(UroToday.com) The 2025 EAU annual meeting featured a rapid-fire debate session on common problems and controversies in bladder cancer and a presentation by Dr. Fredrik Liedberg contending that for muscle invasive bladder cancer, a maximal TURBT is needed. Dr. Liedberg started his presentation by highlighting that for a 79 year old male with diabetes and a history of a stroke with cT3N0M0 bladder cancer, the options are either radical cystectomy or trimodality therapy. Because at the time of the TURBT, this decision may not have yet been made, in his opinion, a maximal TURBT is required.
To date, there has been some concern that a maximal TURBT before radical cystectomy may affect the level of circulating tumor cells. However, Dr. Liedberg notes that the circulating tumor cells are already there preoperatively, and keeping the irrigation bags low during the TURBT may decrease the risk of increasing circulating tumor cell levels. In situations where an incomplete TURBT is done prior to radical cystectomy, there is an increased risk of postoperative bleeding and clot retention, and a maximal TURBT may be a bridge to radical cystectomy without hematuria episodes, especially in patients that may not receive neoadjuvant chemotherapy.
In 2022, Graffeille and colleagues1 assessed the impact of complete TURBT before radical cystectomy on pathological and oncological outcomes of patients with muscle-invasive bladder cancer. Among 486 patients included in the analysis, the TURBT immediately preceding radical cystectomy was considered macroscopically complete in 253 patients (52.1%) and incomplete in 233 patients (47.9%). After a median follow-up of 41 months, macroscopically complete TURBT was associated with better recurrence free survival (5-year rate: 57 versus 37%; p < 0.0001) and cancer specific survival (5-year rate: 70.8 versus 54.5%; p = 0.002).
In a study from Columbia University assessing the association of completeness of TURBT prior to neoadjuvant chemotherapy (n = 93, 67% underwent complete TURBT) with response and survival outcomes,2 patients with complete TURBT were more likely to defer radical cystectomy and pursue active surveillance/delayed intervention (61% versus 32%). Moreover, patients with complete TURBT had higher 5-year overall (77% versus 46%, p = 0.003) and cancer-specific (85% versus 50%, p = 0.001) survival: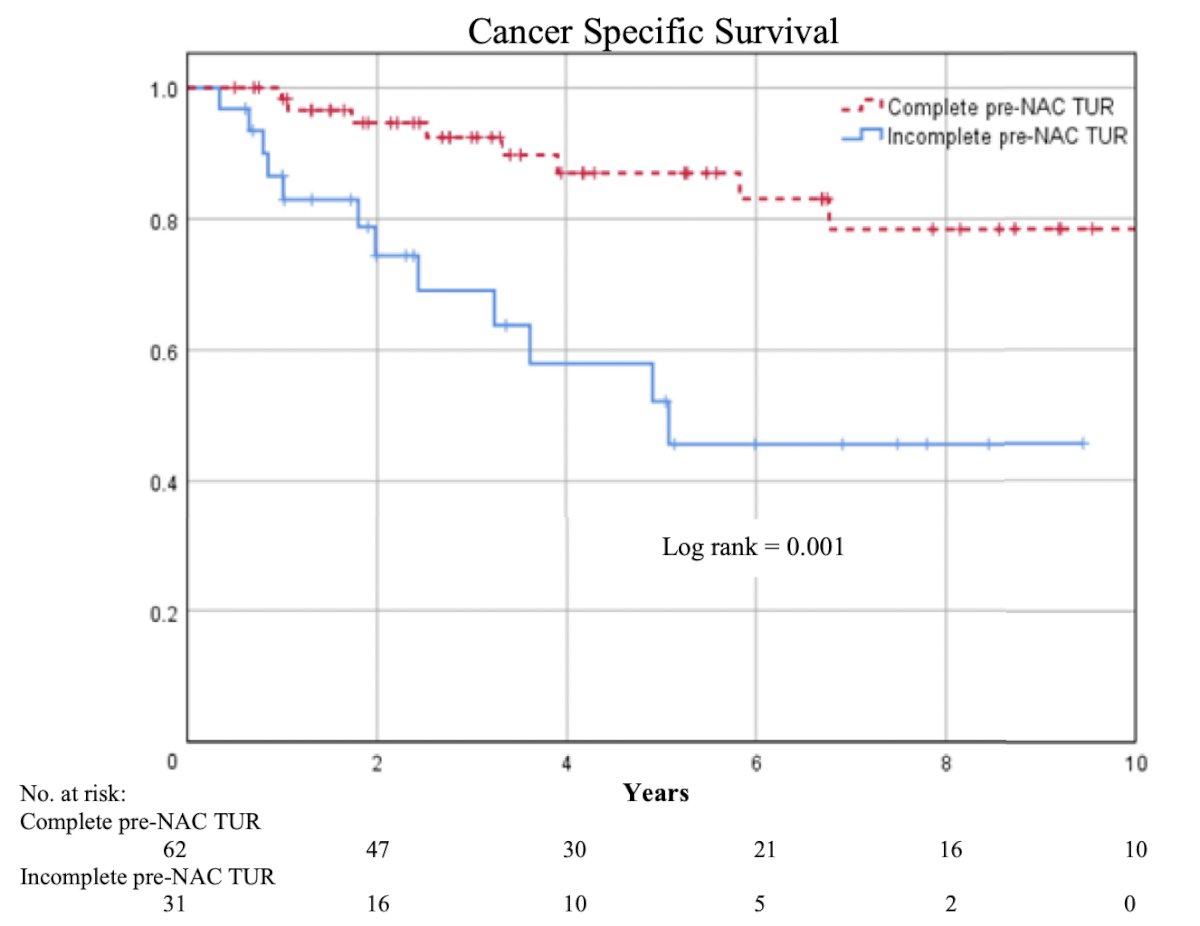
With regards to maximal TURBT prior to trimodality therapy, Dr. Liedberg notes that Suer et al.3 assessed the data of 90 patients (stage T2-4, N0-1, M0 urothelial cancer) who were treated with trimodality therapy. Of these, 43 patients had a second TURBT before starting chemoradiation (group 1), and 47 patients (group 2) were treated with chemoradiation without having a second TURBT. They found that the 5-year disease specific survival rate was better in group 1 compared to group 2 (68 versus 41 %) (p = 0.046):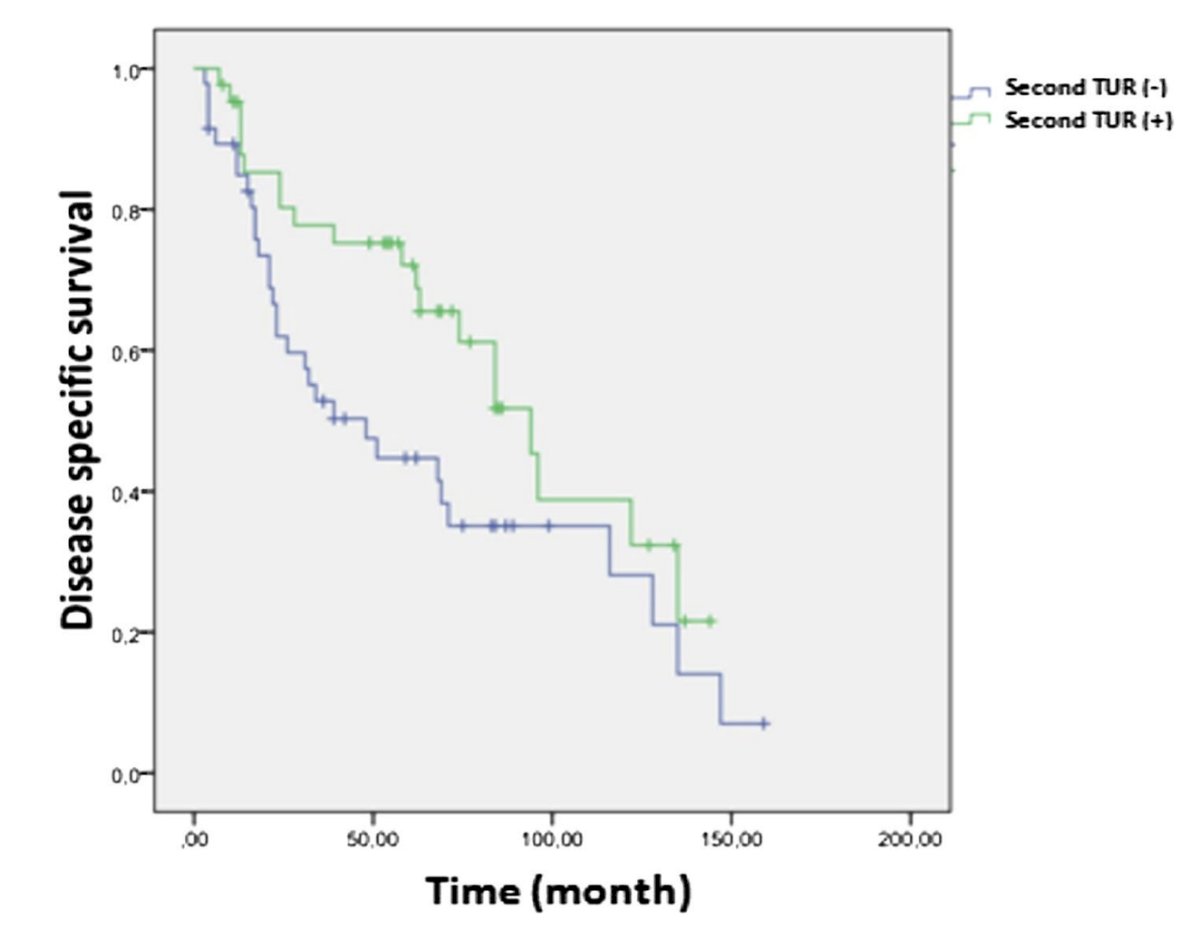
Another potential benefit of maximal TURBT prior to trimodality therapy is to remove potentially radio- and/or chemo-resistant tumors prior to therapy.
Is there a role for watchful waiting after maximal TURBT and chemotherapy? RETAIN 1, a single arm phase II trial with MRI, and HCRN GU16-257, a single arm phase II noninferiority trial, suggest there may be a role for this approach.
Dr. Liedberg concluded his presentation discussing that for muscle invasive bladder cancer, a maximal TURBT is needed with the following take home points:
- In patients opting for radical cystectomy, a maximal TURBT decreases the risk of hematuria (especially those not receiving neoadjuvant chemotherapy), and if they ultimately choose trimodality therapy, they have already had a maximal TURBT
- In patients opting for trimodality therapy, a debulking TURBT removes potentially radio- and/or chemo-resistant tumors and increases the complete response rate and survival after therapy
- Watchful waiting after TURBT and chemotherapy may be an emerging alternative strategy
Presented by: Fredrik Liedberg, MD, Skane University Hospital, Malmö, Sweden
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the European Association of Urology (EAU) 2025 Annual Meeting, Madrid, Spain, Fri, Mar 21 – Mon, Mar 24, 2025.
Related content: Complete vs Partial TURBT for Muscle-Invasive Bladder Cancer Treatment - Fredrik Liedberg, Marco Moschini & Benjamin Pradere
References:
- Graffielle V, Verhoest G, Gryn A, et al. Complete transurethral resection before radical cystectomy may improve oncological outcomes. Urol Int. 2022;106(2):122-129.
- Pak JS, Haas CR, Anderson CB, et al. Survival and oncological outcomes of complete transurethral resection of bladder tumor prior to neoadjuvant chemotherapy for muscle-invasive bladder cancer. Urol Oncol. 2021 Nov;39(11):787.e9-787.e15.
- Suer E, Hamidi N, Gokce MI, et al. Significance of second transurethral resection on patient outcomes in muscle-invasive bladder cancer patients treated with bladder-preserving multimodal therapy. World J Urol. 2016 Jun;34(6):847-851.