(UroToday.com) The 2025 European Association of Urology (EAU) Annual Congress held in Madrid, Spain between March 21st and 24th 2025, was host to plenary session on organ-sparing paradigms in kidney and bladder cancer. Drs. Sima Porten, Ananya Choudhury, and Paolo Gontero debated the need for additional therapy for a muscle-invasive bladder cancer patient who had evidence of a complete clinical response on repeat TURBT and MRI imaging following neoadjuvant chemotherapy alone.
Dr. Francesco Del Giudice began the session with a case presentation of a sexually active 67-year-old male with an excellent performance status who presented with gross hematuria and was found on cystoscopy to have widespread, multiple sessile-appearing lesions that were classified as VI-RADS 4 on mp-MRI (i.e., muscle invasion is likely to be present).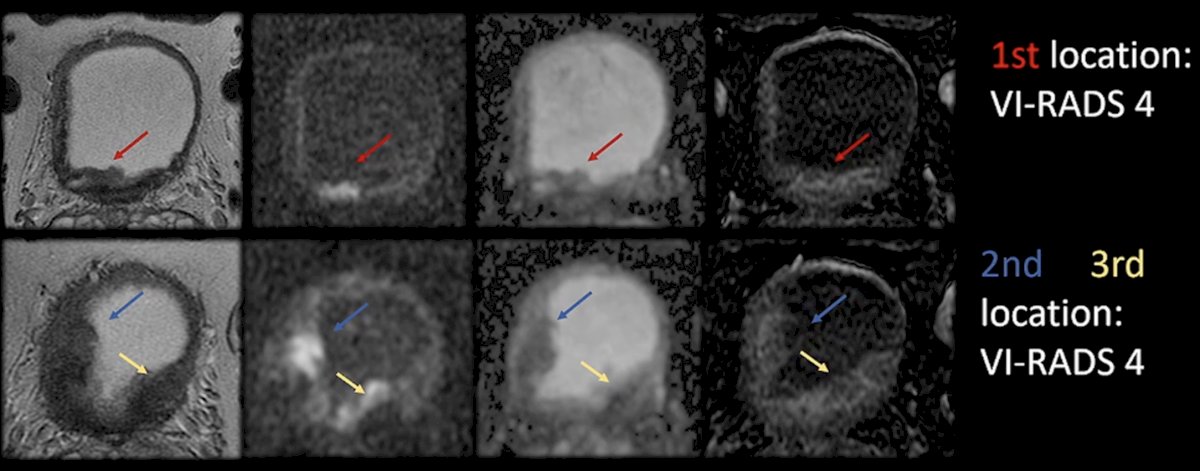
The patient underwent a TURBT with findings of:
- Multifocal, high-grade pure urothelial carcinoma with infiltrative invasion of the lamina propria and focal involvement of the muscularis propria
- Lymphovascular invasion was present
- No CIS on this TURBT sample
He underwent an FDG PET with no evidence of nodal involvement or metastatic disease. His case was discussed at the multi-disciplinary tumor board and was recommended for neoadjuvant chemotherapy with 6 cycles of gem/cis followed by a robotic radical cystectomy and an intracorporeal ileal conduit.
Given his multifocal disease, he was not considered an ideal trimodality therapy (TMT) candidate. However, despite this, the patient expressed a strong preference for TMT with maximal re-TUR, chemotherapy, plus radiotherapy.
He underwent a repeat TURBT in March 2024 with findings of persistent HG T1 disease, with CIS now present. He subsequently received 3 cycles of neoadjuvant gem/cis with good tolerance and no clinically relevant adverse events. An mp-MRI performed 3 months later in June 2024 demonstrated residual tumor in the right lateral and posterior walls with persistent muscle invasion (nacVI-RADS 3).
He proceeded to receive two additional cycles of gem/cis in June 2024. In August 2024 following the completion of 5 cycles total of gem/cis, his MRI demonstrated nacVI-RADS score 1, and he had a complete response on repeat TURBT.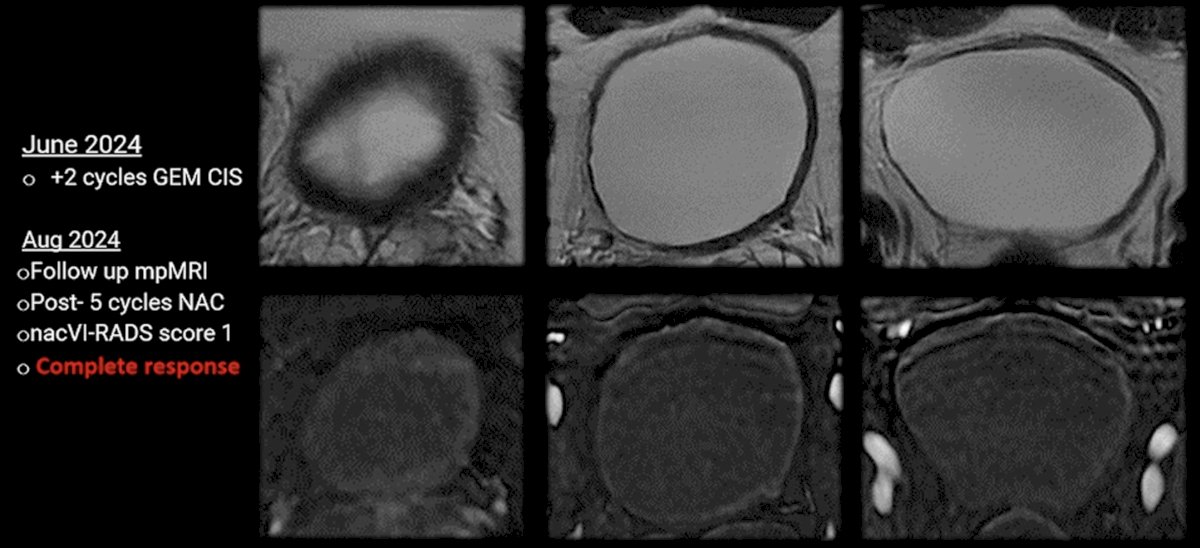
In summary, this was a case of a sexually active 67-year-old male with an excellent performance status with the following history:
- Non-metastatic focal MIBC, HG T2
- High-risk features, including CIS, LVI, multifocal tumors, 3cm, persistent disease at repeat TURBT
- No variant histology (pure urothelial)
- Complete response to systemic therapy (nacVI-RADS 1)
What are the next best steps in management?
- Avoid radiation – systemic therapy is enough
- Radiation is mandatory with systemic therapy
- Surgery is mandatory with systemic therapy
Dr. Porten began her argument in favor of systemic therapy alone in this setting by reminding the audience of what matters most to patients (data from a survey of non-muscle invasive bladder cancer patients; in order):
- Preserving the bladder
- Two-year recurrence-free survival
- Complete responses
Thus, we see that quality of life and avoiding the toxicity of radical therapy (radical cystectomy, TMT) is a high priority for bladder cancer patients.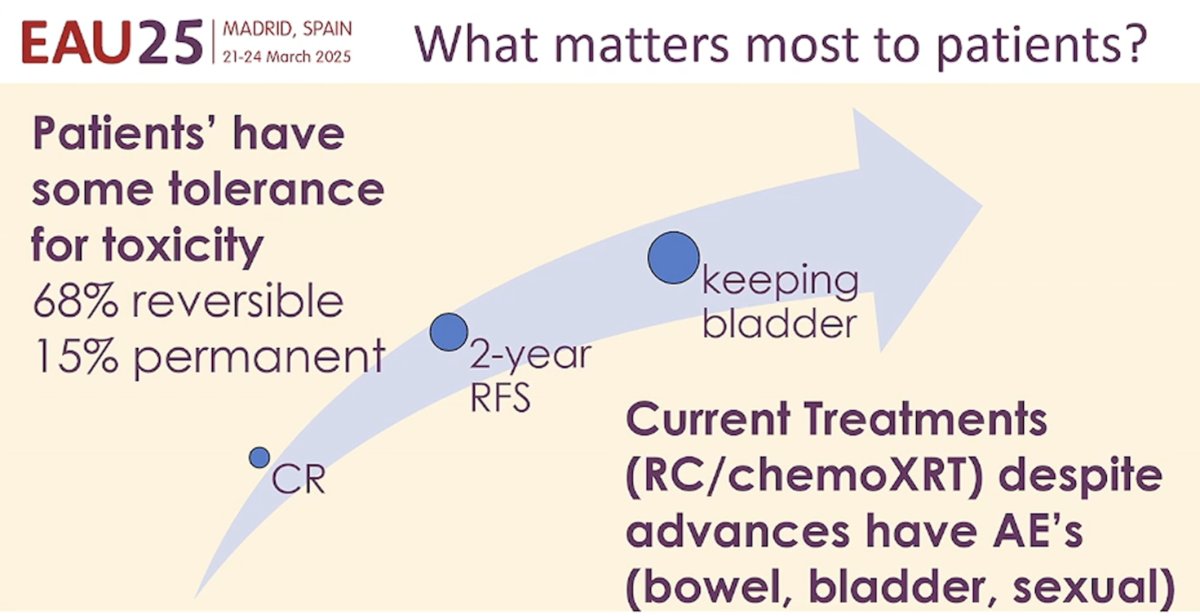
Could we proceed with surveillance and avoid local therapy? The current EAU MIBC guidelines suggest that such an approach is feasible:
- Overtreatment is a possible negative consequence of radical cystectomy
- NAC alone can produce a clinical complete response in up to 56% of cases but rarely produces durable complete responses
- Bladder conserving strategies with TUR and systemic chemotherapy could lead to long-term survival in select patient
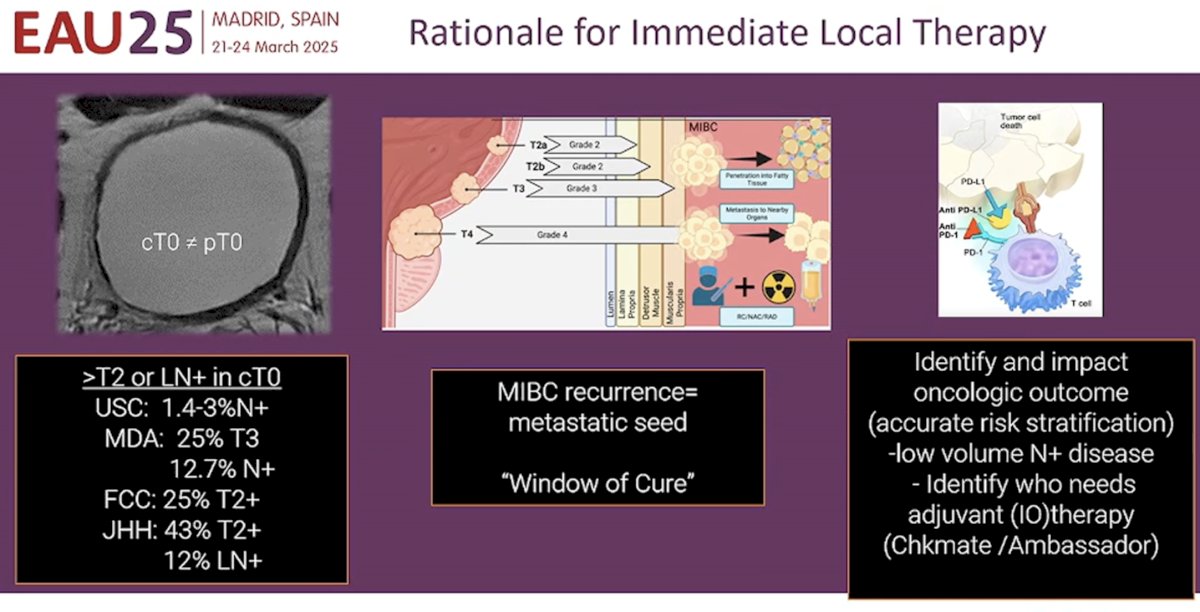
What is the rationale for immediate local therapy? Advocates for local therapy in this setting will argue that even for patients with cT0 disease, ≥pT2 and pN+ disease will be present in up to 43% and 13% of cases, respectively. Furthermore, surgical extirpation can potentially identify and impact oncologic outcomes, while allowing for accurate risk stratification, and identifying those patients who need adjuvant immunotherapy.
However, emerging evidence from bladder-sparing trials suggest that this approach is not unreasonable in select patients. RETAIN was a single arm, non-inferiority phase II trial (NCT02710734) that included cT2-T3N0M0 urothelial carcinoma patients who underwent NAC with accelerated MVAC x 3 cycles. Pre-NAC TURBT specimens were sequenced for mutations in ATM, ERCC2, FANCC, or RB1. Patients with ≥1 mutation and no clinical evidence of disease by restaging TUR, urine cytology, and imaging post-NAC began pre-defined active surveillance. The remaining patients underwent bladder-directed therapy.
The trial design is summarized below:
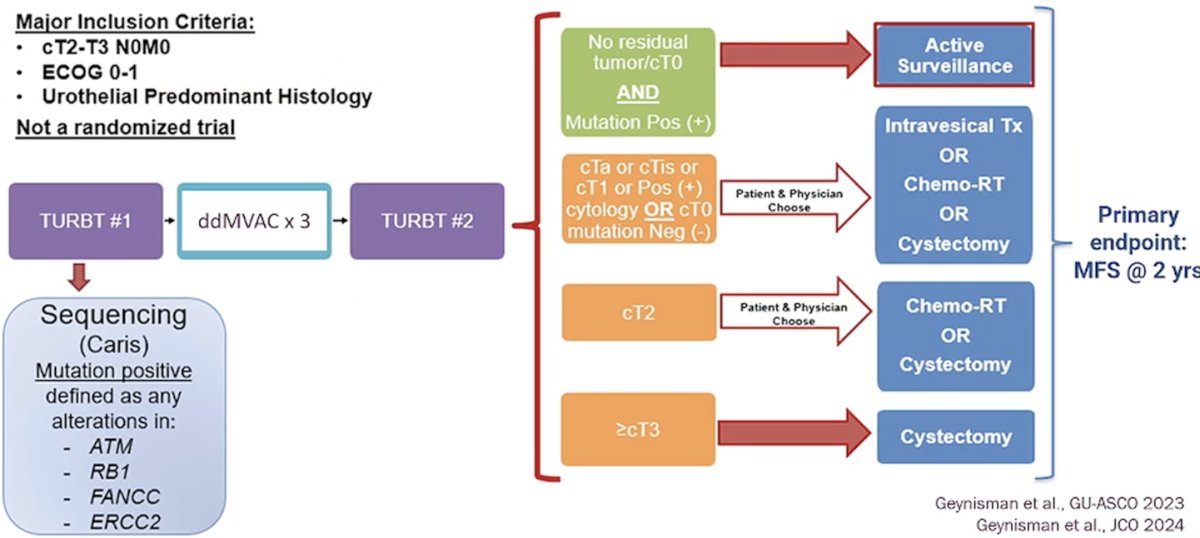
Of the 70 patients in the intent-to-treat (ITT) population, 25 were found to be mutation-positive and had no residual disease. All these patients, including an additional 3 who were either mutation negative or had residual disease, proceeded to active surveillance (n=28). In the overall ITT cohort (n=70), the 2-year metastasis-free survival rate was 73%.
In the cohort of 25 mutation-positive patients who proceeded to active surveillance, 17 (68%) experienced a recurrence. 8 patients underwent a cystectomy (7 for MIBC, 4 N+). Nine patients (36%) developed metastases, of whom 8/9 first recurred in the bladder. To date, 12 (48%) are metastasis-free with an intact, non-irradiated bladder.1
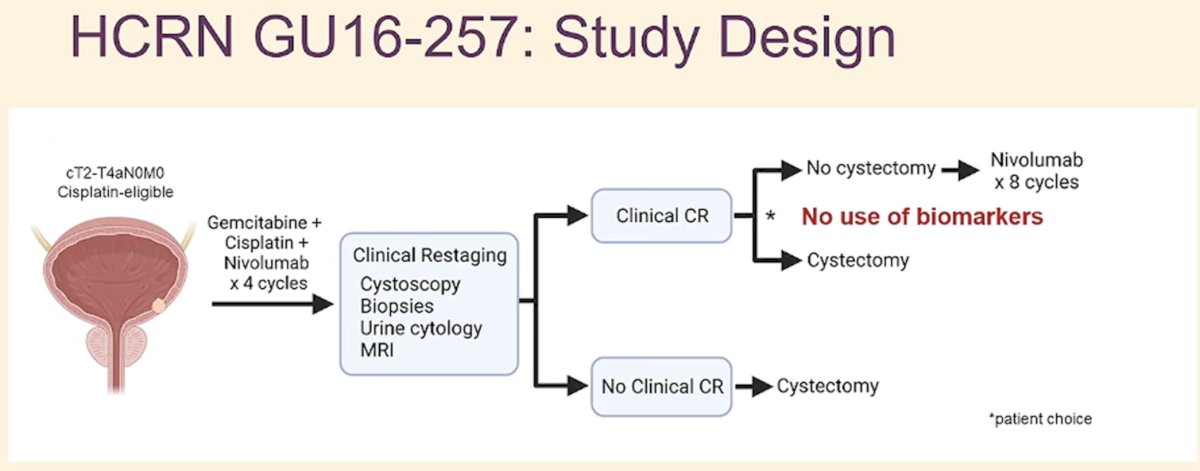
HCRN GU 16-257 was a phase II trial of cisplatin-eligible cT2-T4aN0M0 urothelial bladder cancer patients who received 4 cycles of gemcitabine, cisplatin, plus nivolumab (RETAIN – chemotherapy alone) followed by clinical restaging including urine cytology, MRI/CT of the bladder, cystoscopy and bladder biopsies (no use of biomarkers). Patients achieving a complete CR (normal cytology, imaging, and cT0/Ta) were eligible to proceed without cystectomy and receive nivolumab every 2 weeks x 8 followed by surveillance. Patients not achieving a clinical complete response were recommended to undergo cystectomy.2
Among the 72 eligible patients, 33 (43%) had a clinical complete response. One patient opted for cystectomy, whereas 32 proceeded to surveillance and received 8 additional cycles of nivolumab.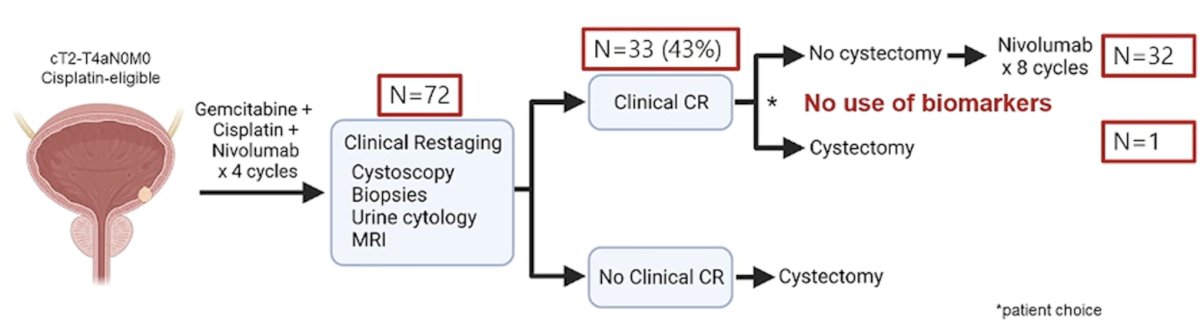
At two-year follow-up, 97% of patients with a clinical complete response remained alive and free of metastases, and 72.2% were alive with an intact bladder.2

As novel, more effective systemic therapy options emerge, including enfortumab vedotin + pembrolizumab (EV-304), it is likely that the requirement for local consolidation in patients with a clinical complete response will decrease.
Additionally, with the emergence of novel biomarkers, including circulating tumor DNA (ctDNA) and urinary tumor DNA (utDNA), improved assessment of ‘true’ complete clinical responses will allow for better selection of bladder-sparing candidates.

Dr. Porten concluded with the following take home messages in support of surveillance for MIBC patients with a complete clinical response following NAC:
- A composite definition of complete clinical response that incorporates mpMRI, CT chest, cytology, and TURBT with template biopsy identifies the best candidates for bladder-sparing approaches
- We need close, regimented surveillance and timely treatment of local recurrences
- Genomic predictors have not been identified yet, but biomarkers like ctDNA and utDNA may be useful
- Novel systemic therapy combinations may facilitate bladder-sparing approaches in a large proportion of MIBC patients
Next, Dr. Ananya Choudhury argued that radiation was mandatory with systemic therapy. She noted that there is now high-quality evidence to support the oncological equivalence of radical cystectomy and TMT in well-selected patients.3
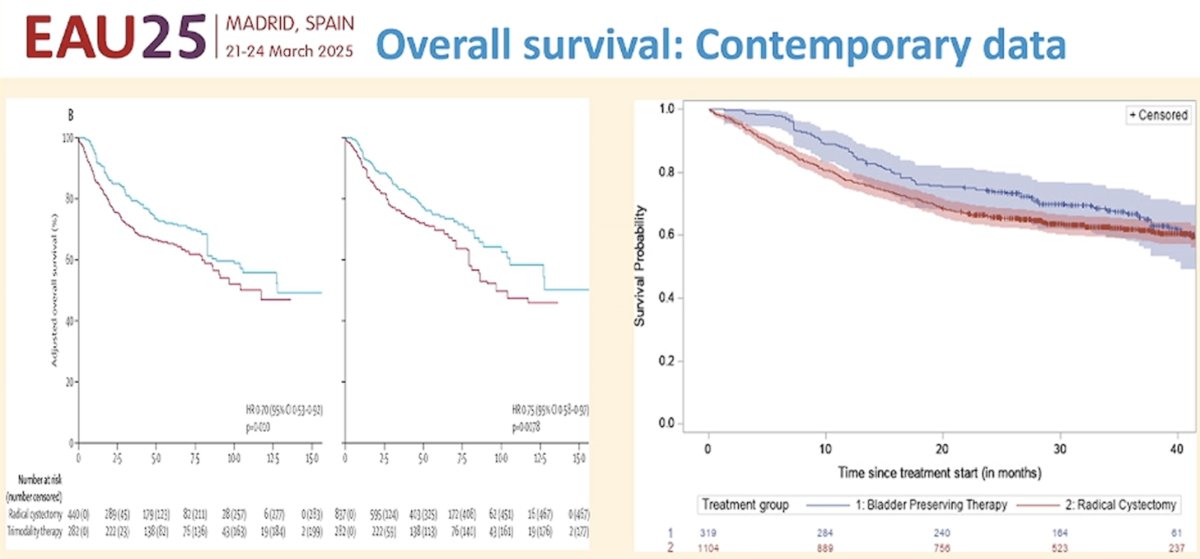
However, when we consider the side effect profile, studies suggest that TMT is associated with a less significant impact on quality-of-life outcomes,4 further supporting the use of radiotherapy consolidation in this setting. 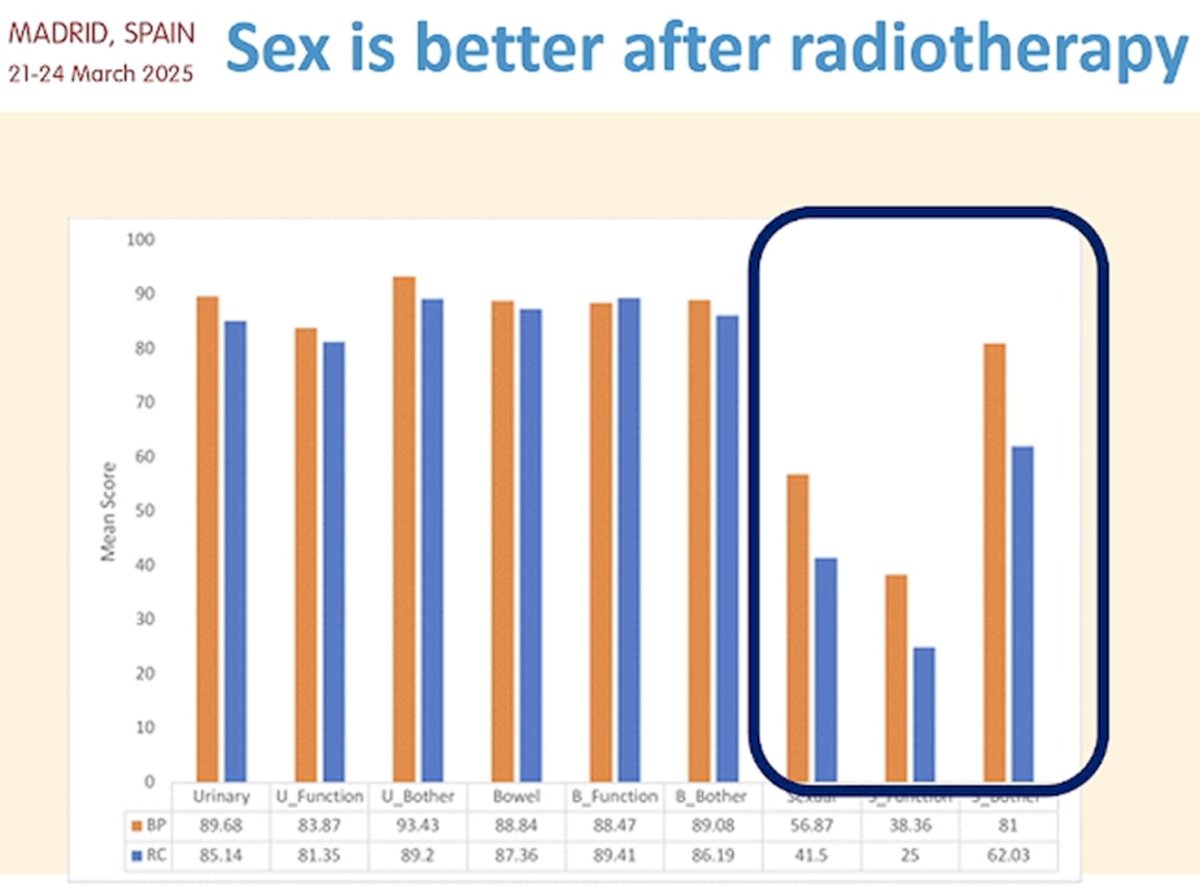
While systemic therapy options in the peri-operative setting continue to improve (e.g., peri-operative chemoimmunotherapy with durvalumab in the NIAGARA trial), Dr. Choudhury noted that a significant proportion of these patients continued to experience distant failure with short- to medium-term follow-up (2-year EFS in NIAGARA intervention arm: 68%).5 She, thus, argued that radiotherapy in this setting should be a critical component of treating MIBC patients.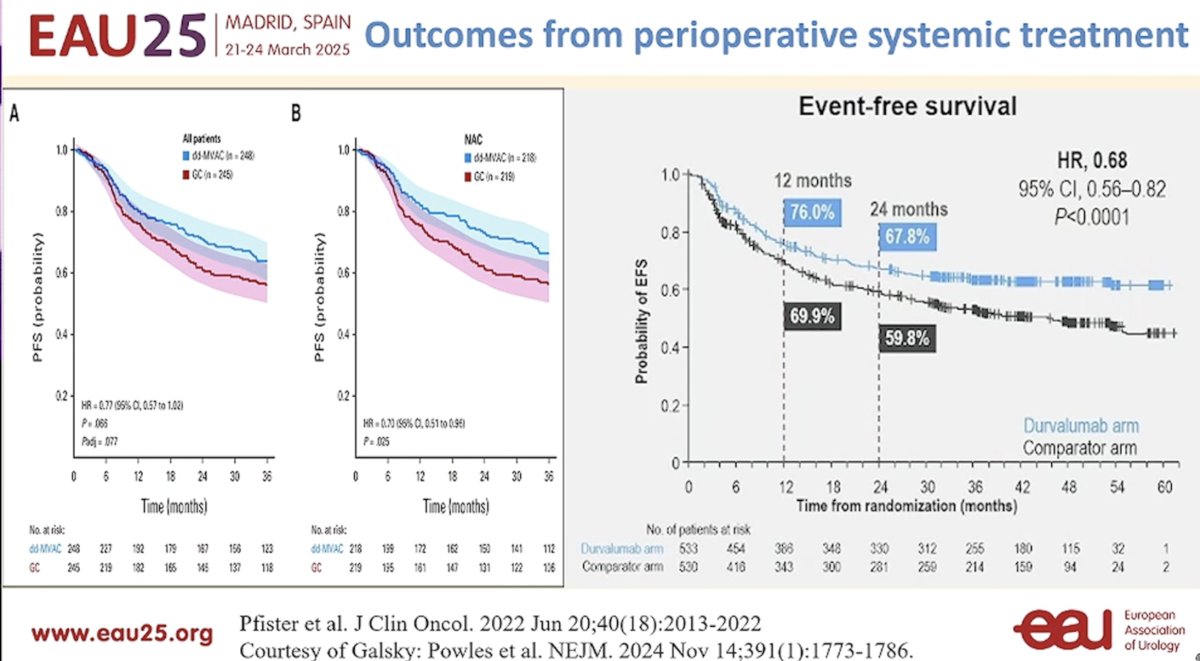
With regards to systemic therapy alone, she noted that there are ‘too many unknowns’. As such, the EAU guidelines currently recommend against offering chemotherapy alone as primary therapy for localized bladder cancer (strong recommendation). Numerous questions remain regarding the role of immunotherapy for bladder-sparing strategies, how to measure a complete response, and how to incorporate biomarkers in this setting.
Dr. Choudhury argued that if we really want to attempt de-escalation strategies, why not consider dose-adaptive radiotherapy strategies instead? Huddart et al. recently published the results of RAIDER, an international phase II trial that randomized 245 patients with unifocal T2-4a urothelial carcinoma of the bladder to standard whole bladder radiotherapy, standard-dose adaptive radiotherapy (SART), or dose-escalated adaptive radiotherapy (DART). Two-year overall survival was 77% for WBRT + SART and 80% for DART (hazard ratio=0.84, p=0.4). Radiotherapy-related grade ≥3 toxicity was reported in only 1 patient. Only 3.8% of patients underwent a salvage cystectomy within a median follow-up of ~40 months.6 These results support the adoption of contemporary, dose-adapted radiotherapy approaches for patients similar to that presented to begin the session.
Finally, Dr. Paolo Gontero argued in favor of surgery being mandatory in this setting. He highlighted the fact that a clinical complete response does not always correlate with a pathologic complete response at cystectomy. In the PURE-01 trial, 34% of patients with a radiologic complete response following neoadjuvant pembrolizumab had residual disease in their cystectomy specimen.7 The MRI criteria for defining a radiologic complete response are not validated, and 10% of residual tumors are missed by experience radiologists using nacVIRADS. How can we even visualize CIS on MRI? Additionally, even when repeat TURBT is incorporated into the clinical complete response assessment, this remains unreliable with 60% of patients with cT0 on repeat TURBT post-chemotherapy having evidence of residual disease.8 Overall, Dr. Gontero’s argument is that this patient is at significant risk of having residual disease present and needs local therapy.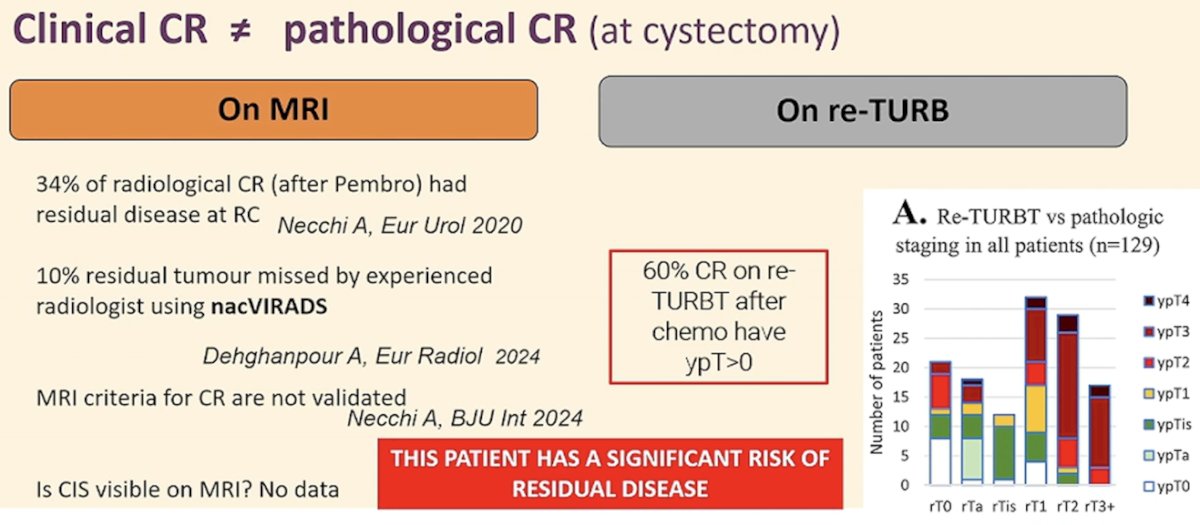
But why surgery over TMT? An important point in this case scenario is that this patient does not meet the classical TMT eligibility criteria. This patient has multifocal disease and CIS, both of which were exclusion criteria in the Zlotta et al. series from 2023.3 Thus, TMT in this patient is likely to be associated with worse outcomes, supporting a surgical approach in this patient.
Importantly, even in patients with a pathologic complete response (i.e., pT0), overall survival outcomes for pT0 patients who underwent radical cystectomy are superior to those who undergo TMT. Thus, Dr. Contero argued that not all pT0 patients are created equally, and the best opportunity for cure in these patients is with a radical cystectomy.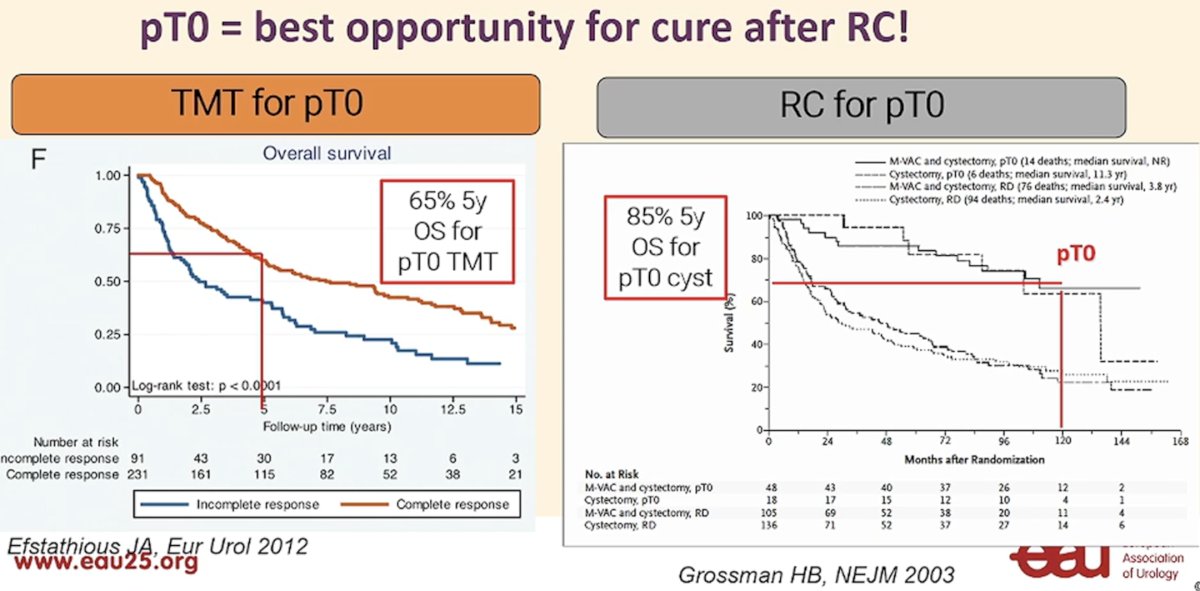
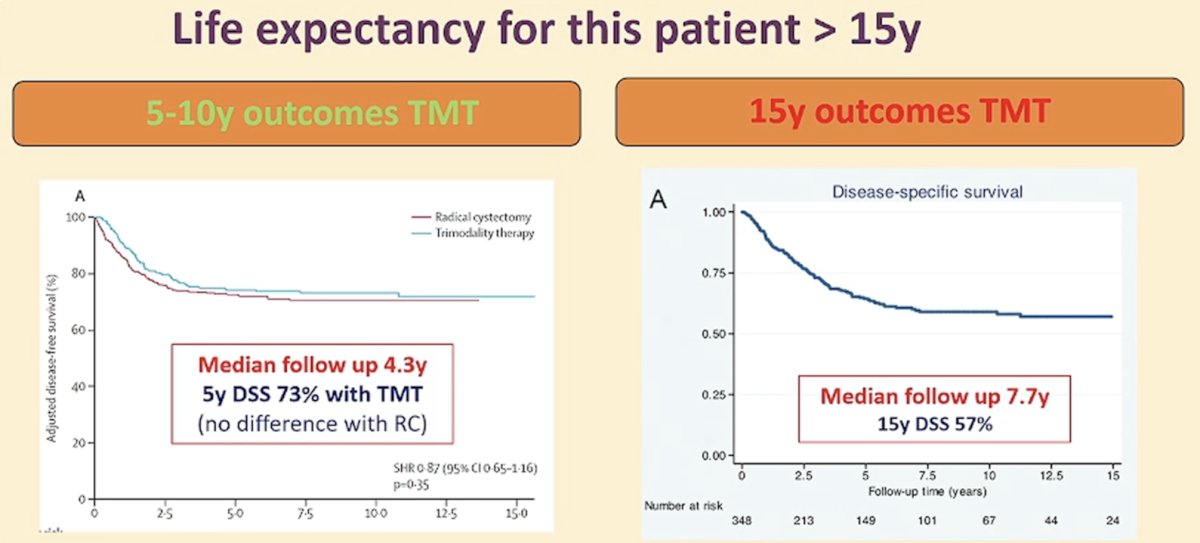
Another important limitation of the TMT literature is that patient follow-up post-TMT remains relatively short. This patient has a life expectancy of >15 years if he receives timely therapy, whereas the median follow-up in the Zlotta TMT series was only 4.3 years and 7.7 years in the MGH series.8
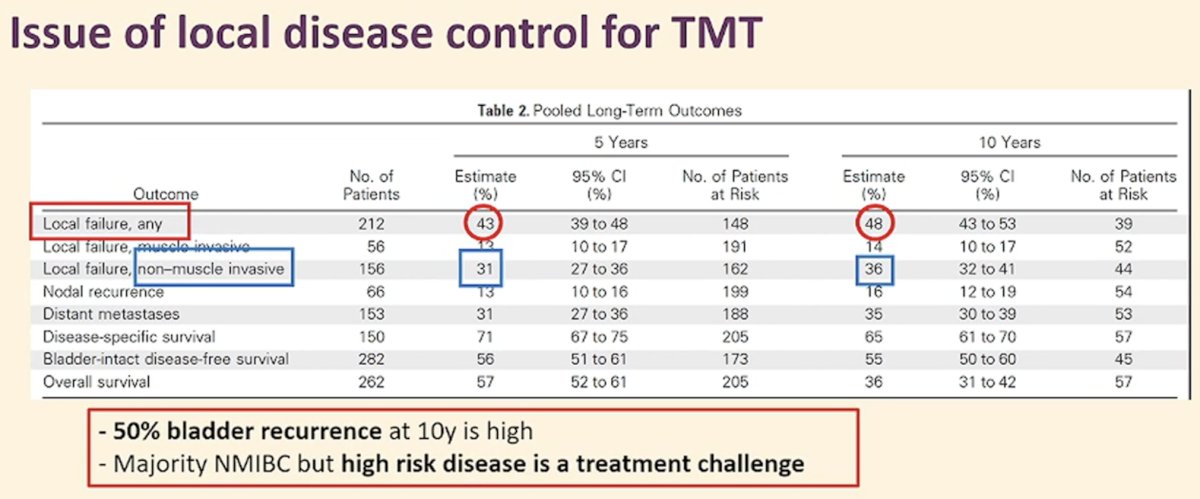
Another important consideration in the follow-up of TMT patients is that there is up to a 50% recurrence rate at 10 years. While the majority of these recurrences are non-invasive in nature, the treatment of recurrent/residual high-risk disease remains challenging.
Dr. Gontero concluded his argument in favor of surgical consolidation for this patient as follows:
- There is a high chance (≥33%) of having residual disease pathologically
- Surveillance alone is inadequate and not recommended
- There are several issues with TMT for this patient
- This patient does not meet the classic inclusion criteria for TMT
- Long-term outcomes are to be determined
- There is lifelong risk of bladder failure
- The best choice for a fit young patient: surgery + ‘maximal’ perioperative therapy
Presented by:
- Sima Porten, MD, MPH, Associate Professor, Urologic Oncologist, Department of Urology, UCSF, San Francisco, CA
- Ananya Choudhury, MA (Cantab), PhD, MRCP, FRCR, Professor, University of Manchester, Manchester, United Kingdom
- Paolo Gontero, MD, Professor of Urology, Chair, Department of Urology, University of Torino School of Medicine, Molinette Hospital, Torino, Italy
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 European Association of Urology (EAU) Annual Congress held in Madrid, Spain between March 21st and 24th, 2025
References:- Geynisman DM, Abbosh PH, Ross E, et al. Phase II Trial of Risk-Enabled Therapy After Neoadjuvant Chemotherapy for Muscle-Invasive Bladder Cancer (RETAIN 1). J Clin Oncol. 2025; 43(9):1113-1122.
- Galsky MD, Daneshmand S, Izadmehr S, et al. Gemcitabine and cisplatin plus nivolumab as organ-sparing treatment for muscle-invasive bladder cancer: a phase 2 trial. Natt Med. 2023; 29(11): 2825-34.
- Zlotta AR, Ballas LK, Miemierko A, et al. Radical cystectomy versus trimodality therapy for muscle-invasive bladder cancer: a multi-institutional propensity score matched and weighted analysis. Lancet Oncol. 2023; 24(6): 669-81.
- Murthy V, Kashid SR, Pal M, et al. Prospective comparative study of quality of life in patients with bladder cancer undergoing cystectomy with ileal conduit or bladder preservation. BMJ Oncol. 2024; 3(1): e000435.
- Powles T, Catto JWF, Galsky MD, et al. Perioperative Durvalumab with Neoadjuvant Chemotherapy in Operable Bladder Cancer. N Engl J Med. 2024; 391(19): 1773-86.
- Huddart R, Hafeez S, Griffin C, et al. Dose-escalated Adaptive Radiotherapy for Bladder Cancer: Results of the Phase 2 RAIDER Randomised Controlled Trial. Eur Urol. 2025; 87(1): 60-70.
- Mehr JP, Bates JN, Lerner SP. Is There A Benefit of Restaging Transurethral Resection of Bladder Tumor Prior to Radical Cystectomy With or Without Neoadjuvant Chemotherapy? Bladder Cancer. 2023; 9(1): 41-8.
- Efstathiou JA, Spiegel DY, Shipley WU, et al. Long-term outcomes of selective bladder preservation by combined-modality therapy for invasive bladder cancer: the MGH experience. Eur Urol. 2012; 61(4): 705-11.