(UroToday.com) The Bladder Cancer Advocacy Network (BCAN) Bladder Cancer Think Tank 2025 held in Washington D.C., United States, between July 30th and August 1st. was host to the Session BCAN-Funded Investigator Speakers - Rapid Research Update 2025. Dr. Bishoy Faltas presented Bio-Digital Avatars for Personalized Sequencing of Bladder Cancer Therapies.
Dr. Faltas discussed the limitations of the current one-size-fits-all approach to treating metastatic bladder cancer, which is typically guided by standardized treatment algorithms. He pointed out that this framework fails to account for tumor evolution over time, especially the emergence of multidrug-resistant clones through successive lines of therapy. To address this, his team developed a deep reinforcement learning model designed to personalize treatment sequencing. This strategy dynamically adapts to tumor evolution, aiming to restrict the growth of resistant subclones and ultimately improve clinical outcomes.
He introduced the concept of adaptive therapy as a way to counteract treatment resistance in metastatic bladder cancer. Rather than relying on fixed, high-intensity dosing strategies that may inadvertently select for resistant clones, adaptive therapy seeks to maintain a controlled tumor burden by adjusting treatment based on tumor dynamics. He referenced modeling work that illustrates how this approach may preserve sensitive cell populations and delay resistance as illustrated below.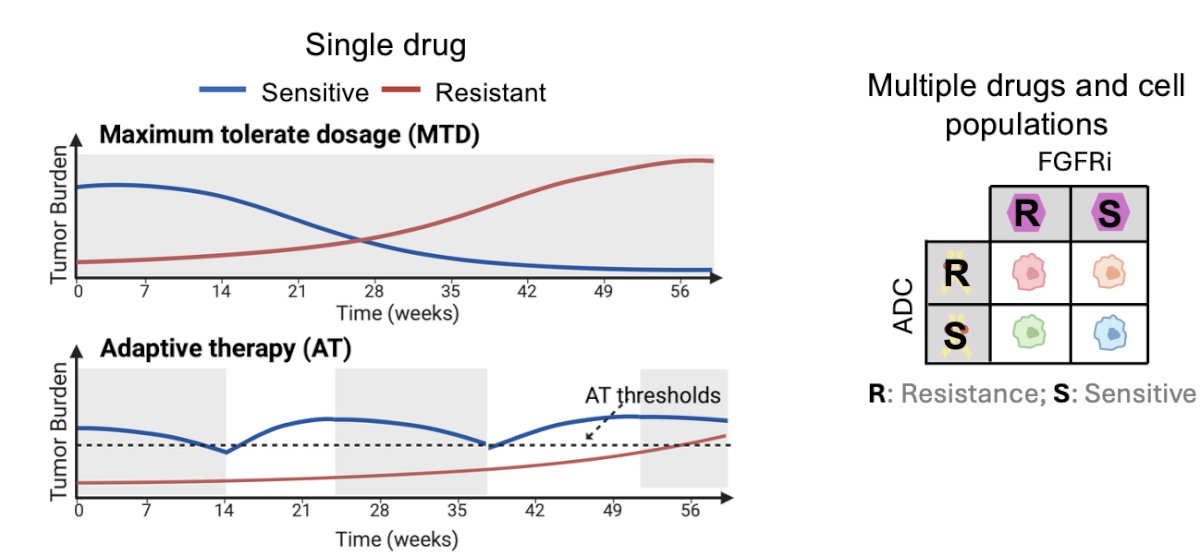
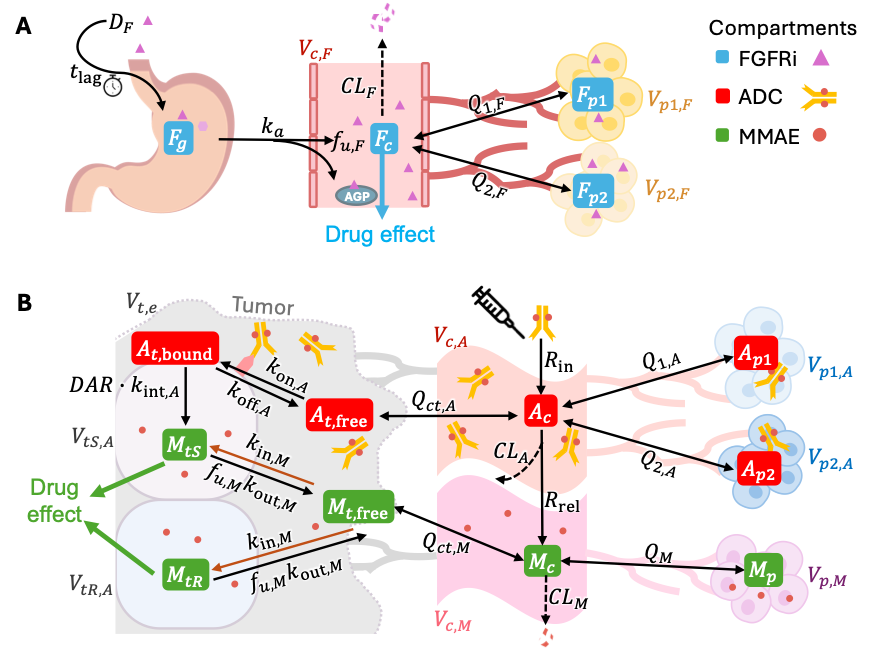
Dr. Faltas and his team developed a mathematical, patient-specific virtual model designed to simulate tumor behavior and guide personalized treatment sequencing. The model uses a mechanistic, bottom-up approach, incorporating a system of coupled ordinary differential equations (ODEs) for each individual. These equations account for:
- The genetic composition of the cancer cell population
- Cancer cell proliferation dynamics
- Drug pharmacokinetics (including diffusion from bloodstream to tumor)
- Drug-specific molecular responses, such as FGFR3 receptor dimerization rates.
Model construction begins with defining tumor subpopulations and simulating ctDNA shedding. These models are then validated against clinical and experimental data, including drug concentrations and tumor volume from patient samples. Real-world measurements such as PET/CT imaging and ctDNA variant allele frequencies are used to track tumor progression. Finally, adaptive therapy schedules are optimized using deep reinforcement learning (DRL), integrating clinical constraints to adjust drug timing and selection. This in silico framework is aimed at designing more responsive, evolution-informed treatment strategies for metastatic bladder cancer.
Data Input
Data inputs for the model include serial clinical measurements of treatment response, gathered after each treatment cycle. These inputs consist of total tumor volume derived from PET/CT imaging and changes in ctDNA variant allele frequency. Together, these parameters provide a dynamic view of tumor evolution and treatment impact, allowing the model to continuously update and refine personalized therapy schedules.
Data OutputThe output of the model is a deep reinforcement learning–based AI agent that learns from longitudinal clinical data and tumor dynamics to predict the optimal personalized treatment strategy. Its primary goal is to delay or prevent the expansion of resistant tumor clones by continuously adapting therapy decisions in real time.
The AI agent incorporates knowledge-guided learning. One example is clinical action masking: if a patient previously did not respond to a specific chemotherapy, indicating resistance, the system automatically excludes that agent from consideration for a defined period such as one year before allowing a potential re-challenge as illustrated below.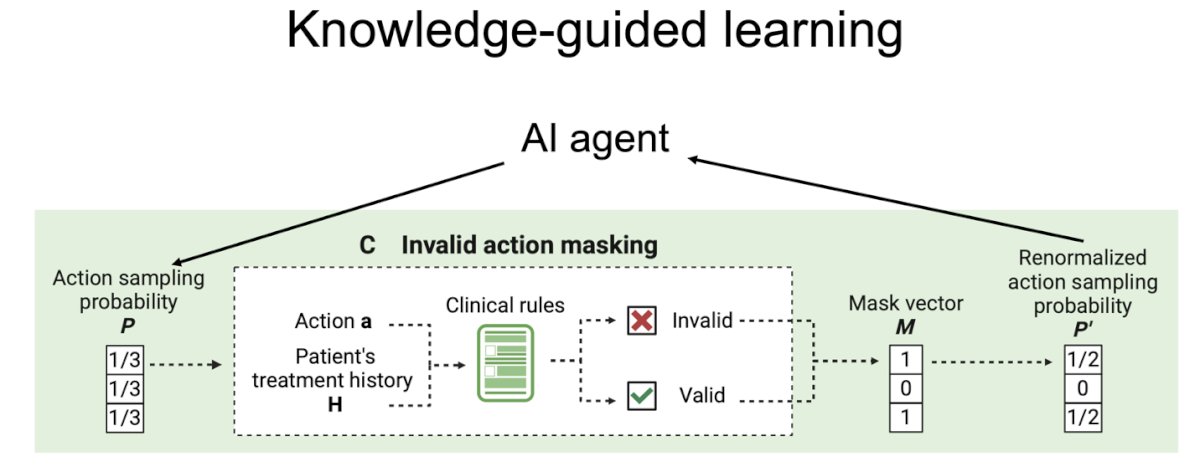
Moreover, the virtual patient model integrates mechanistic pharmacokinetic and pharmacodynamic (PK/PD) models specifically for erdafitinib and enfortumab vedotin. These models simulate how each drug is absorbed, distributed, metabolized, and acts on tumor cells over time, allowing for a more accurate prediction of treatment effects and resistance dynamics within the virtual framework.
Dr. Faltas presented data demonstrating that the virtual tumor model accurately recapitulates drug response dynamics observed in vivo. Using a mouse xenograft model treated with the FGFR inhibitor erdafitinib (10 mg/kg daily starting on day 10), the tumor volume over time closely matched the predictions generated by the model. The plotted data points reflect actual measurements, while the fitted lines represent the model’s output, showing strong agreement between the two.1

Similarly, Dr. Faltas showed validation of the virtual patient model using a mouse xenograft system treated with enfortumab vedotin. Mice received either 0.4 mg/kg or 0.8 mg/kg of EV at the time points marked by vertical gray lines. Tumor volume responses over time were measured (dots) and overlaid with model predictions (lines), demonstrating close alignment between experimental data and the virtual model. This supports the model’s ability to replicate dose-dependent tumor dynamics and further validates its potential for simulating personalized treatment strategies in bladder cancer.
Dr. Faltas presented a deep reinforcement learning–based strategy to personalize treatment sequencing in metastatic urothelial cancer. Using virtual patient models informed by tumor volume and ctDNA dynamics, the system simulates tumor evolution and adapts therapy to suppress resistant clones. Validated with xenograft data for erdafitinib (FGFRi) and enfortumab vedotin (ADC), the AI-guided approach nearly doubled time to progression compared to standard schedules, highlighting its potential to improve outcomes through adaptive, personalized treatment.
Lastly, Dr. Faltas outlined a four-step approach to transition from individual models to in silico clinical trials. First, physiological prior distributions such as tumor growth and drug response rates are defined. Next, patient-level simulations are run to generate clinical outcomes. These simulated results are then compared against completed clinical trials, and only parameters yielding acceptable matches are retained. Finally, these accepted parameters define a virtual patient cohort used to train the deep reinforcement learning model to optimize treatment outcomes.
Dr Faltas concluded his presentation with the following key messages:
- The investigators have developed a bio-digital avatar for personalized metastatic bladder cancer treatment.
- Integrating dynamical systems mechanistic modeling with deep reinforcement learning (AI) and clinical action masking.
- Using ctDNA-based dynamic treatment adjustments, the bio-digital avatar significantly extends predicted time to progression compared to standard clinical protocols.
- Next steps include building virtual patient cohorts to conduct in silico clinical trials and use DRL to optimize outcomes.
Presented by: Bishoy Faltas. MD, Associate Professor of Medicine, Weill Cornell Medical College. Chief Research Officer, Englander Institute for Precision Medicine, New York, NY.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the Bladder Cancer Advocacy Network (BCAN) Bladder Cancer Think Tank 2025 held in Washington, D.C., United States, between July 30th and August 1st
References:
- Meng X, Zhu X, Ji J, Zhong H, Li X, Zhao H, Xie G, Wang K, Shu H, Wang X. Erdafitinib Inhibits Tumorigenesis of Human Lung Adenocarcinoma A549 by Inducing S-Phase Cell-Cycle Arrest as a CDK2 Inhibitor. Molecules. 2022 Oct 9;27(19):6733. doi: 10.3390/molecules27196733. PMID: 36235266; PMCID: PMC9573074.
- Challita-Eid PM, Satpayev D, Yang P, An Z, Morrison K, Shostak Y, Raitano A, Nadell R, Liu W, Lortie DR, Capo L, Verlinsky A, Leavitt M, Malik F, Aviña H, Guevara CI, Dinh N, Karki S, Anand BS, Pereira DS, Joseph IB, Doñate F, Morrison K, Stover DR. Enfortumab Vedotin Antibody-Drug Conjugate Targeting Nectin-4 Is a Highly Potent Therapeutic Agent in Multiple Preclinical Cancer Models. Cancer Res. 2016 May 15;76(10):3003-13. doi: 10.1158/0008-5472.CAN-15-1313. Epub 2016 Mar 24. PMID: 27013195.