(UroToday.com) The 2025 EAU annual meeting featured a rapid-fire debate session on common problems and controversies in bladder cancer and a presentation by Dr. M. Carmen Mir contending that for BCG unresponsive disease we should give one line of salvage therapy before proceeding to radical cystectomy. Dr. Mir started her presentation by defining BCG-unresponsive tumors as those that are BCG refractory and those that develop T1/Ta high grade recurrence within 6 months of completion of adequate BCG exposure, or develop CIS within 12 months of completion of adequate BCG exposure.
Without question, patient preference is to avoid a radical cystectomy, given that 89% of patients prefer a medical therapy over immediate radical cystectomy.1 Moreover, preferences were most affected by time to radical cystectomy (relative attribute importance: 55%), followed by risk of progressing to muscle invasive bladder cancer (relative attribute importance: 25%), medication administration (relative attribute importance: 12%), and the risk of serious side effects (relative attribute importance: 8%). Patients were willing to accept a 43.8% higher risk of progression to delay a radical cystectomy by 5 years, and a 66.1% higher risk of side effects in order to delay a radical cystectomy. But, how much risk are our patients/we willing to take to keep their bladder?
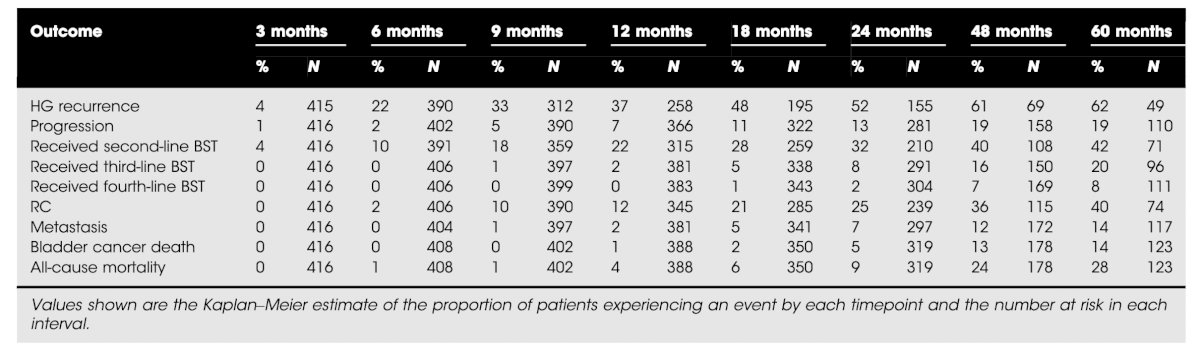
Dr. Mir notes that there is declining efficacy with additional salvage therapies. Recently, Taylor et al.2 assessed 578 patients, of which 28% underwent upfront radical cystectomy and 72% received bladder sparing therapy. Over a median 50 months follow-up, there were no statistically significant differences in metastasis-free survival, cancer-specific survival, or overall survival between treatment groups. Of note, 50% had additional BCG as their bladder sparing therapy. As follows is an outcomes summary of patients undergoing initial bladder sparing therapy:
Dr. Mir also noted that among available bladder sparing therapies, there is limited long term benefit. For example, in KEYNOTE-0573,4 53% underwent salvage therapies and 50% eventually underwent radical cystectomy. In the SWOG 1605 trial of atezolizumab, the complete response rate at 6 months was 27%, but 7 patients had muscle invasive bladder cancer, 6 of which were non-complete responders. For IL-15 NAI,5 initial complete response rate was 71%, 54% had a complete response in the reinduction group, and 7 underwent radical cystectomy (all with non muscle invasive bladder cancer). Overall, 30/43 (70%) had prior BCG + other therapies.
Previous work has demonstrated that progressive muscle invasive bladder cancer is worse than primary muscle invasive bladder cancer, with regards to recurrence free, cancer specific and overall survival. Dr. Mir highlighted the following summary of risk of disease progression in initial non-responders from the key BCG unresponsive non muscle invasive bladder cancer trials:

With regard to toxicity and patient burden, bladder sparing therapy implies frequent cystoscopies, toxicity related to drug administration, and worry about progression. Upfront radical cystectomy may not significantly worsen quality of life. The CISTO trial is assessing a comparison of intravesical therapy and surgery as treatment options for bladder cancer and will help further define some of these questions.
Dr. Mir’s final point was regarding the clinical guidelines and regulations. The EAU guidelines provide a strong recommendation for offering a radical cystectomy to patients with BCG unresponsive bladder cancer, and a weak recommendation for offering patients with BCG unresponsive bladder cancer, who are not candidates for radical cystectomy due to comorbidities, preservation strategies (intravesical chemotherapy, chemotherapy and microwave-induced hyperthermia, electromotive administration of chemotherapy, intravesical- or systemic immunotherapy, preferably within a clinical trial).
Dr. Mir concluded her presentation by discussing that for BCG unresponsive disease we should give one line of salvage therapy before proceeding to radical cystectomy with the following take home points:
- Multi-disciplinary discussion is essential to evaluate further lines of bladder sparing therapies
- Over 50% of patients will ultimately undergo radical cystectomy, so are we avoiding or delaying radical cystectomy?
- It is important to differentiate initial responders to first line from initial non-responders (progression risk increases by further lines of therapy)
- There is a need for better prediction tools of progression (ie. biomarkers, imaging, artificial intelligence tools)
- The key is patient counseling on the risks and benefits, in order to have individualized patient decision making
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the European Association of Urology (EAU) 2025 Annual Meeting, Madrid, Spain, Fri, Mar 21 – Mon, Mar 24, 2025.
References:
- Collacott H, Krucien N, Heidenreich S, et al. Patient preferences for treatment of Bacillus Calmette-Guerin-unresponsive non-muscle-invasive bladder cancer: A cross-country choice experiment. Eur Urol Open Sci. 2023 Jan 31:49:92-99.
- Taylor JI, Kamat AM, O’Donnell MA, et al. Long-term outcomes of bladder-sparing therapy vs radical cystectomy in BCG-unresponsive non-muscle-invasive bladder cancer. BJU Int. 2025 Feb;135(2):260-268.
- Balar AV, Kamat AM, Kulkarni GS, et al. Pembrolizumab monotherapy for the treatment of high-risk non-muscle-invasive bladder cancer unresponsive to BCG (KEYNOTE-057): An open-label, single-arm, multicenter, phase 2 study. Lancet Oncol. 2021 Jul;22(7):919-930.
- Necchi A, Roumiguié M, Kamat AM, et al. Pembrolizumab monotherapy for high-risk non-muscle-invasive bladder cancer without carcinoma in situ and unresponsive to BCG (KEYNOTE-057): a single-arm, multicentre, phase 2 trial. Lancet Oncol. 2024 Jun;25(6):720-730.
- Chamie K, Chang SS, Kramolowsky E, et al. IL-15 Superagonist NAI in BCG-Unresponsive Non-Muscle-Invasive Bladder Cancer. NEJM Evid 2022; 2(1)