(UroToday.com) The 2025 EAU annual meeting featured a rapid-fire debate session on common problems and controversies in bladder cancer and a presentation by Dr. Laura Mertens contending that for high risk non muscle invasive bladder cancer, it is time to dethrone BCG. Dr. Mertens started by making the point that BCG is not bad, in fact, a recent European Urology Oncology review article1 suggest that among 12 studies, the 5 year recurrence free survival rate is 39-66% and the 5 year progression free survival rate is 70-84%. However, Dr. Mertens states that BCG must be better than its current efficacy.
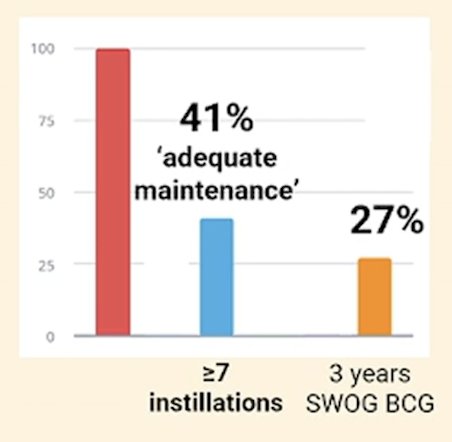
Notably, the duration of recommended BCG treatment is not feasible. According to the EAU guidelines, for EAU high risk patients, there is a strong recommendation for offering full dose BCG instillations for one to three years, and that three year maintenance is more effective than one year to prevent recurrence in patients with high risk tumors. Only ~27% of patients complete 3 years of SWOG recommended maintenance BCG and only 41% of patients receive ‘adequate maintenance’ defined as 7+ instillations of BCG:
Serious toxicity is also possible with prolonged BCG courses, with local BCG related toxicity estimated to be 63% and systemic BCG-related toxicity estimated to be 32%. Rare, but severe, complications such as aortoesophageal fistulae have also been reported.
Despite 5 year recurrence free survival rates of 39-66% and the 5 year progression free survival rates of 70-84% [1], BCG is not effective for all high risk non muscle invasive bladder cancer. We need tools to predict those who are unlikely to respond to BCG (and look for alternatives) and to monitor treatment response to be able to adjust the dose and duration of treatment. Many alternatives to BCG exist, including intravesical chemohyperthermia with mitomycin C, which is approved in Europe. Other novel options include the immunomodulator RUTI (presented at ESMO 2024), the trifunctional anti-EpCAM/CD3 bite-specific antibody catumaxomab (presented at ESMO 2024), and disitamab vedotin for patients with tumor HER2 expression (presented at ASCO GU 2025).
Dr. Mertens concluded her presentation by discussing that in 2025 it is time to dethrone BCG for high risk non muscle invasive bladder cancer with the following take home points:
- BCG has been the cornerstone treatment of patients with high risk non muscle invasive bladder cancer, but ‘not bad’ is not equivalent to ‘good enough’
- There is a need to optimize patient selection, dose and duration, and combination with novel agents to achieve superior outcomes
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the European Association of Urology (EAU) 2025 Annual Meeting, Madrid, Spain, Fri, Mar 21 – Mon, Mar 24, 2025.
References:
- Longoni M, Scilpoti P, Sona F, et al. Oncological outcomes in BCG-naïve high-risk non muscle invasive bladder cancer patients: A systematic review on current treatment strategies and future perspectives. Eur Urol Oncol. [in press].