(UroToday.com) The 2025 EAU annual meeting featured a rapid-fire debate session on common problems and controversies in bladder cancer and a presentation by Dr. Ashish Kamat contending that for BCG unresponsive disease sequential therapies can be safely offered.
Dr. Kamat started by highlighting the changes made in the non muscle invasive bladder cancer (NMIBC) disease space from 1970 – 2018, specifically BCG’s approval in 1990 for treatment of CIS and to prevent relapse of Ta and T1 disease, the FDA’s public workshop in 2013 for clinical trial design issues for developing new therapies in NMIBC, clarification of bladder cancer disease states following treatment of patients with intravesical BCG1 in 2015, the International Bladder Cancer Group’s definitions, end points, and clinical trial designs for NMIBC in 2016,2 and the FDA’s guidance for industry of BCG-unresponsive NMIBC development of drugs and biologics for treatment:

From 2018 through 2025 and beyond, we have additional new potential therapeutics on the market including TAR-200, cretostimogene +/- pembrolizumab, and detalimogene voraplasmid: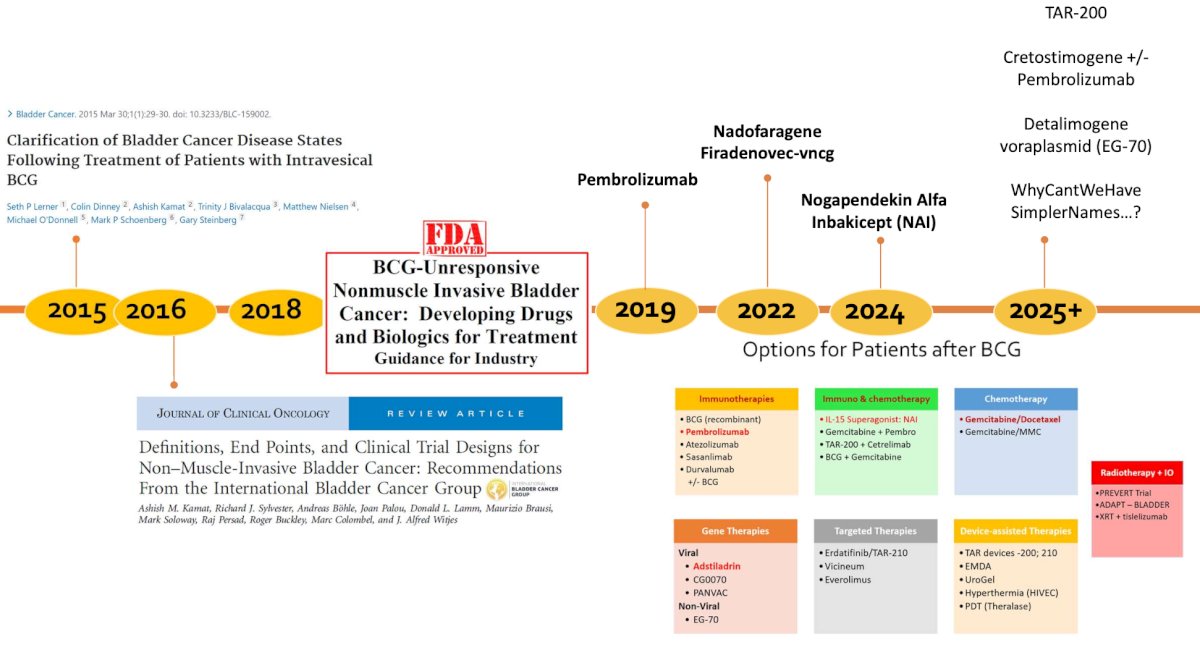
Next, Dr. Kamat discussed the International Bladder Cancer Group’s recommendations for optimal sequencing and patient selection among patients with BCG unresponsive NMIBC.3 For patients with BCG-unresponsive CIS, gemcitabine + docetaxel, nadofaragene firadenovec, and NAI + BCG are recommended; because of its systemic toxicity, pembrolizumab should only be offered after other options are exhausted. For patients with BCG-unresponsive papillary-only tumors, gemcitabine + docetaxel, nadofaragene firadenovec, NAI + BCG, single-agent chemotherapy, hyperthermic mitomycin C, and pembrolizumab are recommended: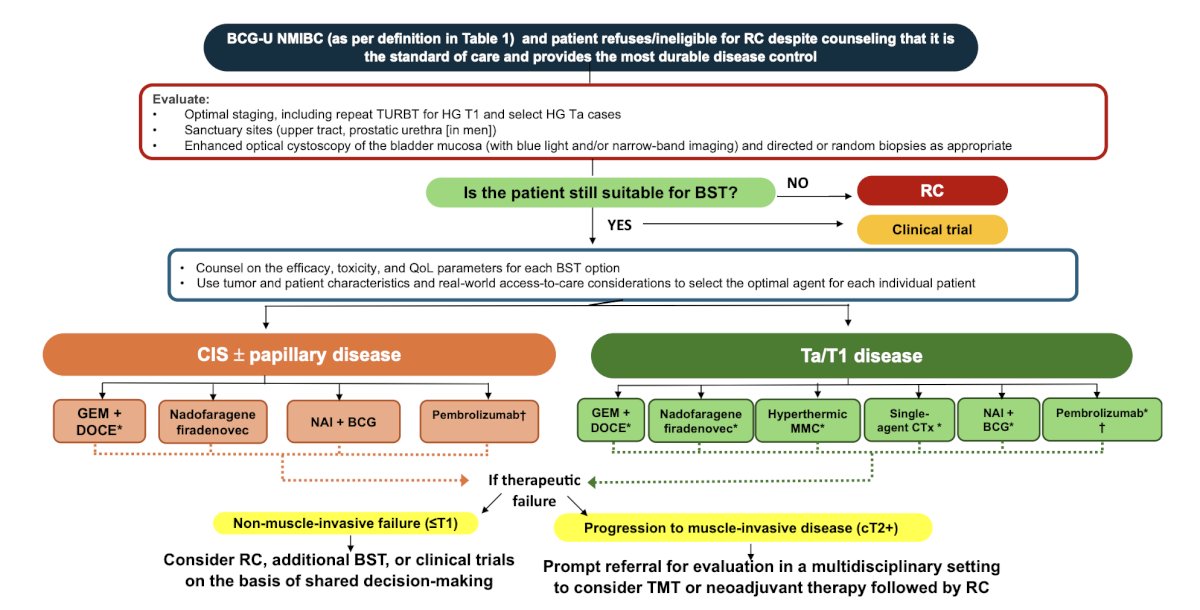
Importantly, when assessing complete response/high grade recurrence free survival at 3 and 12 months for approved and selected treatment options for BCG-unresponsive non muscle invasive bladder cancer, gemcitabine + docetaxel has impressive and durable responses for both CIS and HG Ta/T1 disease:4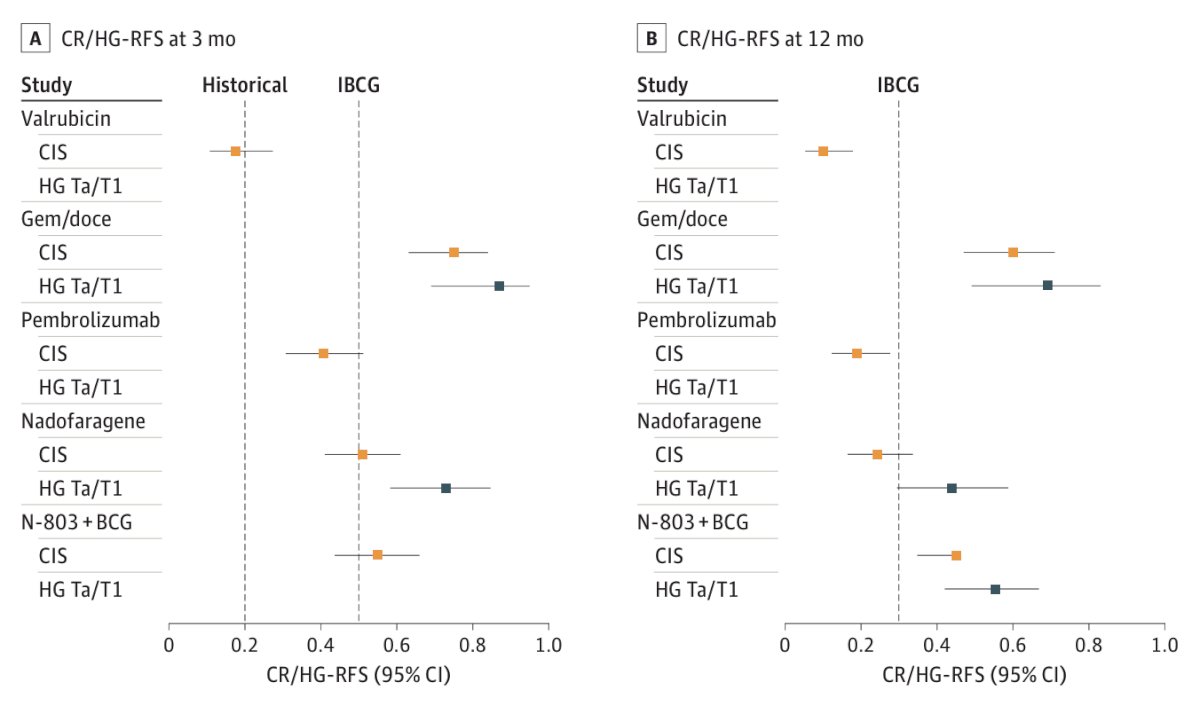
Highlighting work from his group assessing long term survival outcomes of BCG-unresponsive non muscle invasive bladder cancer treated with bladder sparing therapies,5 Dr. Kamat notes that among 114 patients, 38 underwent early radical cystectomy and 76 underwent bladder sparing treatment. There were no significant differences in overall survival (HR 1.40, 95% CI 0.68-2.89, p = 0.4) or cancer specific survival (HR 0.88, 95% CI 0.22-3.55, p = 0.9) between the two groups:![Highlighting work from his group assessing long term survival outcomes of BCG-unresponsive non muscle invasive bladder cancer treated with bladder sparing therapies [5], Dr. Kamat notes that among 114 patients, 38 underwent early radical cystectomy and 76 underwent bladder sparing treatment. There were no significant differences in overall survival (HR 1.40, 95% CI 0.68-2.89, p = 0.4) or cancer specific survival (HR 0.88, 95% CI 0.22-3.55, p = 0.9) between the two groups](/images/com-doc-importer/201-eau-2025/eau-2025-rapid-fire-debate-bcg-unresponsive-disease-how-much-risk-can-my-patient-tolerate-sequential-therapies-can-be-safely-offered/image-4.jpg)
Recently, Taylor et al.6 assessed 578 patients, of which 28% underwent upfront radical cystectomy and 72% received bladder sparing therapy. Over a median 50 months follow-up, there were no statistically significant differences in metastasis-free survival, cancer-specific survival, or overall survival between treatment groups: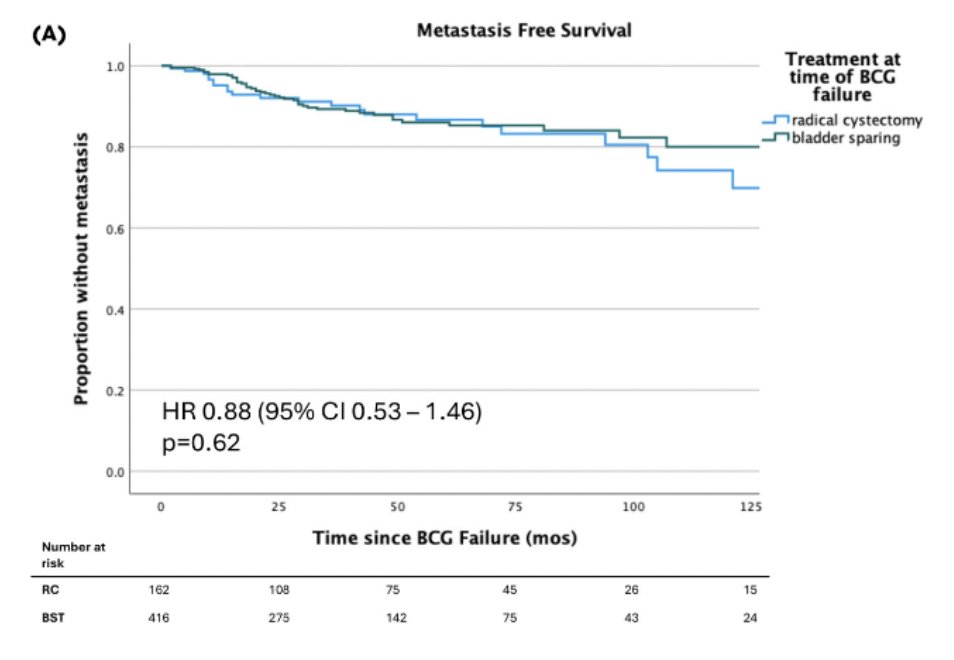
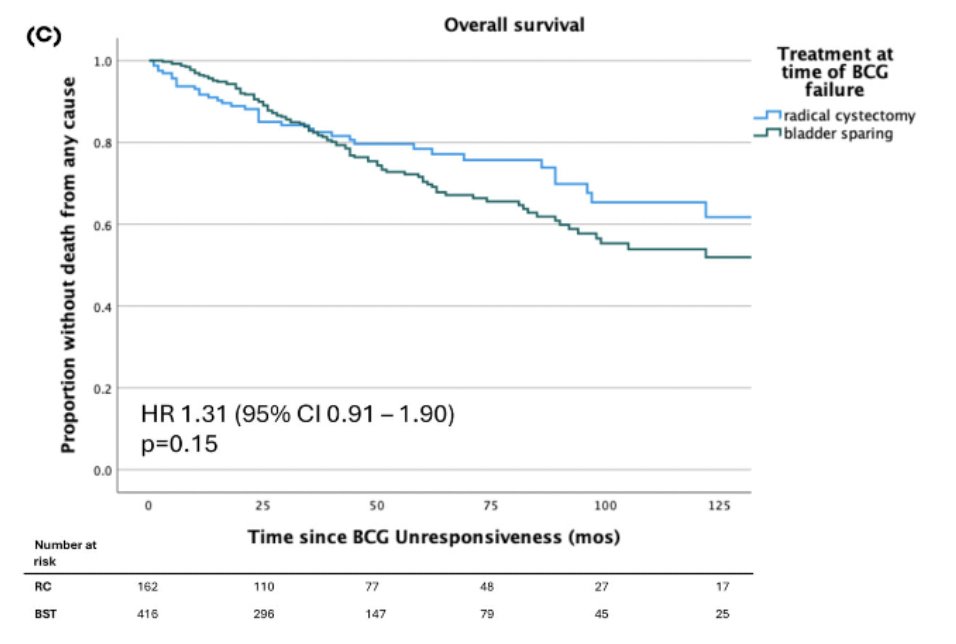
Thus, taken together, for a patient (highlighted in this debate) with HG T1a followed by 18 months of BCG, followed by a T1HG recurrence followed by gemcitabine + docetaxel, followed by 16 months of follow-up and a subsequent HG Ta recurrence, the risk of metastasis is approximately 5% and the risk of death is approximately 2%.
There are many questions that remain in this disease space from a patient’s perspective, notably “Am I giving up long term cure for short term gain?” To help alleviate anxiety for both the patient and the provider, Dr. Kamat notes that the International Bladder Cancer Group has provided the following consensus recommendations for bladder sparing therapy in BCG-unresponsive non muscle invasive bladder cancer:3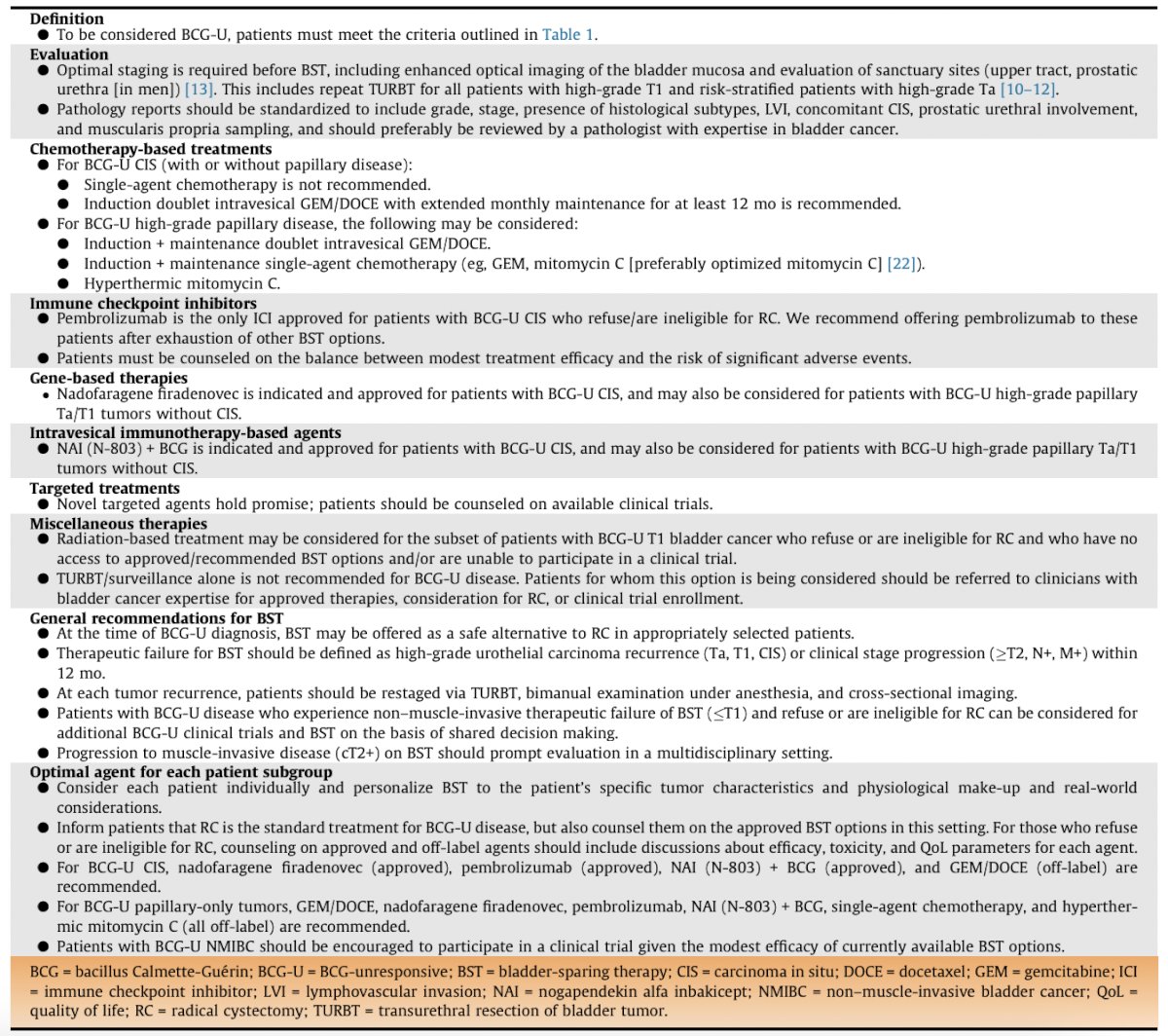
Dr. Kamat concluded his presentation discussing that for BCG unresponsive disease sequential therapies can be safely offered with the following take home points:
- “How many lines of therapy?” is the wrong question
- The question should be “Is continued therapy improving survival and quality of life, or is it delaying the inevitable at a major cost?”
- In 2025, personalized approaches with enhanced cystoscopy, appropriate imaging, biomarkers (?ctDNA), and better patient selection should drive decision making, not a fixed number of lines of therapy
Presented by: Ashish Kamat, MD, MBBS, Professor of Urology, and Wayne B. Duddleston Professor of Cancer Research, University of Texas, MD Anderson Cancer Center, Houston, TX
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the European Association of Urology (EAU) 2025 Annual Meeting, Madrid, Spain, Fri, Mar 21 – Mon, Mar 24, 2025.
Related content: Managing BCG-Unresponsive Bladder Cancer: Balancing Bladder Preservation and Cystectomy - Paolo Gontero & Maria Carmen Mir
References:
- Lerner SP, Dinney C, Kamat A, et al. Clarification of Bladder Cancer Disease States Following Treatment of Patients with Intravesical BCG. Bladder Cancer. 2015 Mar 30;1(1):29-30.
- Kamat AM, Sylvester RJ, Bohle A, et al. Definitions, End Points, and Clinical Trial Designs for Non-Muscle-Invasive Bladder Cancer: Recommendations From the International Bladder Cancer Group. J Clin Oncol. 2016 Jun 1;34(16):1935-1944.
- Li R, Hensley PJ, Gupta S, et al. Bladder-sparing therapy for Bacillus Calmette-Guerin-unresponsive non-muscle-invasive Bladder Cancer: International Bladder Cancer Group Recommendations for Optimal Sequencing and Patient Selection. Eur Urol. 2024 Aug 24;S0302-2838(24)02516-8.
- Hwang TJ, Davies BJ, Preston MA. Advancing Patient-Centered Outcomes and Equity in Clinical Trials for BCG-Unresponsive Nonmuscle Invasive Bladder Cancer. JAMA Oncol. 2023 Nov 1;9(11):1491-1492.
- Tan WS, Grajales V, Contieri R, et al. Bladder-sparing treatment in patients with Bacillus Calmette-Guerin-unresponsive non-muscle-invasive bladder cancer: An analysis of long-term survival outcomes. Eur Urol Open Sci. 2023 May 13;53:16-22.
- Taylor JI, Kamat AM, O’Donnell MA, et al. Long-term outcomes of bladder-sparing therapy vs radical cystectomy in BCG-unresponsive non-muscle-invasive bladder cancer. BJU Int. 2025 Feb;135(2):260-268.