumab, are redefining how we treat these patients. Discrepancies among trials in this space highlight the need for optimal biomarkers of treatment response, including AI, radiomics, and tissue or urinary signatures.
Presented by: Philippe Spiess, BS, MS, MD, FRCS, FACS, Urologic Oncologist and Assistant Chief of Surgical Services at the Moffitt Cancer Center. Tampa, FL
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain between March 21st and 24th 2025
References:- Necchi A, Anichini A, Raggi D, Briganti A, Massa S, Lucianò R, Colecchia M, Giannatempo P, Mortarini R, Bianchi M, Farè E, Monopoli F, Colombo R, Gallina A, Salonia A, Messina A, Ali SM, Madison R, Ross JS, Chung JH, Salvioni R, Mariani L, Montorsi F. Pembrolizumab as Neoadjuvant Therapy Before Radical Cystectomy in Patients With Muscle-Invasive Urothelial Bladder Carcinoma (PURE-01): An Open-Label, Single-Arm, Phase II Study. J Clin Oncol. 2018 Dec 1;36(34):3353-3360. doi: 10.1200/JCO.18.01148. Epub 2018 Oct 20. PMID: 30343614.
- Necchi A, Faltas BM, Slovin SF, Meeks JJ, Pal SK, Schwartz LH, Huang RSP, Li R, Manley B, Chahoud J, Ross JS, Spiess PE. Immunotherapy in the Treatment of Localized Genitourinary Cancers. JAMA Oncol. 2023 Oct 1;9(10):1447-1454. doi: 10.1001/jamaoncol.2023.2174. PMID: 37561425; PMCID: PMC11429659.
- Boydell E, Sandoval JL, Michielin O, Obeid M, Addeo A, Friedlaender A. Neoadjuvant Immunotherapy: A Promising New Standard of Care. Int J Mol Sci. 2023 Jul 24;24(14):11849. doi: 10.3390/ijms241411849. PMID: 37511609; PMCID: PMC10380420.
- Alfred Witjes J, Bruins HM, Carrión A, Cathomas R, Compérat E, Efstathiou JA, Fietkau R, Gakis G, Lorch A, Martini A, Mertens LS, Meijer RP, Milowsky MI, Neuzillet Y, Panebiaco V, Redlef J, Rink M, Rouanne M, Thalmann GN, Sæbjørnsen S, Veskimäe E, Mariappan P, van der Heijden AG. Corrigendum to "European Association of Urology Guidelines on Muscle-invasive and Metastatic Bladder Cancer: Summary of the 2023 Guidelines" [Eur. Urol. 85 (2024) 17-31]. Eur Urol. 2024 Jun;85(6):e180. doi: 10.1016/j.eururo.2024.03.002. Epub 2024 Mar 15. Erratum for: Eur Urol. 2024 Jan;85(1):17-31. doi: 10.1016/j.eururo.2023.08.016. PMID: 38492977.
- Apolo AB, Ballman KV, Sonpavde G, Berg S, Kim WY, Parikh R, Teo MY, Sweis RF, Geynisman DM, Grivas P, Chatta G, Reichert ZR, Kim JW, Bilen MA, McGregor B, Singh P, Tripathi A, Cole S, Simon N, Niglio S, Ley L, Cordes L, Srinivas S, Huang J, Odegaard M, Watt C, Petrylak D, Hoffman-Censits J, Wen Y, Hahn O, Mitchell C, Tan A, Streicher H, Sharon E, Moon H, Woods M, Halabi S, Perez Burbano G, Morris MJ, Rosenberg JE. Adjuvant Pembrolizumab versus Observation in Muscle-Invasive Urothelial Carcinoma. N Engl J Med. 2025 Jan 2;392(1):45-55. doi: 10.1056/NEJMoa2401726. Epub 2024 Sep 15. PMID: 39282902; PMCID: PMC11698643.
- Powles T, Catto JWF, Galsky MD, Al-Ahmadie H, Meeks JJ, Nishiyama H, Vu TQ, Antonuzzo L, Wiechno P, Atduev V, Kann AG, Kim TH, Suárez C, Chang CH, Roghmann F, Özgüroğlu M, Eigl BJ, Oliveira N, Buchler T, Gadot M, Zakharia Y, Armstrong J, Gupta A, Hois S, van der Heijden MS; NIAGARA Investigators. Perioperative Durvalumab with Neoadjuvant Chemotherapy in Operable Bladder Cancer. N Engl J Med. 2024 Nov 14;391(19):1773-1786. doi: 10.1056/NEJMoa2408154. Epub 2024 Sep 15. PMID: 39282910.
- Beckabir W, Zhou M, Lee JS, Vensko SP, Woodcock MG, Wang HH, Wobker SE, Atassi G, Wilkinson AD, Fowler K, Flick LM, Damrauer JS, Harrison MR, McKinnon KP, Rose TL, Milowsky MI, Serody JS, Kim WY, Vincent BG. Immune features are associated with response to neoadjuvant chemo-immunotherapy for muscle-invasive bladder cancer. Nat Commun. 2024 May 24;15(1):4448. doi: 10.1038/s41467-024-48480-1. PMID: 38789460; PMCID: PMC11126571.
- Choueiri TK, Tomczak P, Park SH, Venugopal B, Ferguson T, Symeonides SN, Hajek J, Chang YH, Lee JL, Sarwar N, Haas NB, Gurney H, Sawrycki P, Mahave M, Gross-Goupil M, Zhang T, Burke JM, Doshi G, Melichar B, Kopyltsov E, Alva A, Oudard S, Topart D, Hammers H, Kitamura H, McDermott DF, Silva A, Winquist E, Cornell J, Elfiky A, Burgents JE, Perini RF, Powles T; KEYNOTE-564 Investigators. Overall Survival with Adjuvant Pembrolizumab in Renal-Cell Carcinoma. N Engl J Med. 2024 Apr 18;390(15):1359-1371. doi: 10.1056/NEJMoa2312695. PMID: 38631003.
- Basu A, Au C, Kommalapati A, Kandala H, Sudhaman S, Mahmood T, Carson C, Pajak N, Dutta P, Calhoun M, Malhotra M, ElNaggar AC, Liu MC, Ferguson Iii J, Peyton C, Rais-Bahrami S, Tan A. Longitudinal Testing of Circulating Tumor DNA in Patients With Metastatic Renal Cell Carcinoma. JCO Precis Oncol. 2024 Dec;8:e2400667. doi: 10.1200/PO-24-00667. Epub 2024 Dec 18. PMID: 39693589; PMCID: PMC11670910.
- Gu L, Peng C, Li H, Jia T, Chen X, Wang H, Du S, Tang L, Liang Q, Wang B, Ma X, Zhang X. Neoadjuvant therapy in renal cell carcinoma with tumor thrombus: A systematic review and meta-analysis. Crit Rev Oncol Hematol. 2024 Apr;196:104316. doi: 10.1016/j.critrevonc.2024.104316. Epub 2024 Mar 2. PMID: 38432444.