(UroToday.com) The Bladder Cancer Advocacy Network (BCAN) Bladder Cancer Think Tank 2025 held in Washington, D.C., United States, between July 30th and August 1st. was host to the Session: Lessons Learned from Clinical Trials. Dr. Parminder Singh discussed Navigating Intergroup Collaboration in Clinical Trials Lessons from Leading the S1806 Trial (SWOG/NRG).
The S1806 trial is a phase III randomized study evaluating the addition of atezolizumab to concurrent chemoradiotherapy in patients with localized muscle-invasive bladder cancer (MIBC). The trial enrolled 432 patients with clinical stage T2–T4aN0M0 disease, randomized 1:1 to receive either standard chemoradiation or chemoradiation plus atezolizumab. The primary endpoint is bladder-intact event-free survival (BIEFS), a composite measure designed to capture disease control without the need for cystectomy. Key secondary endpoints include overall survival (OS), disease-free survival (DFS), metastasis-free survival (MFS), cystectomy rate, quality of life (QoL), and translational biomarker analyses. The study schema is outlined below. 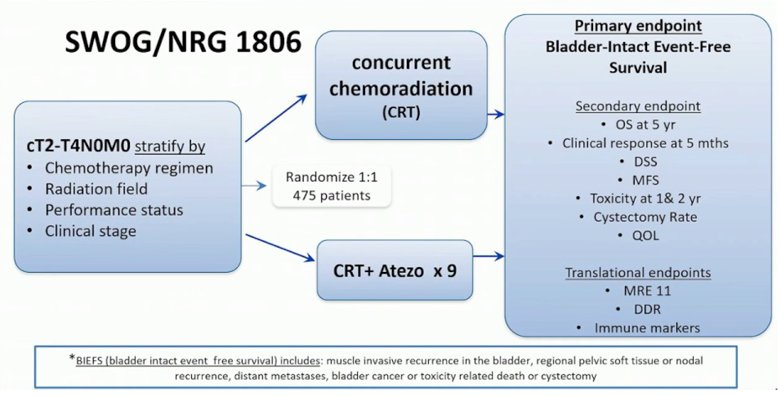
Dr. Singh, who co-chaired the SWOG S1605 trial alongside Peter Black, a phase II study of atezolizumab in BCG-unresponsive non–muscle-invasive bladder cancer, credited that experience as the foundation for the S1806 trial concept.1 Having been deeply involved in S1605, he carried forward the idea of exploring atezolizumab in combination with chemoradiation for localized MIBC. The concept was first presented at SWOG, followed by intergroup discussions and steering committee approval in 2017. In 2018, the FDA provided feedback on the proposed primary endpoint of bladder-intact event-free survival, and by 2019, the trial was activated. Remarkably, accrual was completed in 2024, exceeding the target enrollment by 50 patients. Still, Dr. Singh noted, it has been nearly a decade since the idea was first conceived, a reflection of both the complexity and persistence required to execute a cooperative group trial.
Dr. Singh emphasized that an intergroup collaboration was essential for the success of S1806. Previous trials, including several from RTOG, had faced significant challenges with slow accrual, raising concerns about feasibility. However, RTOG’s prior experience and input were critical in refining the trial design. Partnering with ECOG helped expand site access and boost accrual potential.
Dr. Singh reflected on the pre-approval responsibilities required to bring S1806 to life, noting the challenge of balancing clinical duties, four days of clinic, and one admin day per week, with limited time for research. The trial concept was rigorously vetted by SWOG, CTEP, and the FDA. Building the right team was essential, involving clinical collaborators, translational scientists, statisticians, and pharmacists. Protocol development required thoughtful attention to eligibility criteria, endpoint selection, and logistical feasibility, including whether patients could realistically travel for treatment. Engaging surgeons and radiation oncologists early on was critical, especially to harmonize standards across sites. He emphasized the importance of walking through every eligibility criterion to assess how it would play out in real-world practice. He noted, underscoring that launching a trial like this requires a committed and multidisciplinary team.
Dr. Singh spoke about the post-approval responsibilities of being a principal investigator, which are sometimes overlooked. This includes reviewing charts, addressing eligibility concerns, evaluating adverse events, responses, deaths, and progression events, all while fielding protocol-related questions from sites across the country. He is also responsible for ensuring ongoing protocol compliance. Importantly, much of this work is done without dedicated support or protected salary, highlighting the personal investment often required to see a cooperative group trial through to completion.
Beyond clinical oversight, Dr. Singh highlighted the ongoing need for dedicated translational research coordination. This includes ensuring timely tissue submission, maintaining sample quality, and addressing protocol deviations when they arise. He helps lead monthly meetings with clinical research coordinators and is responsible for presenting regular updates at SWOG and investigator meetings. One key decision, such as discarding the buffy coat, means that the sample type won’t be available for analysis in this trial. Still, S1806 now represents the largest collection of tissue and urine specimens in any bladder cancer study to date, offering an unprecedented opportunity for future correlative science.
Dr. Singh emphasized the tangible outcomes that can emerge from leading a cooperative group trial like S1806. Beyond advancing the science, these efforts open doors for meaningful leadership opportunities ranging from authorship on national presentations to eligibility for major grants and funding mechanisms. Such roles also elevate institutional recognition and can lead to broader leadership positions within cooperative group structures, creating a platform for continued impact at the national level.
Dr. Singh shared a few hard-earned negotiation lessons from his experience leading S1806. First, be present early at the negotiating table; decisions made at the outset often shape the entire trajectory of the trial. It’s important to push for clear effort distribution from the start, ensuring that responsibilities are well-defined and manageable. Equally critical is aligning effort with recognition; those doing the work should receive appropriate credit. And finally, don’t be afraid to ask for help; no one is expected to know everything, and collaboration is key to navigating the complexity of cooperative group trials.
A clear distinction between registration and non-registration trials was made, noting that the latter are often much simpler to execute. For those considering leading a trial in the future, he offered practical advice. First, understand the full scope of work before committing to registration trials, in particular come with significant regulatory and logistical demands. Engage early with cooperative group leadership to align expectations and resources. Be proactive about authorship discussions and securing proper credit for your effort. Finally, build support for translational science from the beginning, as these components can be complex but ultimately elevate the impact of the study.
Dr. Singh concluded his presentation with the following key takeaways:
- Intergroup trials bring added complexity, but offer greater reach and impact
- As PI, expect to serve as the operational and communication hub
- Strategic negotiation and stakeholder engagement are just as critical as scientific vision
- Maintain visibility, seek support, and stay actively involved at every stage of the process.
Presented by: Parminder Singh, MD, Hematologist, Oncologist, Mayo Clinic, Phoenix, AZ.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the Bladder Cancer Advocacy Network (BCAN) Bladder Cancer Think Tank 2025 held in Washington, D.C., United States, between July 30th and August 1st
Reference: