(UroToday.com) The Bladder Cancer Advocacy Network (BCAN) Bladder Cancer Think Tank 2025, held in Washington D.C., United States, was host to the session: Navigating Financial Toxicity in Bladder Cancer. Dr Parminder Singh, Dr. Matthew Mossanen, and Dr. Ruchika Talwar co-chaired the session Balancing Innovation and Affordability: Collaborative Pathways in Bladder Cancer Care.
Dr. Mossanen opened by emphasizing the significant economic burden associated with bladder cancer care. He noted that bladder cancer is one of the most expensive cancers to treat, with high direct costs that also lead to substantial indirect costs. These indirect impacts include patient anxiety over care-related expenses, stress about treatment decisions, lost workdays, caregiver strain, lifestyle changes, and an overall decline in quality of life, collectively contributing to what is termed "financial toxicity."
In the United States, up to 75% of bankruptcies are due to medical expenses. Around 40% of cancer patients report financial hardship, and in bladder cancer specifically, up to 1 in 4 patients experience financial toxicity. These individuals are more likely to delay care and report poorer mental and physical health. He emphasized the importance of mindful conversations between clinicians and patients, focusing on the patient, prognosis, and treatment plan.
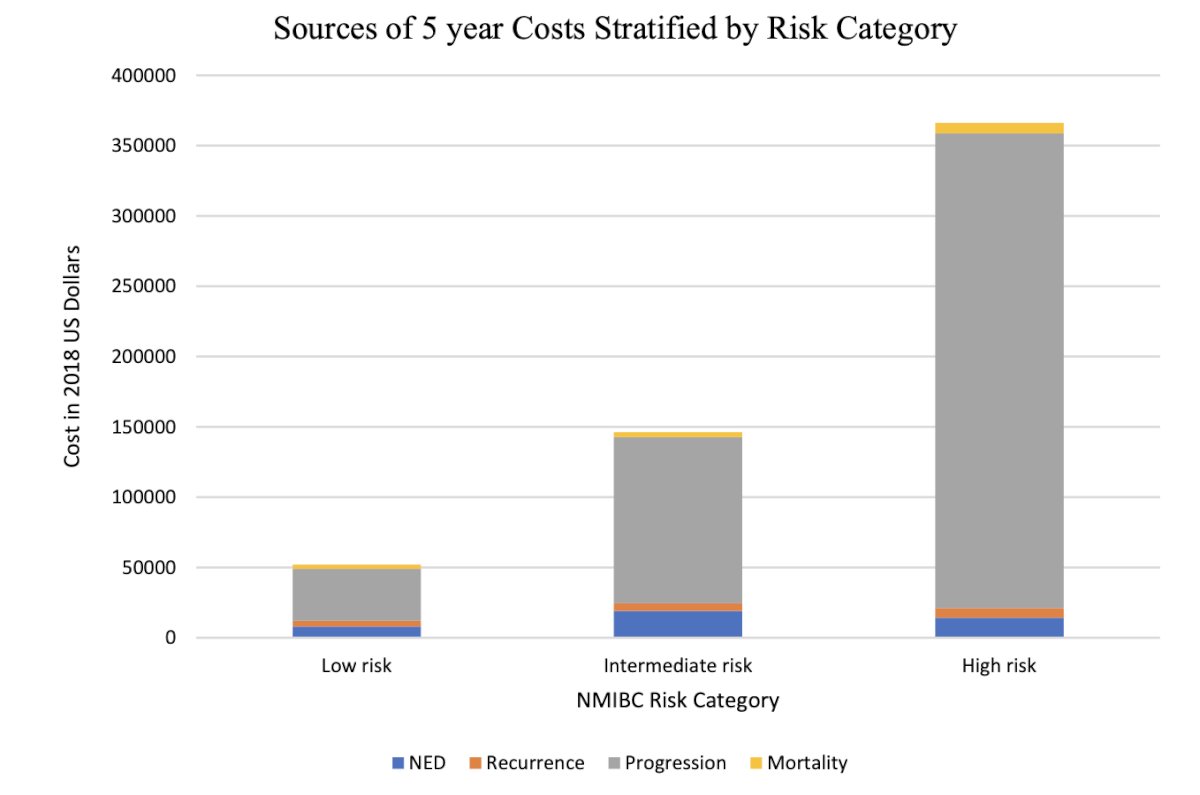
Dr. Mossanen emphasized that current models used to study the cost of bladder cancer care have limitations. He referenced a study that developed various models to estimate surveillance costs for non–muscle-invasive bladder cancer, noting that estimates vary by risk category, for example, $52,125 for low-risk disease versus $366,143 for high-risk disease. Each disease state is dynamic, and patients may shift between categories due to progression. Additionally, these models risk becoming outdated as treatment costs and care options evolve over time.1
We must consider multiple perspectives when addressing the cost of bladder cancer care. From the patient and physician standpoint, informed decision-making requires transparency around the financial implications of treatment. Public health systems play a role in shaping policy to ensure equitable access. If therapies are too expensive, patients may skip doses, jeopardizing outcomes. Economic factors also matter; rising drug prices can drive up insurance premiums and influence which treatments hospitals choose to stock and offer. Ultimately, the goal is to align therapeutic decisions with clinical benefit, affordability, and system-wide sustainability.
Dr. Mossanen concluded by acknowledging that the problem of financial toxicity in bladder cancer care is likely to persist, especially as new and novel therapies continue to emerge across all disease stages. He emphasized the urgent need to engage in open dialogue about the cost of care and to collaborate across disciplines, clinicians, policymakers, economists, and patient advocates to develop sustainable solutions that ensure both access and equity.
Evolving paradigm of Bladder cancer treatment in Non-Muscle Invasive and Muscle Invasive Bladder Cancer and Financial Implications – Parminder SinghDr. Singh highlighted the timeline of FDA approvals in bladder cancer highlights the expanding treatment landscape, from early agents like Thiotepa (1959) and BCG (1990) to more recent and costly innovations such as pembrolizumab (2020), nadofaragene (2022), and N-803 (2024). This rapid expansion of novel and targeted therapies, while beneficial, also contributes to the rising cost of care, emphasizing the need for ongoing discussions around financial impact and healthcare resource allocation.
Dr. Singh shared the pipeline of anticipated approvals for BCG-naïve, BCG-recurrent, and BCG-unresponsive bladder cancer, highlighting the large number of trials expected to read out between 2025 and 2028. This underscores the rapid pace of therapeutic development and the need to prepare for its clinical and financial implications.
These therapies for BCG-unresponsive NMIBC show varying durations of response, with median durations ranging from 9.7 months (Adstiladrin) to over 28 months (Cretostimogene grenadenorepvec). Pembrolizumab and NAI also demonstrate durable benefit in subsets of patients. However, as median durations of response (mDOR) extend and patients remain on therapy for longer periods, this will likely translate into significantly increased treatment costs over time.
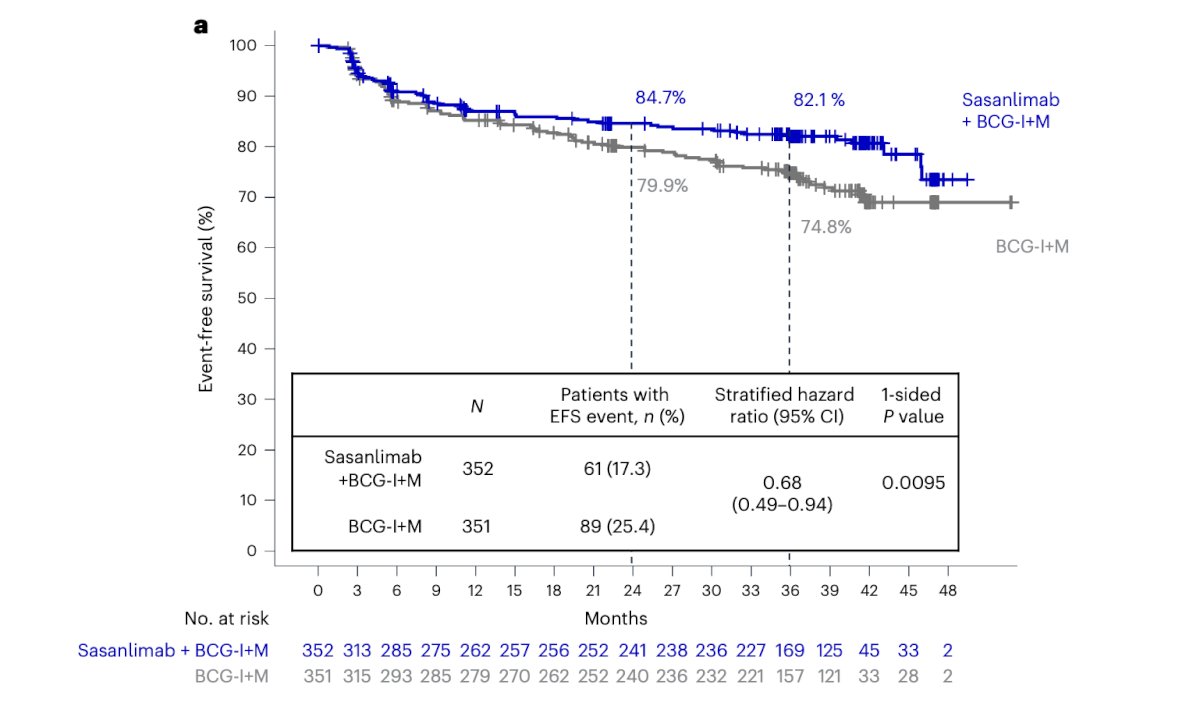
The randomized phase 3 CREST trial evaluated sasanlimab plus BCG in BCG-naive, high-risk non–muscle-invasive bladder cancer (NMIBC). The combination significantly improved event-free survival (EFS), with 84.7% and 82.1% EFS at 24 and 36 months, respectively. While effective, this regimen adds treatment burden, as patients must return for frequent intravesical or systemic therapies, contributing further to cost and logistical challenges in care delivery.2
The rising cost of bladder cancer care is becoming a growing concern due to the increasing availability of novel and often expensive therapies. A comparison of estimated treatment costs reveals a steep financial burden: while BCG remains relatively low in cost (4,587 USD), N-803 (~$1.15M for 30 cycles), and especially CG0070 (Cretostimogene grenadenorepvec), which may exceed $2.1M for 36 cycles, contribute significantly to the overall cost. As more therapies are approved and longer durations of response are achieved, the cumulative burden to patients and health systems will escalate.3
The treatment landscape for locally advanced and metastatic urothelial carcinoma (la/mUC) has rapidly evolved, with a notable acceleration in FDA approvals since 2016. The introduction of immunotherapies such as atezolizumab, nivolumab, and avelumab, along with targeted agents like erdafitinib and enfortumab vedotin, has significantly broadened therapeutic options and costs. This momentum continues with anticipated approvals of novel combinations like nivolumab plus gemcitabine and cisplatin in 2024. These advances highlight the increasing complexity and financial burden in both BCG-unresponsive and la/mUC settings.
Dr. Singh highlighted the EV-302 trial and its significant impact on improving overall survival for patients with urothelial carcinoma. He emphasized how therapies like enfortumab vedotin (OS curves shown below) have transformed the treatment landscape, leading to better outcomes, durable remissions, and longer durations on therapy, underscoring the progress made in recent years and the growing potential for sustained disease control and longer durations of response.4

Dr. Louie outlined the challenges of drug development from the sponsor’s perspective, describing it as a lengthy, risky, and expensive process. He noted that the average timeline from discovery to approval is 10–12 years, with fewer than 10% of drugs entering Phase 1 ultimately gaining regulatory approval. The financial burden is substantial, with direct “out-of-pocket” sponsor costs estimated at $1.4 billion, and indirect costs (including failed drug programs) reaching $2.6 billion. Oncology, in particular, has one of the lowest success rates (3–5%) and the highest costs, making it one of the most complex and resource-intensive therapeutic areas.
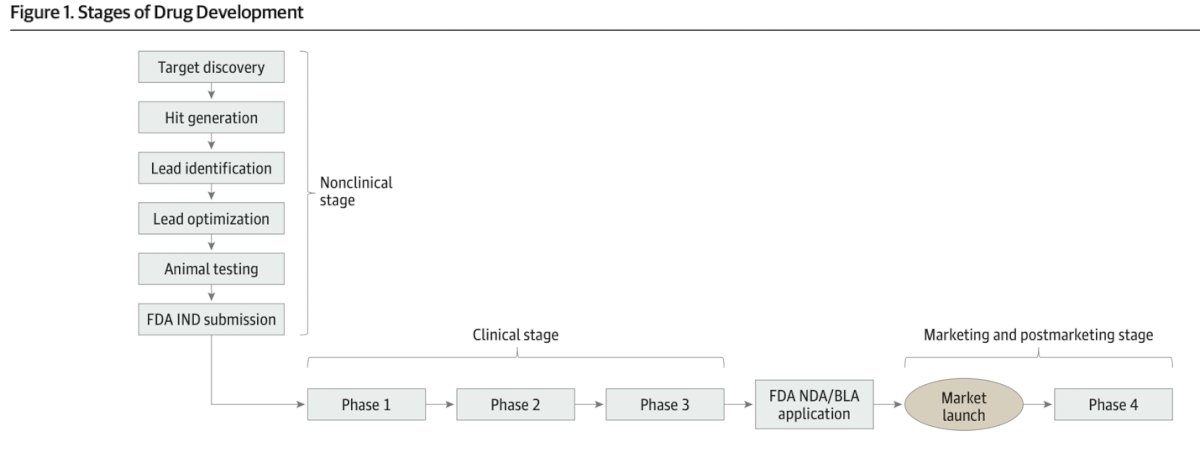
The drug development process begins with the nonclinical stage, which includes target discovery, hit generation, lead identification, lead optimization, and animal testing. After these steps, a sponsor submits an Investigational New Drug (IND) application to the FDA. Upon approval, the drug enters the clinical stage, consisting of Phase 1 (safety and dosage), Phase 2 (efficacy and side effects), and Phase 3 (confirmation of effectiveness, monitoring of side effects, comparison to commonly used treatments). Following successful clinical trials, a New Drug Application (NDA) or Biologic License Application (BLA) is submitted to the FDA. If approved, the drug proceeds to market launch and enters Phase 4, the post-marketing stage, which involves continued safety monitoring and long-term effectiveness assessments as illustrated below.5
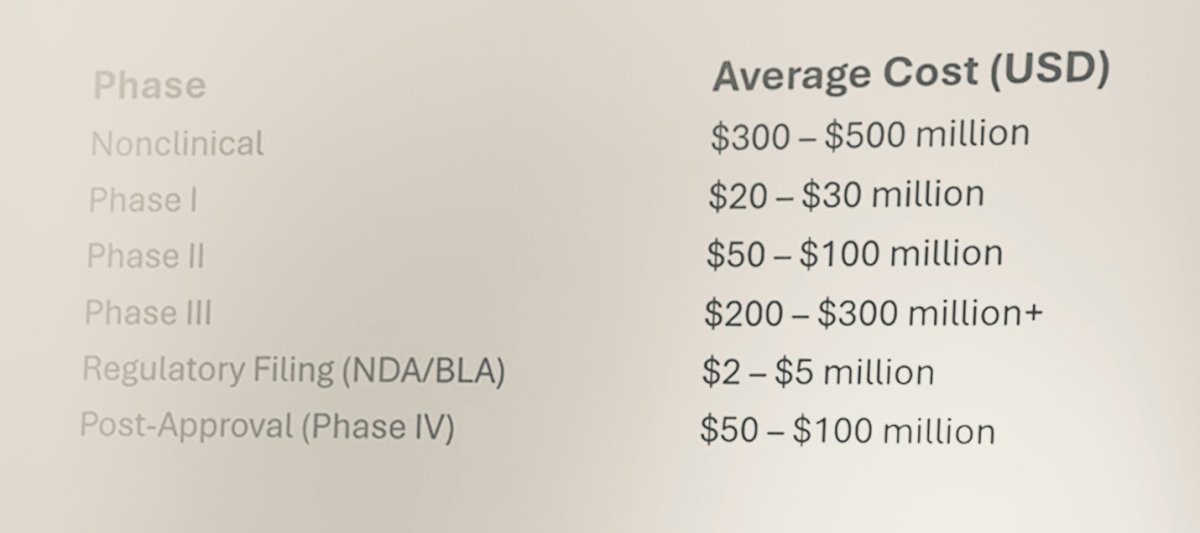
The average cost of drug development varies by phase, with Phase III being the most expensive, typically ranging from $200 to $300 million or more. Nonclinical development also represents a significant investment at $300–$500 million. A summary of the average cost for each Phase is presented below.
The largest reason for drug development failure is lack of efficacy, accounting for 57% of cases and typically becoming evident only during Phase II or III trials. Other contributing factors include safety or toxicity concerns (17%), commercial reasons (15%), and poor pharmacokinetics or bioavailability (8%). Ideally, failures should occur earlier in development during preclinical or Phase I stages to help reduce financial losses and resource expenditure.
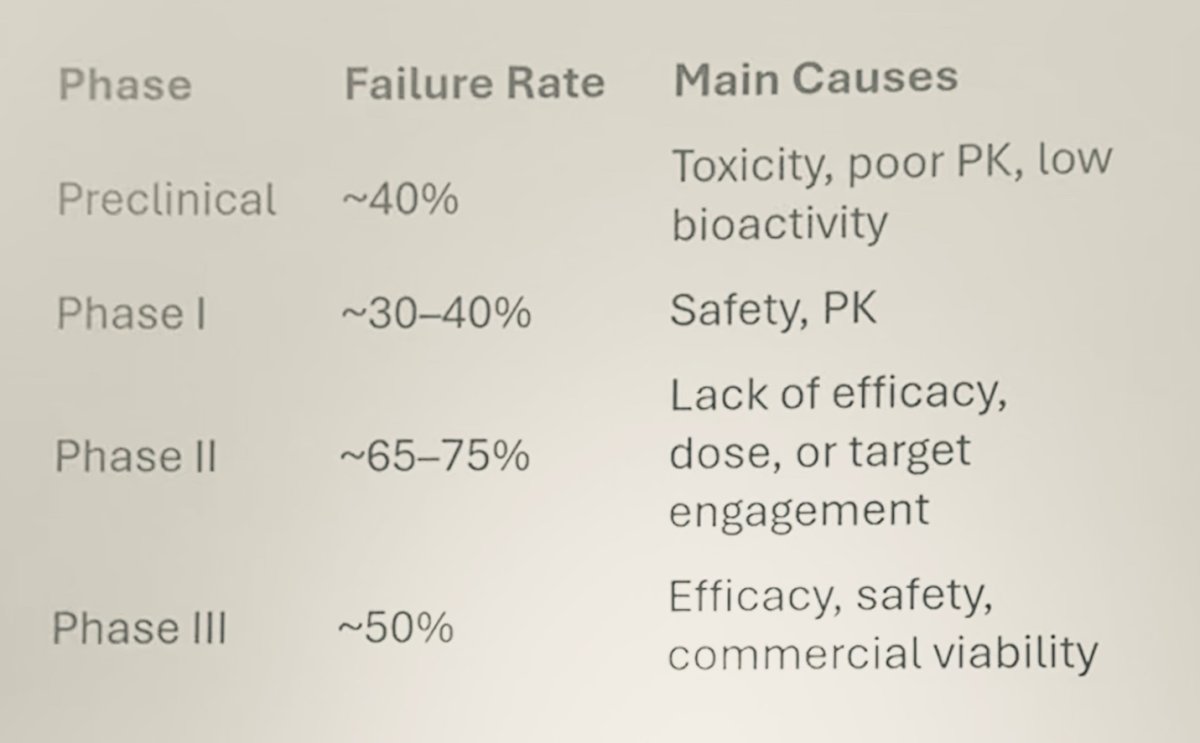
Dr. Louie highlighted that the failure rate across drug development stages remains high. In the preclinical stage, a substantial proportion of drugs fail due to toxicity, poor pharmacokinetics, or low bioactivity. During Phase I, failures often result from safety concerns or suboptimal PK. Phase II, which focuses on efficacy and dose optimization, sees the highest attrition, primarily because of insufficient efficacy or lack of adequate target engagement. Even in Phase III, where drugs are tested in larger populations, about half still fail, typically due to challenges with efficacy, safety, or commercial viability. This is illustrated in detail in the figure below.
Lastly, Dr. Louie emphasized the potential of artificial intelligence (AI) to enhance and accelerate the drug development process. AI can assist in identifying novel therapeutic targets, rapidly screen thousands of drug candidates, and streamline the early stages of development. Furthermore, AI tools can improve the efficiency and speed of clinical trial design and execution, potentially reducing time to approval and overall development costs.
Mr. Toner explained that once a drug price is established, the revenue strategy and budget teams begin determining how to manage it. He highlighted that transformative therapies, while potentially altering the entire trajectory of a disease, come at a significant cost, positioned somewhere between traditional drugs and solid organ transplantation in terms of financial burden.
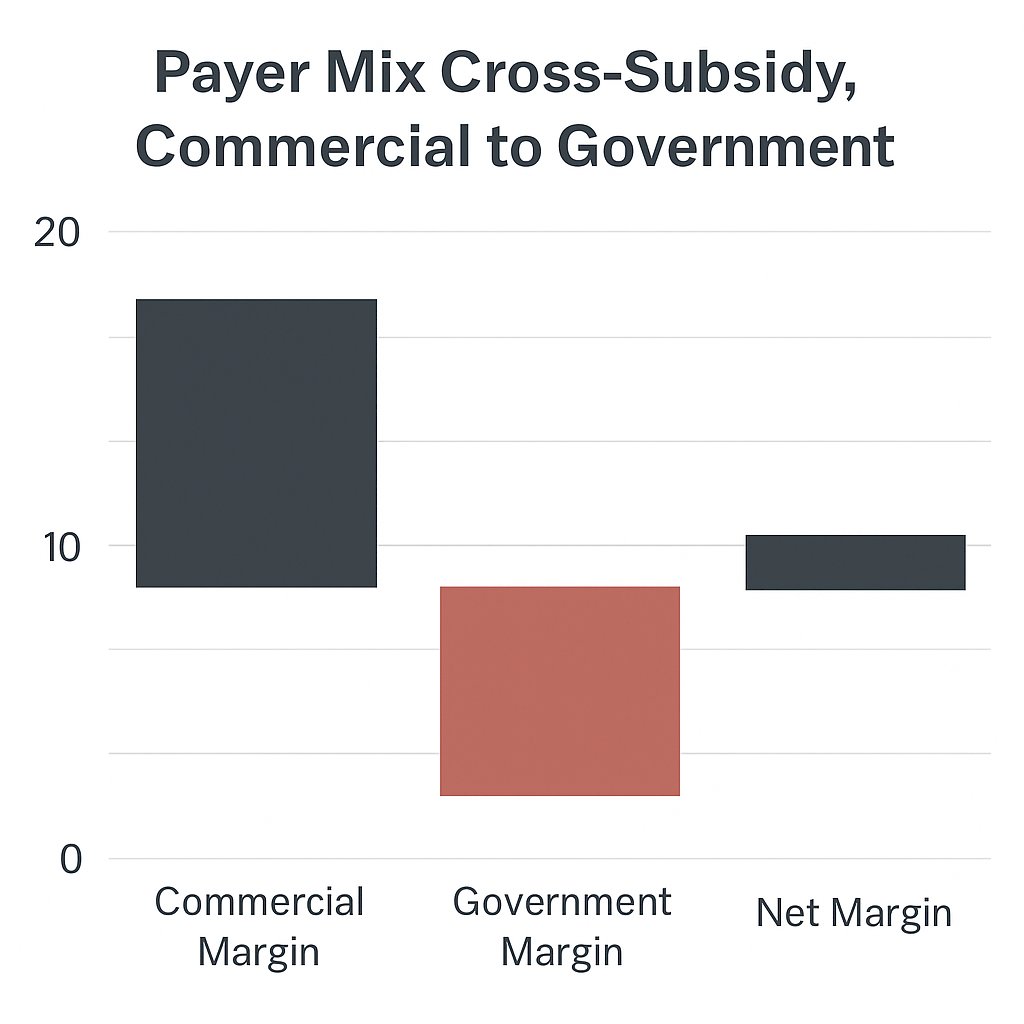
In the U.S., access to care is shaped by two entrenched cross-subsidization mechanisms often referred to as the “ugly pillars” of healthcare financing. These structures weren’t designed intentionally and are widely criticized, yet they persist. Mr. Toner illustrated this through two key examples. First, the payer mix cross-subsidy compares reimbursements from commercial insurers versus government payers, where commercial payers contribute above the cost of care (black bar), while government programs pay less (red bar), creating a widening net margin imbalance. Second, drug-to-service cross-subsidization shows that revenue from drug margins offsets deficits from underpaid physician services, such as office visits. However, these existing financial workarounds are ill-equipped to support the high upfront costs of emerging cell and gene therapies, making sustainable access to innovation increasingly challenging without systemic reform.
Mr. Toner explained that the drug product margin effectively cross-subsidizes other components of the healthcare delivery system, including physician salaries, clinical infrastructure, and office operations. When a new therapy is being considered for adoption, especially transformative ones with high cost, the revenue and strategy teams must evaluate whether the reimbursement dynamics (as reflected in the margin charts) make sense within the existing care model. Because of the complexity and magnitude of these changes, it takes time to align stakeholders across departments, emphasizing the importance of proactive financial planning when introducing novel therapies.
Moreover, transformative therapeutics, such as cell and gene therapies, require a more complex and multidisciplinary onboarding process compared to traditional formulary approvals. Because each product varies in complexity and delivery requirements, systems must coordinate across a range of stakeholders while avoiding bureaucratic delays and redundancy. The approach proposed involves assembling a Transformative Therapeutics Enterprise Team composed of product- or class-specific groups (e.g., for sickle cell, hemophilia, or T cell receptor therapies). These groups include clinical and research champions, formulary and specialty representatives, pharmacy and supply chain staff, financial planners, legal and ethics advisors, and contracting leads.
This enterprise team works with both regional and enterprise-level C-suite and practice leadership to guide new therapies from pre-FDA stages through to formulary approval, ensuring alignment with consensus-based guidelines and restrictions. The model aims to streamline coordination while balancing innovation with operational and financial feasibility.
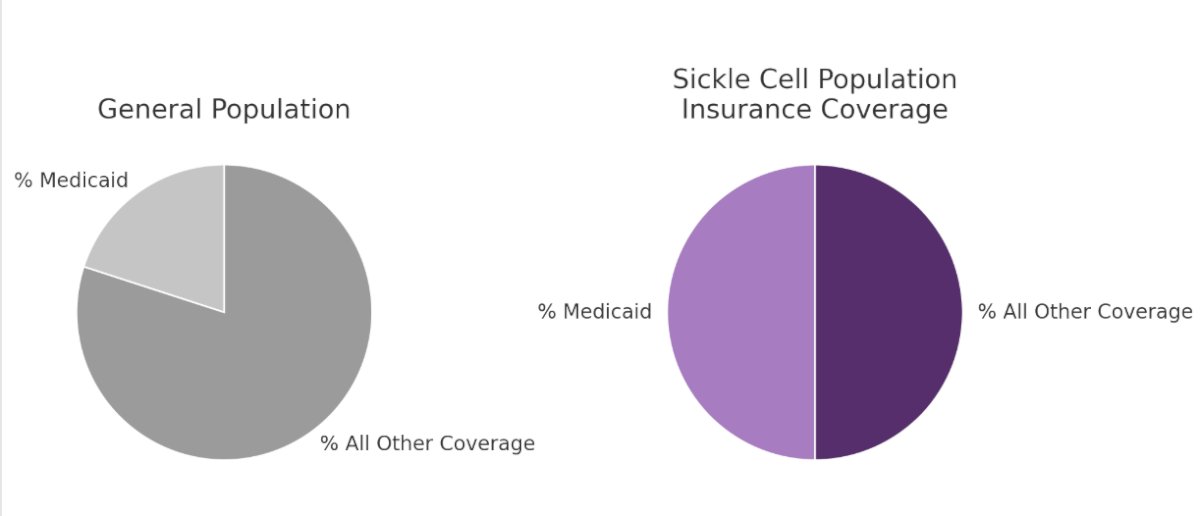
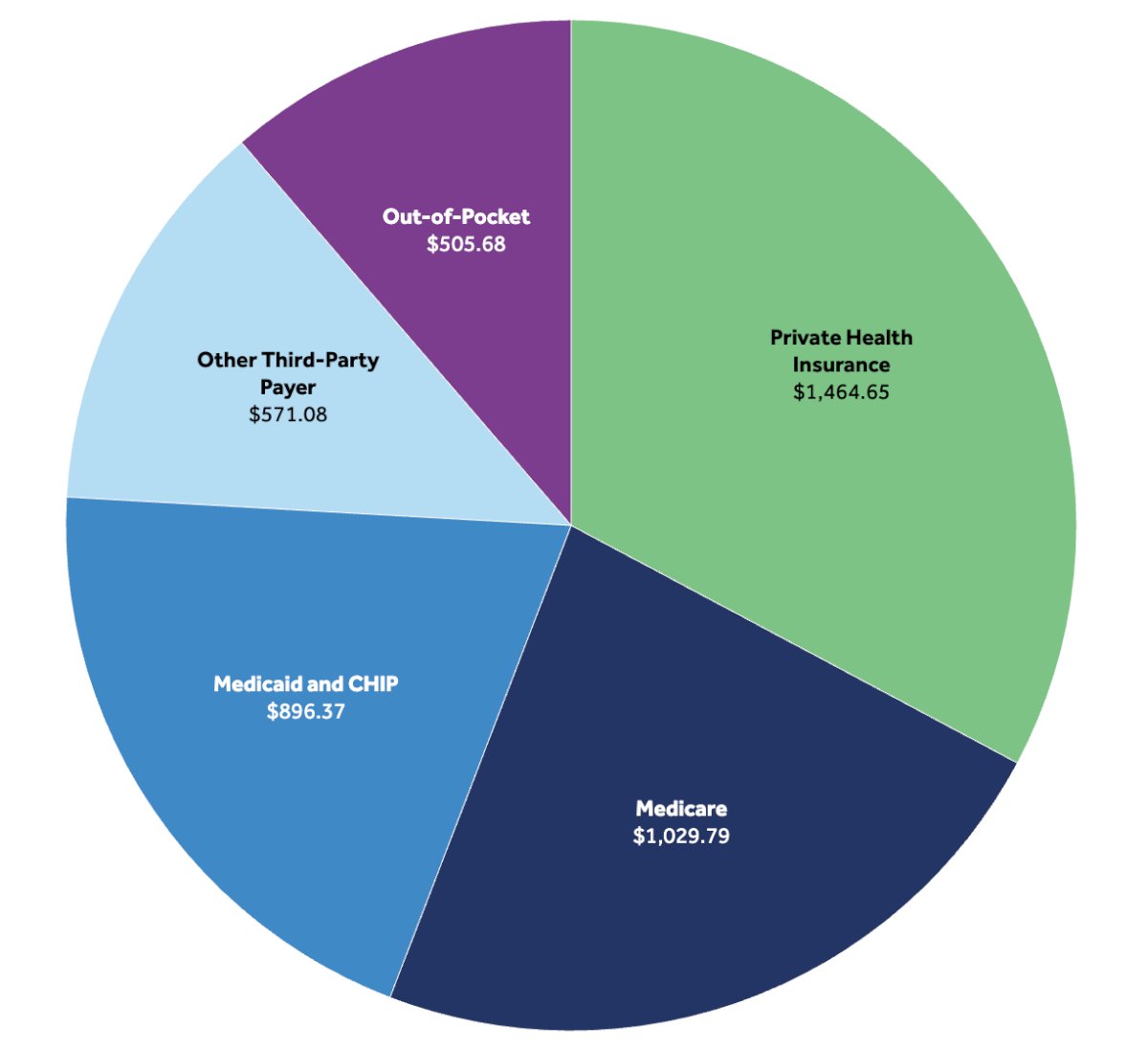
Mr. Toner discussed that therapies for sickle cell disease are disproportionately covered by state-sponsored Medicaid. This creates a major challenge for the payer mix cross-subsidy model, which normally relies on commercial payers to offset government under-reimbursement. The left pie chart shows that, in the general population, Medicaid represents a smaller fraction of coverage, whereas the right chart demonstrates that a much larger proportion of sickle cell patients are Medicaid-insured. This mismatch prevents the usual financial balancing mechanism from functioning effectively for these therapies.
Lastly, even when commercial payers are involved, hospitals typically receive only the invoice cost, also referred to as “pass-through” reimbursement for cell and gene therapy products. As a result, there is no profit margin on the product itself, since these therapies are already extremely expensive. This effectively prevents the second access cross-subsidy (from drug margin to physician services) from functioning. In this context, the traditional cross-subsidy model breaks down, creating financial challenges for providers seeking to deliver transformative therapies.
The Payer’s perspective - Stephanie SpenceA pharmacist working within a health plan plays a key role in managing high-cost drugs by monitoring spending trends and identifying unexpected spikes. With the emergence of gene therapies some carrying price tags as high as $2.3 million for a single treatment, these pharmacists must develop creative strategies to anticipate and mitigate financial risks.
Specialty drugs, typically defined as those costing over $600 for a 30-day supply, are increasingly common and often require complex handling. For instance, Krystexxa, a treatment for gout, is priced around $20,000 per dose, administered twice monthly, totaling 24 times per year. These medications fall under the purview of specialty pharmacy, a domain that demands credentialed and certified specialist pharmacists to manage logistics, patient education, and access. These services extend far beyond what’s available at a standard neighborhood pharmacy.
Drugs may be sourced either through wholesalers or directly from manufacturers, depending on the therapy. In the case of gene therapies, such as one for hemophilia manufactured in Germany, the cost includes not just the product itself but also the logistics of flying it to the United States. For example, a gene therapy with a $3 million price tag undergoes a thorough internal review. These treatments often address unmet needs in small patient populations, making their financial impact more concentrated but still significant. Health plans closely monitor how such drugs are being requested, including whether use is aligned with approved indications (on-label) or extends beyond them (off-label).
In the context of utilization management, prior authorizations are typically the first mechanism employed to control access to high-cost therapies. Another key strategy involves site-of-care management. Moreover, the cost of a drug can vary significantly depending on where it is administered. The price is influenced by negotiated contracts between payers and providers, and these rates can differ substantially across regions. For example, the cost of administering a drug in Florida may differ from that in Washington, DC, highlighting the geographic variability in reimbursement structures.
Lastly, Ms. Spence highlighted the importance of site-of-care programs, which aim to steer drug utilization toward specific settings such as outpatient facilities or provider offices that may offer more cost-effective care. She also described emerging risk management models, where manufacturers acknowledging the high costs of drug development may price therapies with built-in warranties tied to clinical efficacy. These models are designed to share financial risk and reinforce value-based care.
Advocating for Affordable Bladder Cancer Care - Ruchika TalwarDr. Talwar began by noting that financial toxicity is a combination of two key components: financial burden and financial distress. Financial burden refers to objective, out-of-pocket costs borne by patients, including payments to doctors, hospitals, and pharmacies, as well as co-payments, co-insurance, and deductibles. In contrast, financial distress represents the indirect, subjective impact of this burden, encompassing factors such as travel time, lost wages, decreased work productivity, early retirement, the toll on loved ones, and emotional stress or anxiety. Together, these elements underscore how the tangible expenses and the intangible emotional consequences compound to create significant financial strain for cancer patients.
Notably, while less than 20% of physicians can accurately estimate a patient's out-of-pocket costs, 90% of patients over the age of 65 want their physicians to provide this information. However, significant barriers exist, the major one being the complexity and opacity of the healthcare payment system, where no two patients typically pay the same amount due to variations in insurance coverage, negotiated rates, and benefit structures. This disconnect between patient expectations and provider capabilities contributes to the challenge of addressing financial toxicity in clinical care.
In 2023, the U.S. health system crossed a staggering $4.8 trillion in total spending, and projections show that by 2032, we could be looking at $7.7 trillion, nearly a fifth of the nation’s GDP. These numbers aren't just abstract; they reflect the massive financial pressure that care delivery systems are under. A closer look at who’s footing the bill reveals a steady expansion in the role of government-sponsored insurance, including Medicare and Medicaid, which together now make up nearly half of all healthcare expenditures.
With this backdrop, it’s no surprise that policymakers are zeroing in on healthcare as a prime area for cost containment. From Medicaid reductions to sweeping changes in pharmaceutical pricing, there’s a clear push to rein in spending, and for those of us working in cancer care, this evolving environment demands we rethink how therapies are delivered, reimbursed, and accessed, especially as more high-cost innovations come online.
Dr. Talwar highlighted a recent Executive Order aimed at slashing pharmaceutical costs by 59%, though the pathway to achieving that number remains unclear. She pointed out this isn’t the first time a presidential administration has tried to take on drug pricing, referencing Trump’s direct outreach to pharma CEOs, demanding tangible reductions. Several provisions are now being proposed: requiring Medicaid to pay no more than the lowest global price for a given drug, applying “most favored nation” pricing standards to pipeline therapies (particularly relevant for high-cost agents in bladder cancer), and mandating that drug manufacturers repatriate overseas revenues. Perhaps most striking is the proposal to allow direct-to-consumer drug sales at those same benchmark prices. While ambitious, the implementation details remain vague, and the potential impact on access, innovation, and the U.S. pharma market will depend on how aggressively these ideas are enforced.
However, Dr. Talwar emphasized a critical nuance often missed in the pricing debate: the reason other countries pay less than the U.S. is that they negotiate aggressively, setting caps on what they’ll pay, sometimes below the cost of development. When that happens, pharmaceutical companies rely on U.S. pricing to recoup losses and generate a net profit. This system, she argued, effectively places the financial burden of global R&D on the American healthcare system. So, while “most favored nation” pricing sounds fair on paper, it doesn’t reflect the full economic reality, especially for cutting-edge therapeutics like those in bladder cancer.
The Inflation Reduction Act marks a significant policy shift by enabling Medicare to directly negotiate prices for select high-cost drugs, aiming to lower patient out-of-pocket expenses. While its current scope primarily targets Part D medications, namely oral therapies and not intravesical treatments, it introduces a $2,000 annual cap on out-of-pocket drug spending beginning in 2025. Importantly, it also eliminates cost-sharing in the catastrophic coverage phase, providing welcome relief for many patients facing steep monthly medication bills. By allowing patients to spread costs more evenly throughout the year, the legislation aims to create predictability and ease financial toxicity, although its impact on bladder cancer patients will likely depend on whether future expansions include urologic oncology agents.
The No Surprises Act, originally passed under the Trump 1.0 administration, protects patients from unexpected medical bills when receiving care from out-of-network providers, often during emergencies or in hospitals where certain clinicians aren't in-network, even if the facility is. It also mandates clearer cost estimates before treatment. While not bladder cancer–specific, its relevance becomes clear when considering the complexity of care pathways in bladder cancer, which often involve multiple specialties (urologic surgery, medical oncology, radiology, anesthesia) and high-cost treatments. This law helps ensure that patients undergoing cystectomy, chemotherapy, or imaging don’t face unanticipated bills from providers they didn’t even know were out-of-network an important safeguard in an already financially burdensome disease setting.
Looking ahead, several proposed federal bills could significantly impact financial toxicity for patients with bladder cancer and other urologic malignancies. Legislation such as the Cancer Drug Parity Act, Prescription Drug Affordability Act, and the Improving Seniors’ Timely Access to Care Act aims to reduce out-of-pocket (OOP) costs, ensure fair access to oral vs. IV therapies, and streamline prior authorizations issues, particularly relevant for patients navigating complex, multimodal bladder cancer treatment. There have even been proposals to fund non-medical trial-related costs, like parking an acknowledgment that financial barriers extend beyond drug costs alone. As policy interest in drug pricing and patient affordability grows, it's clear this is top-of-mind for lawmakers. Continued advocacy is crucial not only to support the passage of these bills but also to ensure transparent pricing, predictable cost structures, and effective implementation of existing laws, all of which are essential to making novel therapies accessible to the patients who need them most.
For bladder cancer drugs, especially in the post-BCG setting, rising costs mean tighter control over access. Medicare and Medicaid coverage require prior approval, and payers are increasingly relying on utilization management protocols such as step therapy and prior authorizations to ensure appropriate use of high-cost treatments. Looking ahead, the likely "future state" will involve structured escalation protocols where access to next-line therapies is based on cost tiers, meaning patients may need to fail lower-cost options before qualifying for newer, more expensive drugs.
Dr Talwar noted that the evolving landscape of bladder cancer care is pushing a shift away from traditional fee-for-service models toward value-based arrangements. These models aim to bundle all services related to a condition into a single payment, rewarding quality over quantity. Initiatives like the CMS Enhanced Oncology Model and Vanderbilt’s MyOncology Health Model reflect this shift, incentivizing providers to deliver coordinated, cost-efficient care.
Innovative care delivery, such as at-home intravesical therapy and infusion services, is gaining traction, helping reduce patient burden and overall costs. With Medicare and Medicaid increasingly focused on these models, future payment structures may hinge on outcomes rather than service volume, especially as programs like Mayo Clinic’s ongoing research explore home-based treatment delivery. Where patients receive these therapies and how they’re reimbursed will be central to achieving sustainable, high-quality care.
Providers play a critical role in supporting patients through the financial complexities of cancer care. At the clinic level, care navigation and financial counseling can make a significant difference. Leveraging pharmaceutical assistance programs and grants can alleviate out-of-pocket burdens for those who may not otherwise afford treatment. Tools like real-time benefit checks used at institutions like Vanderbilt allow physicians to see estimated drug costs at the time of prescribing, enabling transparent discussions with patients about affordability. For those on Medicare Part D, public tools are also available to preview medication costs. These proactive steps can empower patients to make informed decisions and avoid unexpected financial strain.
Lastly, advocacy plays a critical role in shaping policy to improve access and affordability in bladder cancer care. Dr Talwar encouraged us to engage with organizations like BCAN, ASCO, and AUA to amplify their voices through coordinated efforts such as congressional fly-ins, patient–physician meetings with lawmakers, and letters to representatives. These efforts demonstrate collective strength and ensure that legislators hear directly from the experts who understand patient needs and system challenges. Building these relationships helps influence meaningful legislation that supports patients and the future of bladder cancer treatment.
Presented by:
Co-Chairs: Parminder Singh, MD, Mayo Clinic; Matthew Mossanen, MD, MPH, Brigham and Women’s Hospital, Harvard Medical School; Ruchika Talwar, MD, MMHC, Vanderbilt University Medical Center.
- Richard Toner, Division Chair, Revenue, Strategy, and Innovation at Mayo Clinic College of Medicine
- Michael Louie, MD, MPH, MSc, EVP, Medical Affairs and Clinical Development, UroGen Pharma Inc.
- Stephanie Spence, PharmD, CSP, Certified Specialty Pharmacist Managed Care Leader
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the Bladder Cancer Advocacy Network (BCAN) Bladder Cancer Think Tank 2025 held in Washington D.C., United States, between July 30th and August 1st.
Reference:
- Mossanen M, Wang Y, Szymaniak J, Tan WS, Huynh MJ, Preston MA, Trinh QD, Sonpavde G, Kibel AS, Chang SL. Evaluating the cost of surveillance for non-muscle-invasive bladder cancer: an analysis based on risk categories. World J Urol. 2019 Oct;37(10):2059-2065. doi: 10.1007/s00345-018-2550-x. Epub 2018 Nov 16. PMID: 30446799.
- Shore ND, Powles TB, Bedke J, Galsky MD, Palou Redorta J, Ku JH, Kretkowski M, Xylinas E, Alekseev B, Ye D, Guerrero-Ramos F, Briganti A, Kulkarni GS, Brinkmann J, Calella AM, Cesari R, Eccleston A, Michelon E, Vermette J, Wei C, Steinberg GD. Sasanlimab plus BCG in BCG-naive, high-risk non-muscle invasive bladder cancer: the randomized phase 3 CREST trial. Nat Med. 2025 May 31. doi: 10.1038/s41591-025-03738-z. Epub ahead of print. Erratum in: Nat Med. 2025 Jul 21. doi: 10.1038/s41591-025-03894-2. PMID: 40450141.
- Ran Sun et al.Treatment patterns with intravesical bacillus Calmette-Guérin (BCG) in patients with non-muscle-invasive bladder cancer (NMIBC): A real-world data analysis.. JCO 42, e16584-e16584(2024) DOI:10.1200/JCO.2024.42.16_suppl.e16584
- Powles T, Valderrama BP, Gupta S, Bedke J, Kikuchi E, Hoffman-Censits J, Iyer G, Vulsteke C, Park SH, Shin SJ, Castellano D, Fornarini G, Li JR, Gümüş M, Mar N, Loriot Y, Fléchon A, Duran I, Drakaki A, Narayanan S, Yu X, Gorla S, Homet Moreno B, van der Heijden MS; EV-302 Trial Investigators. Enfortumab Vedotin and Pembrolizumab in Untreated Advanced Urothelial Cancer. N Engl J Med. 2024 Mar 7;390(10):875-888. doi: 10.1056/NEJMoa2312117. PMID: 38446675.
- Sertkaya A, Beleche T, Jessup A, Sommers BD. Costs of Drug Development and Research and Development Intensity in the US, 2000-2018. JAMA Netw Open. 2024 Jun 3;7(6):e2415445. doi: 10.1001/jamanetworkopen.2024.15445. PMID: 38941099; PMCID: PMC11214120.