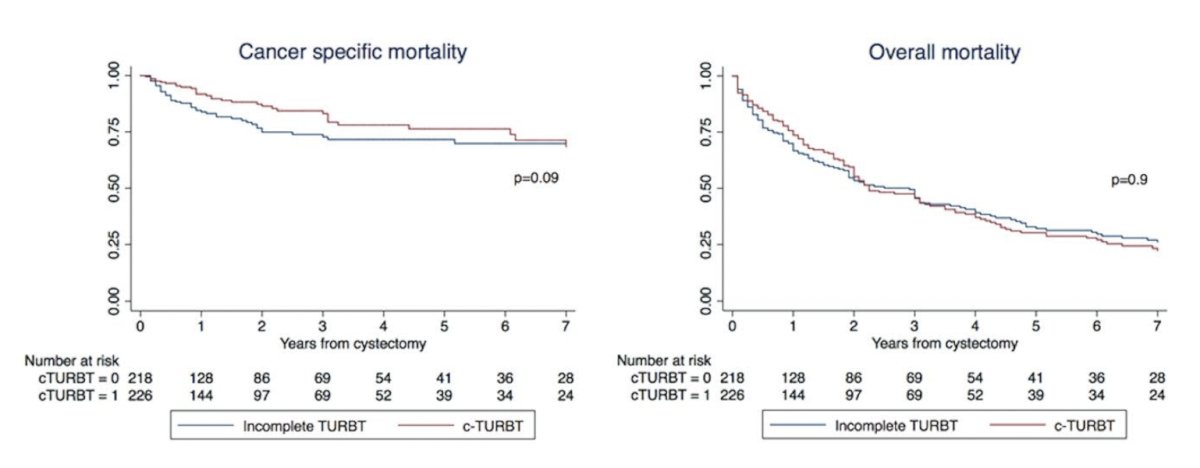
(UroToday.com) The 2025 EAU annual meeting featured a rapid-fire debate session on common problems and controversies in bladder cancer and a presentation by Dr. Marco Moschini contending that for muscle invasive bladder cancer, only a diagnostic TURBT is sufficient. Dr. Moschini started his presentation by highlighting a study from Zamboni et al.1 that assessed the impact of completeness of last transurethral resection of bladder tumors on the outcomes of radical cystectomy. Among 727 patients from three tertiary care centers (2001-2018), 433 (60%) of patients received a complete TURBT. This study noted no significant survival benefit observed for complete versus not complete TURBT with regards to overall (p = 0.9) and cancer specific mortality (p = 0.09):
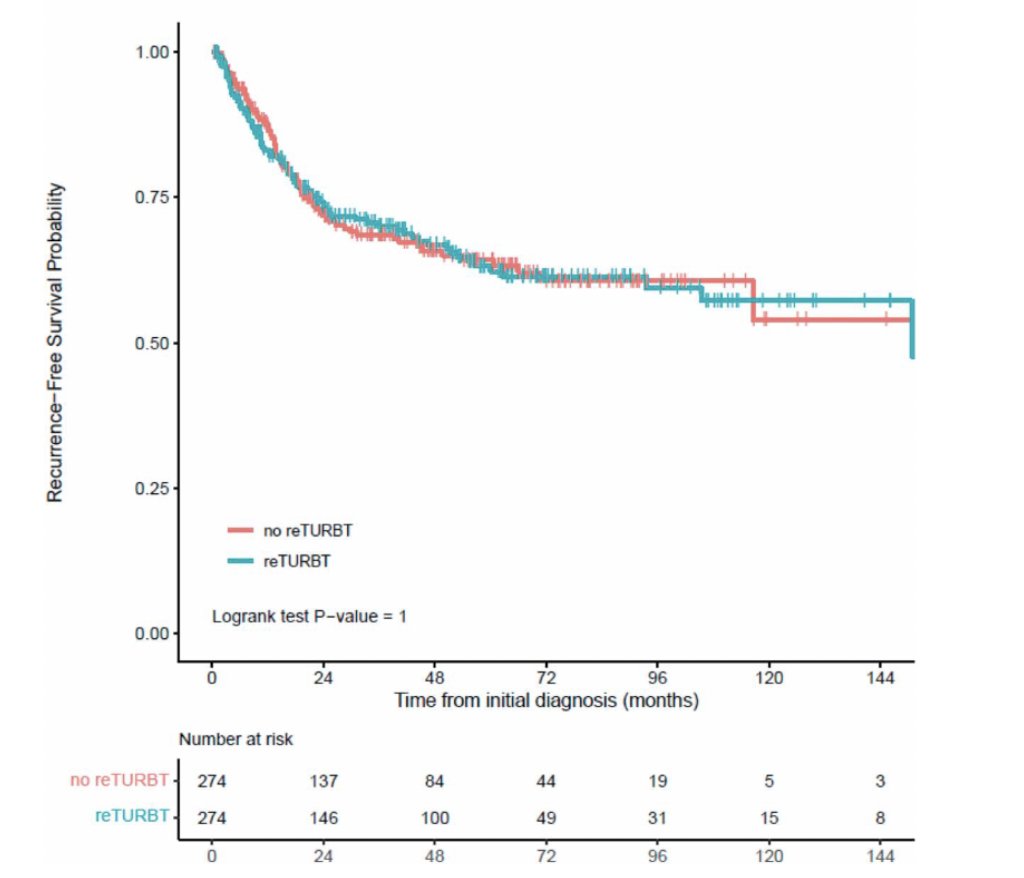
In another retrospective cohort study of 657 patients with clinical stage T2N0 muscle invasive bladder cancer, Bree et al.2 assessed the utility of repeat TURBT prior to radical cystectomy. After propensity score matching done by age, gender, receipt of neoadjuvant chemotherapy, preoperative hydronephrosis, variant histology, lymphovascular invasion, or CIS, they found that Kaplan-Meier estimates of recurrence-free (p = 1.0) and overall survival (p = 0.30) demonstrated no significant difference based upon performance of repeat TURBT:

Does grossly complete TURBT improve response to neoadjuvant chemotherapy? Ghandour et al3 sought to answer this question, assessing 100 muscle invasive bladder cancer patients (from 2011-2018) treated with cisplatin based neoadjuvant chemotherapy prior to radical cystectomy. There were 49 patients that underwent complete resection while 51 patients underwent incomplete resection prior to neoadjuvant chemotherapy. On logistic regression, there was no association between completeness of TURBT and ypT0 or ypT < 2 rates.
Dr. Moschini then discussed trimodality therapy, noting that a pooled analysis of RTOG trials 8802, 8903, 9506, 9706, 9906, and 0233 showed that overall survival and disease specific survival was 57% and 71%, respectively, which is similar to studies of radical cystectomy in patients with similarly staged muscle invasive bladder cancer.4 Additionally, in the BC2001 trial,5 radiotherapy with or without synchronous chemotherapy with fluorouracil and mitomycin C showed that chemoradiotherapy significantly improved 2-year locoregional disease-free survival (67% versus 54% in the radiotherapy group). In the Zlotta et al.6 2023 trimodality therapy study, this retrospective analysis included 703 patients with muscle invasive bladder cancer clinical stage T2-T3/4aN0M0. Specifically, there were 421 radical cystectomy patients and 282 trimodality therapy patients who would have been eligible for both trimodality therapy or radical cystectomy (from 2005 to 2017). To compare homogeneous cohorts, all patients included in this analysis had solitary tumors <7 cm, no unilateral hydronephrosis, and no extensive carcinoma in situ. Treatment propensity scores were estimated using logistic regression, and patients were matched 3:1, with the covariates including age, sex, clinical T stage (cT2 vs cT3-4), hydronephrosis, (neo)adjuvant chemotherapy, body mass index, smoking history, and ECOG status. The 5-year metastasis free survival, disease free survival, and cancer specific survival were similar between the two groups, while trimodality therapy was associated with better overall survival (HR 0.75, 95% CI 0.58-0.97), in part secondary to a 2.5% perioperative mortality in the radical cystectomy group:

Finally, Dr. Moschini discussed a recent study by Longoni et al.7 assessing survival after trimodality therapy in octogenarians with organ-confined bladder cancer within the SEER database (2004-2021). Among 2,335 octogenarian patients with T2N0M0 urothelial carcinoma, 1,562 (66.3%) received trimodality therapy and 793 (33.7%) received radical cystectomy. The 5-year cancer specific mortality rate was 50.1% for trimodality therapy versus 31.1% for radical cystectomy, and the 5-year overall mortality rate was 25.1% for trimodality therapy versus 20.6% for radical cystectomy:

Dr. Moschini concluded his presentation by discussing that for muscle invasive bladder cancer, only a diagnostic TURBT is sufficient with the following take home points:
- In cases planned for radical cystectomy or neoadjuvant chemotherapy, TURBT should focus on confirming muscle invasive (T2), and accurate sampling is essential to identify histological variants rather than complete resection
- The optimal candidates for trimodal therapy are those with low volume T2-T4a urothelial carcinoma with focal CIS, no hydronephrosis, and good bladder and lower urinary tract function
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the European Association of Urology (EAU) 2025 Annual Meeting, Madrid, Spain, Fri, Mar 21 – Mon, Mar 24, 2025.
References:
- Zamboni S, Moschini M, Gallina A, et al. The impact of completeness of last transurethral resection of bladder tumors on the outcomes of radical cystectomy. World J Urol. 2019 Dec;37(12):2707-2714.
- Bree KK, Kokorovic A, Westerman ME, et al. Repeat transurethral resection of muscle-invasive bladder cancer prior to radical cystectomy is prognostic but not therapeutic. J Urol. 2023 Jan;209(1):140-149.
- Ghandour RA, Kusin S, Wong D, et al. Does grossly complete transurethral resection improve response to neoadjuvant chemotherapy Urol Oncol. 2020 Sep;38(9):736.e11-736.e18.
- Mak RH, Hunt D, Shipley WU, et al. Long-term outcomes in patients with muscle-invasive bladder cancer after selective bladder-preserving combined-modality therapy: A pooled analysis of Radiation Therapy Oncology Group protocols 8802, 8903, 9506, 9706, 9906, and 0233. J Clin Oncol. 2014 Dec 1;32(34):3801-3809.
- James ND, Hussain SA, Hall E, et al. Radiotherapy with or without chemotherapy in muscle-invasive bladder cancer. N Engl J Med. 2012 Apr 19;366(16): 1477-1488.
- Zlotta AR, Ballas LK, Niemierko A, et al. Radical cystectomy versus trimodality therapy for muscle-invasive bladder cancer: A multi-institutional propensity score matched and weighted analysis. Lancet Oncol. 2023 Jun;24(6):669-681.
- Longoni M, Di Bello F, Penaranda NR, et al. Survival after trimodal therapy in octogenarians with organ-confined urothelial bladder cancer. BJU Int. 2024 Dec 12 [Epub ahead of print].