(UroToday.com) The 2026 American Urologic Association (AUA) Annual Meeting was host to an upper tract urothelial carcinoma (UTUC) poster session. Dr. Ali Zahalka presented the long-term, follow-up efficacy and safety outcomes of accelerated methotrexate, vinblastine, Adriamycin, and cisplatin (aMVAC) from the phase II trial of neoadjuvant systemic chemotherapy followed by extirpative surgery for patients with high-grade UTUC.
Historically, prospective data supporting neoadjuvant chemotherapy in UTUC have been limited. ECOG-ACRIN EA8141 was designed to address this evidence gap by evaluating four cycles of cisplatin-based neoadjuvant chemotherapy in cisplatin-eligible patients with high-grade UTUC undergoing radical nephroureterectomy. Initial results established a pathologic complete response (pCR) rate of 14%, helping provide the prospective evidence base that has led to neoadjuvant cisplatin-based chemotherapy becoming the standard of care for eligible patients with high-risk UTUC.
EA8141 was a prospective, multicenter phase II trial (ClinicalTrials.gov identifier NCT02412670) that enrolled patients with high-grade UTUC treated with four cycles of neoadjuvant aMVAC followed by nephroureterectomy. The primary endpoint was pathologic complete response, defined as ypT0N0. Secondary endpoints included recurrence-free survival (RFS), event-free survival (EFS), bladder cancer-free survival (BCFS), and overall survival (OS).
For the long-term analyses, pathologic responders were defined as patients with ypT0–1N0 disease, whereas non-responders were defined as those with residual ≥ypT2 disease and/or nodal metastases.
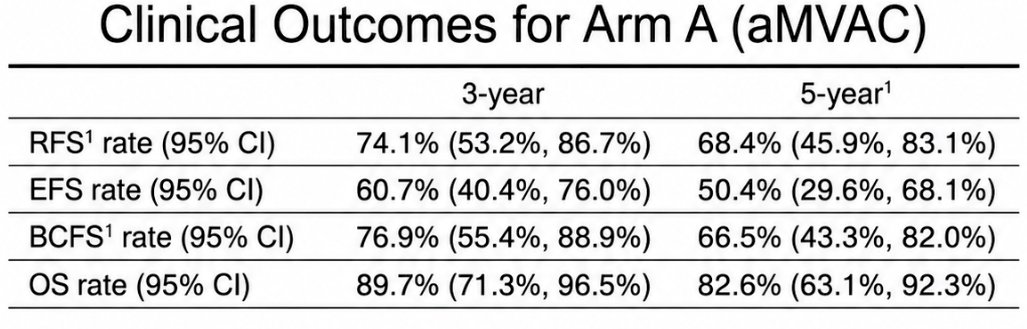
The central results table demonstrated durable oncologic outcomes following neoadjuvant aMVAC and surgery.
At 3 years:
- Recurrence-free survival: 74.1% (95% CI 53.2–86.7%)
- Event-free survival: 60.7% (95% CI 40.4–76.0%)
- Bladder cancer-free survival: 76.9% (95% CI 55.4–88.9%)
- Overall survival: 89.7% (95% CI 71.3–96.5%)
At 5 years:
- Recurrence-free survival: 68.4% (95% CI 45.9–83.1%)
- Event-free survival: 50.4% (95% CI 29.6–68.1%)
- Bladder cancer-free survival: 66.5% (95% CI 43.3–82.0%)
- Overall survival: 82.6% (95% CI 63.1–92.3%)
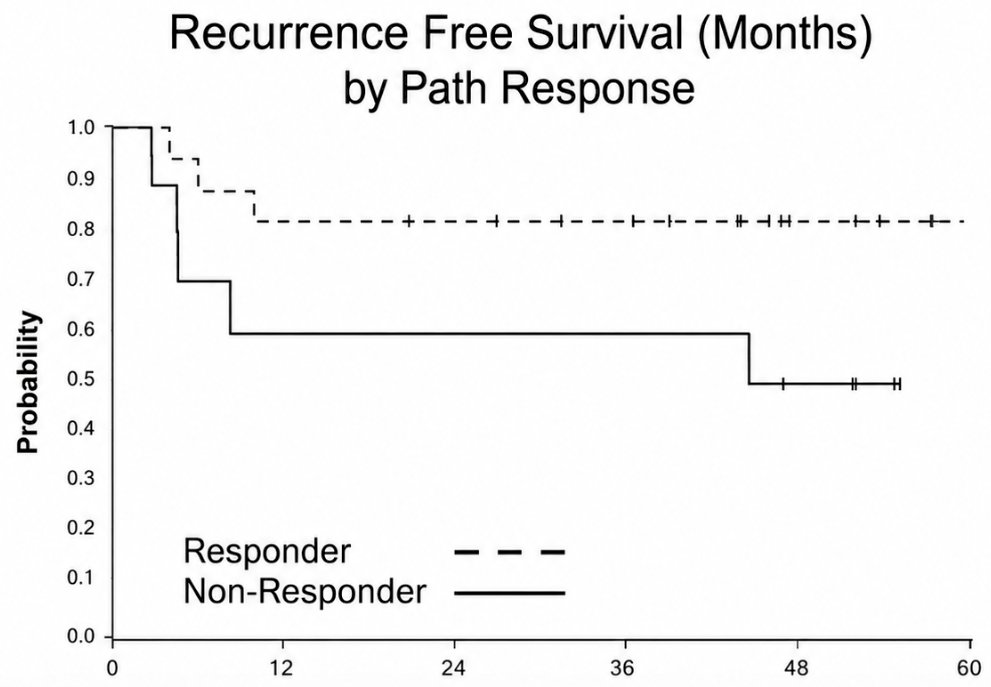
The Kaplan–Meier curve for recurrence-free survival by pathologic response showed a striking separation between responders and non-responders. Patients achieving ypT0–1N0 maintained an approximately 80% recurrence-free survival probability throughout five years of follow-up, whereas non-responders experienced an early decline within the first year and a subsequent plateau around 50%. These findings underscore the strong prognostic significance of pathologic downstaging after neoadjuvant chemotherapy.
The investigators concluded that long-term follow-up continues to support a meaningful and durable clinical benefit of neoadjuvant aMVAC in cisplatin-eligible patients with high-grade UTUC. In addition to inducing pathologic complete responses, neoadjuvant chemotherapy was associated with favorable long-term recurrence-free, bladder cancer-free, and overall survival outcomes.
These results are particularly important because they provide mature prospective evidence demonstrating that neoadjuvant cisplatin-based chemotherapy not only improves pathologic outcomes but also translates into durable long-term oncologic benefit. Together with prior EA8141 reports, these findings firmly establish neoadjuvant chemotherapy as the standard-of-care approach for eligible patients with high-grade UTUC.
Presented by: Ali Zahalka, MD, Department of Urology, The University of Texas Southwestern Medical Center, Dallas, TX
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.