(UroToday.com) The 2025 European Association of Urology (EAU) Annual Congress held in Madrid, Spain was host to a plenary session on organ-sparing paradigms in kidney and bladder cancer. Dr. Peter Black discussed whether current methods of complete response evaluation are adequate for appropriately selecting patients with muscle-invasive bladder cancer (MIBC) for bladder-sparing approaches.
Dr. Black emphasized that the current standard of care for MIBC remains morbid and de-intensification strategies are needed.
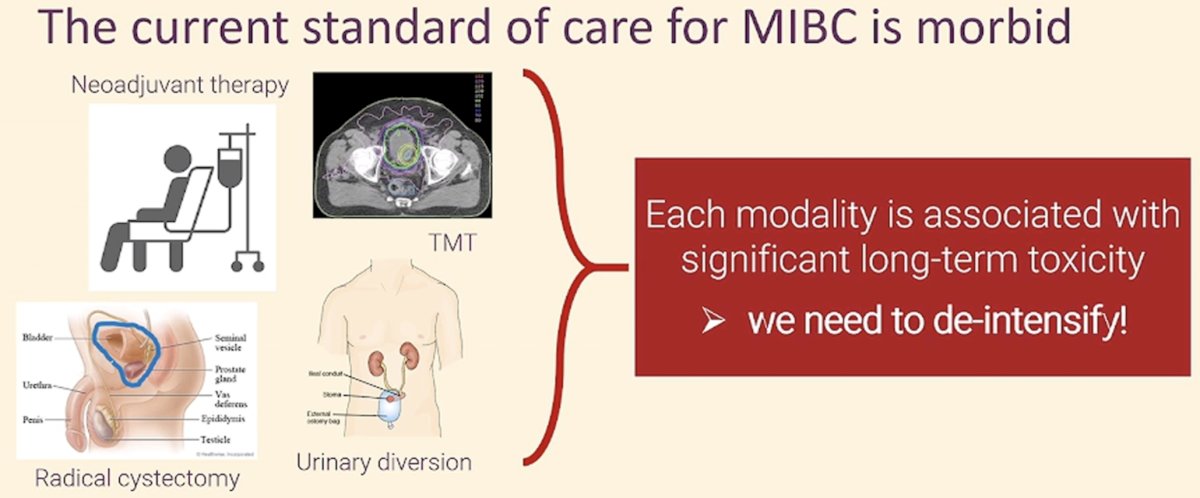
However, when considering de-intensification strategies involving active surveillance after neoadjuvant therapy (i.e., bladder-sparing approaches), there are two critical challenges:
- Do we have the tools necessary to determine complete response accurately?
- If we miss persistent disease, can we rescue these patients?
Current tools available for evaluating complete responses following neoadjuvant therapy, include cytology, CT chest/abdomen/pelvis, and a cystoscopy +/- TURBT:
To date, there are four trials evaluating bladder-sparing approaches for MIBC, of which three have been presented or published (RETAIN, HOOSIER, RETAIN 2):

RETAIN was a single arm, non-inferiority phase II trial (NCT02710734) that included cT2-T3N0M0 urothelial carcinoma patients who underwent neoadjuvant chemotherapy (NAC) with accelerated MVAC x 3 cycles. Pre-NAC TURBT specimens were sequenced for mutations in ATM, ERCC2, FANCC or RB1. Patients with ≥1 mutation and no clinical evidence of disease by restaging TUR, urine cytology and imaging post-NAC began pre-defined active surveillance. The remaining patients underwent bladder-directed therapy.
The trial design is summarized below:
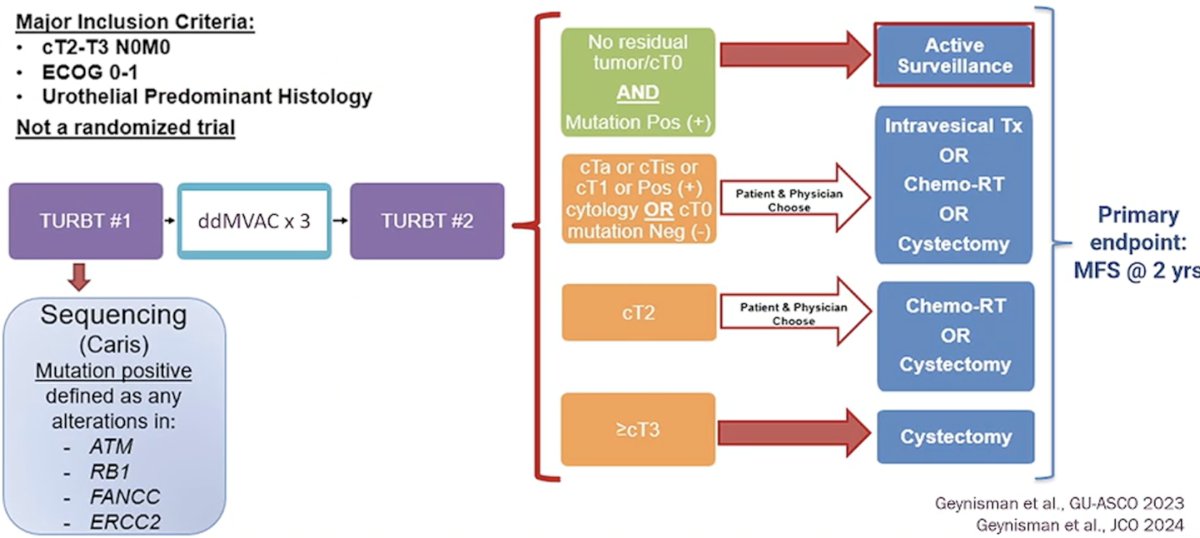
Of the 70 patients in the intent-to-treat (ITT) population, 25 were found to be mutation-positive and had no residual disease. All these patients, including an additional 3 who were either mutation negative or had residual disease, proceeded to active surveillance (n=28). In the overall ITT cohort (n=70), the 2-year metastasis-free survival rate was 73%.

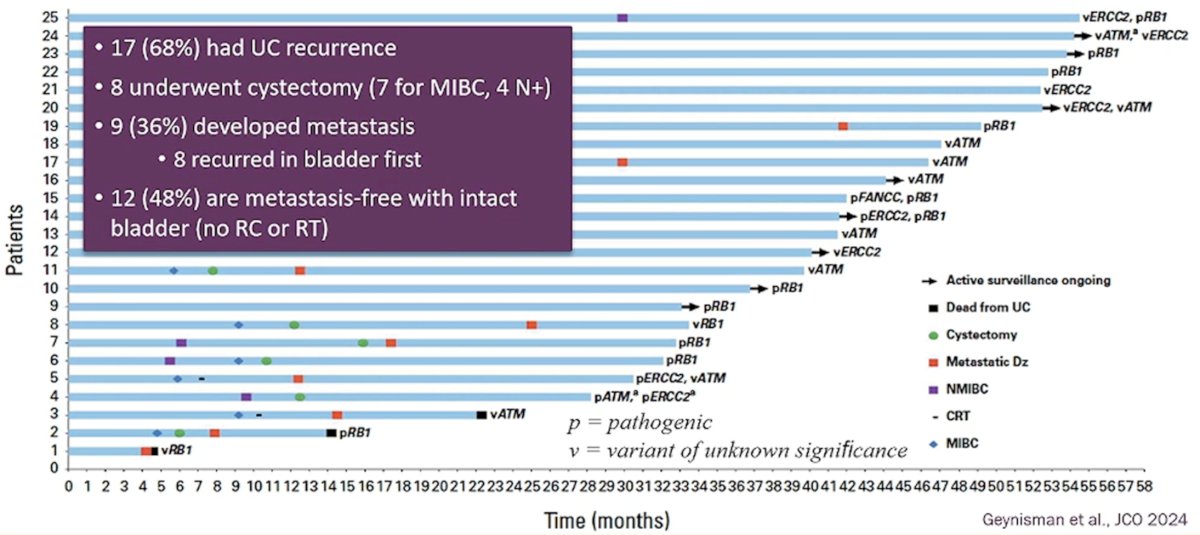
In the cohort of 25 mutation-positive patients who proceeded to active surveillance, 17 (68%) experienced a recurrence. 8 patients underwent a cystectomy (7 for MIBC, 4 N+). Nine patients (36%) developed metastases, of whom 8/9 first recurred in the bladder. To date, 12 (48%) are metastasis-free with an intact bladder (no radical cystectomy or radiotherapy).
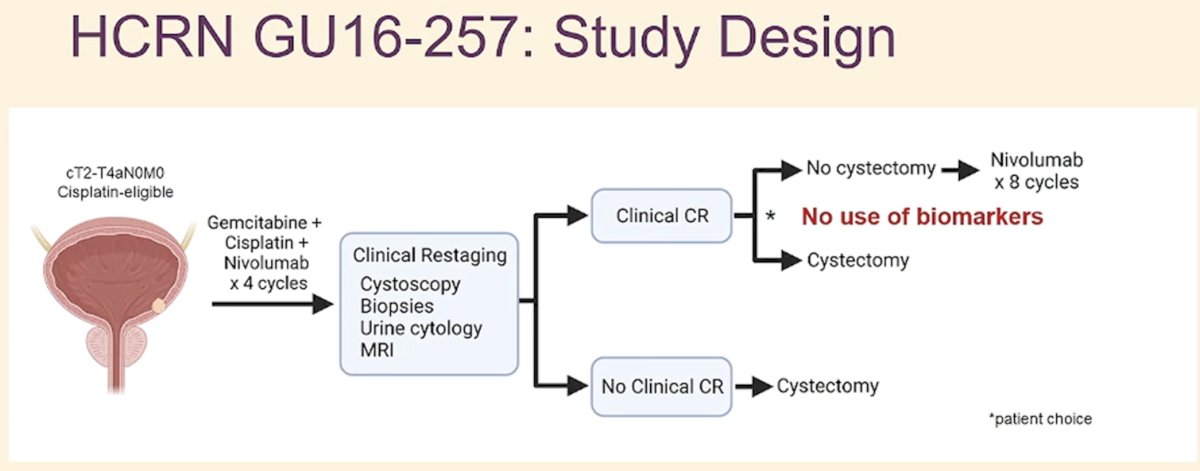
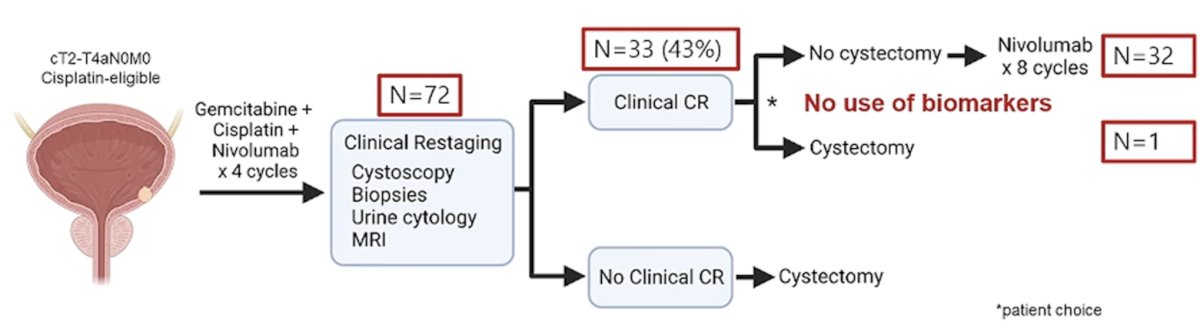
HCRN GU 16-257 was a phase II trial of cisplatin-eligible cT2-T4aN0M0 urothelial bladder cancer patients who received 4 cycles of gemcitabine, cisplatin, plus nivolumab (RETAIN – chemotherapy alone) followed by clinical restaging including urine cytology, MRI/CT of the bladder, cystoscopy and bladder biopsies (no use of biomarkers). Patients achieving a complete CR (normal cytology, imaging, and cT0/Ta) were eligible to proceed without cystectomy and receive nivolumab every 2 weeks x 8 followed by surveillance. Patients not achieving a clinical complete response were recommended to undergo cystectomy.2
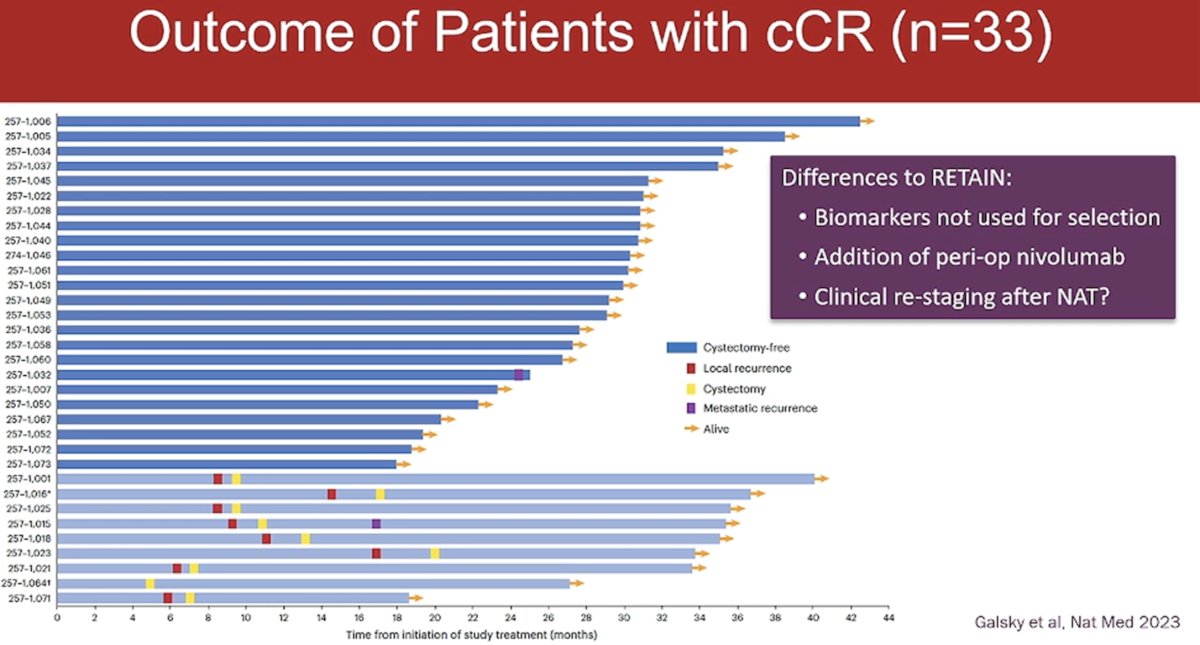
Among the 72 eligible patients, 33 (43%) had a clinical complete response. One patient opted for cystectomy, whereas 32 proceeded to surveillance and received 8 additional cycles of nivolumab.
At two-years follow-up, 97% of patients with a clinical complete response remained alive and free of metastases, and 72.2% were alive with an intact bladder.2
Notable differences between HCRN GU 16-257 and RETAIN included the following:
- Biomarkers were used for the selection of patients for bladder-sparing approaches in RETAIN (ATM, RB1, FANCC, ERCC2), but not HCRN GU 16-257
- Chemoimmunotherapy was used in HCRN GU 16-257 and patients received peri-operative nivolumab
- Differences in clinical re-staging following neoadjuvant therapy
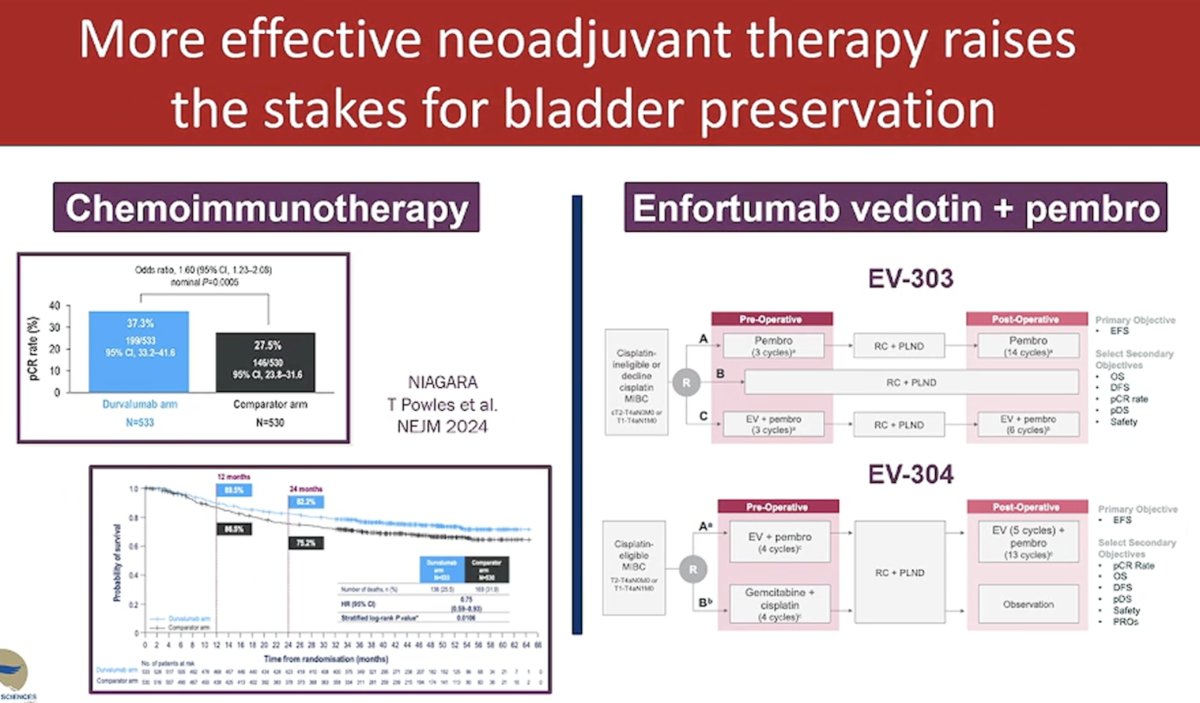
Dr. Black noted that the paradigm for bladder-sparing approaches is likely to evolve with the emergence of novel systemic therapy combination approaches, including perioperative durvalumab with neoadjuvant chemotherapy (NIAGARA)3 and enfortumab vedotin + pembrolizumab (EV-303, EV-304).
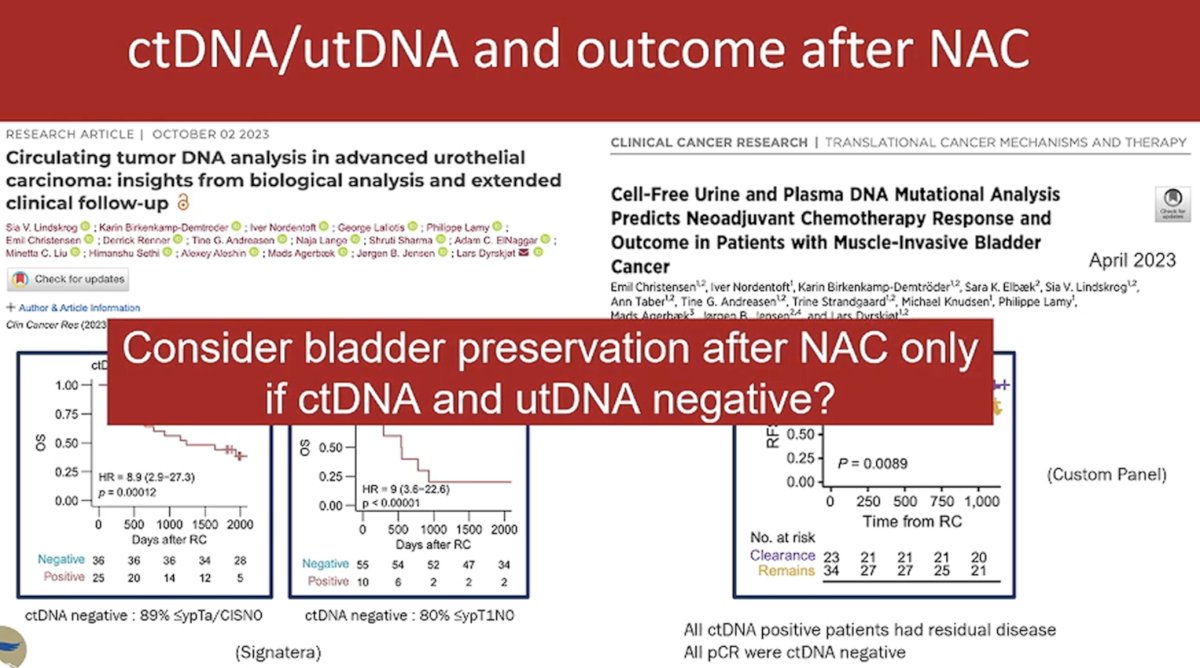
The next ‘wave’ of tools for determining complete response is likely to incorporate urinary tumor DNA (utDNA), circulating tumor DNA (ctDNA), and MRI (VI-RADS scoring system).
The prognostic utility of ctDNA has clearly been established. Following a radical cystectomy, ctDNA has a sensitivity of 94% and a specificity of 98% for identifying metastatic relapses. During NAC, ctDNA dynamics are independently associated with patient outcomes when adjusted for pathologic downstaging (HR: 4.7; p=0.029). For NAC-naïve patients, ctDNA is a prognostic predictor before (HR:3.4; p=0.0005) and after radical cystectomy (HR:17.8; p=0.0002).4
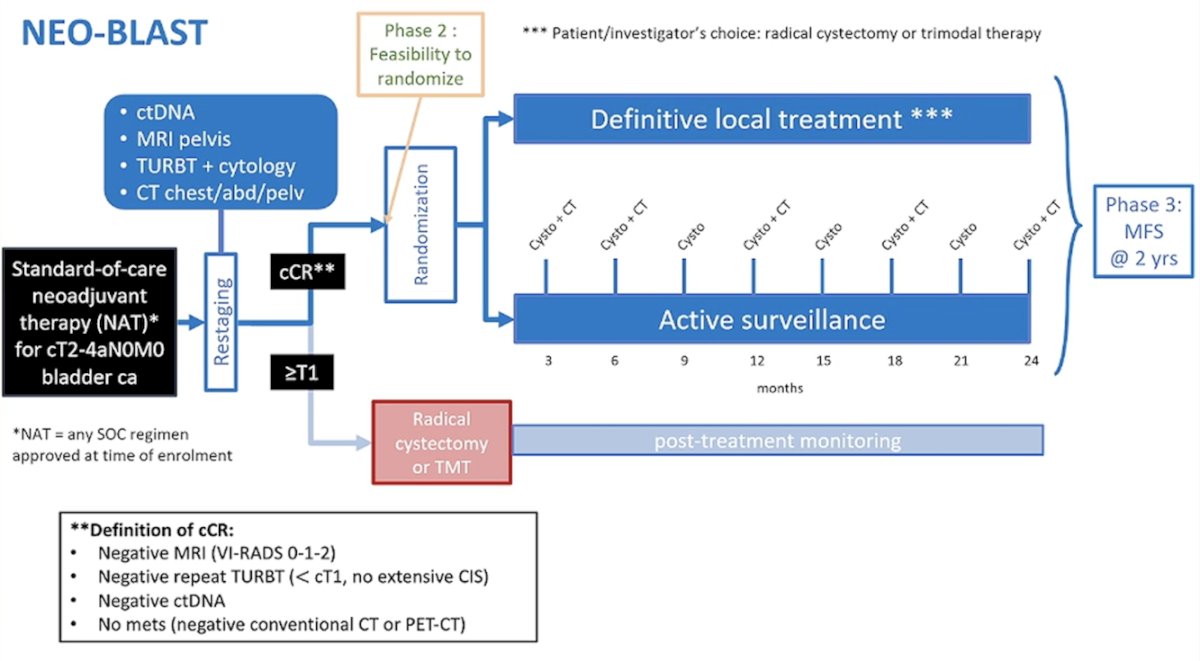
Dr. Black concluded by highlighting the NEO-BLAST trial, which is investigating neoadjuvant therapy for MIBC, incorporating ctDNA as part of the criteria to assess clinical complete response. Patients who achieve a complete response may proceed with local definitive treatment or surveillance instead of radical cystectomy.
Presented by: Peter Black, MD, Senior Research Scientist, Vancouver Prostate Centre, Professor, Department of Urologic Sciences, University of British Columbia, Vancouver Prostate Center
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the European Association of Urology (EAU) 2025 Annual Meeting, Madrid, Spain, Fri, Mar 21 – Mon, Mar 24, 2025.
References:
- Geynisman DM, Abbosh PH, Ross E, et al. Phase II Trial of Risk-Enabled Therapy After Neoadjuvant Chemotherapy for Muscle-Invasive Bladder Cancer (RETAIN 1). J Clin Oncol. 2025; 43(9):1113-1122.
- Galsky MD, Daneshmand S, Izadmehr S, et al. Gemcitabine and cisplatin plus nivolumab as organ-sparing treatment for muscle-invasive bladder cancer: a phase 2 trial. Natt Med. 2023; 29(11): 2825-34.
- Powles T, Catto JWF, Galsky MD, et al. Perioperative Durvalumab with Neoadjuvant Chemotherapy in Operable Bladder Cancer. N Engl J Med. 2024; 391(19): 1773-86.
- Lindskrog SV, Birkenkamp-Demtroder K, Nordentoft I, et al. Circulating Tumor DNA Analysis in Advanced Urothelial Carcinoma: Insights from Biological Analysis and Extended Clinical Follow-up. Clin Cancer Res. 2023; 29(23): 4797-807.
- Christensen E, Birkenkamp-Demtroder, Sethi H, et al. Early Detection of Metastatic Relapse and Monitoring of Therapeutic Efficacy by Ultra-Deep Sequencing of Plasma Cell-Free DNA in Patients With Urothelial Bladder Carcinoma. J Clin Oncol. 2019; 37(18): 1547-57.