(UroToday.com) The 2026 American Urologic Association (AUA) Annual Meeting was host to an upper tract urothelial carcinoma (UTUC) poster session. Dr. Marie Semmler presented a study evaluating deep early tumor shrinkage in metastatic upper tract urothelial carcinoma treated with first-line enfortumab vedotin plus pembrolizumab (EV+P).
Tumor response during systemic therapy is traditionally assessed using the Response Evaluation Criteria in Solid Tumors (RECIST), later updated to RECIST version 1.1.1,2 Although immune-related RECIST (iRECIST) criteria were developed to account for pseudoprogression,3 radiographic objective response does not always translate into durable clinical benefit. This issue is particularly relevant in metastatic UTUC, which is increasingly recognized as a biologically and clinically distinct disease entity characterized by more aggressive disease dynamics and important molecular and genetic differences compared with urothelial carcinoma arising from the lower urinary tract.
The phase 3 EV-302 trial established enfortumab vedotin plus pembrolizumab (EV+P) as a new first-line standard of care for metastatic urothelial carcinoma, including patients with metastatic UTUC.4 In this context, the investigators performed an in-depth radiologic assessment to determine whether deep early tumor shrinkage—defined as at least a 50% reduction in overall tumor burden at first follow-up imaging—could serve as an early marker of durable clinical benefit.
Baseline and follow-up imaging from patients with metastatic UTUC treated with first-line EV+P were retrospectively reviewed by a board-certified radiologist with subspecialty expertise in urothelial cancer imaging. The analysis included objective response, lesion-specific response, changes in overall tumor burden, and deep early tumor shrinkage.
The study cohort consisted of 16 patients. The median age was 73 years (interquartile range [IQR] 57–80), and 56% were male. Primary tumors originated in the renal pelvis in 69% and the ureter in 31%. Metastatic disease was present at initial diagnosis in 69%, while 31% developed secondary metastatic disease. Most patients had ECOG performance status 0–1 (88%), and 75% harbored multiple metastatic sites. Prior surgical treatment had been performed in 38%, and 38% had received previous systemic therapy.
![The study cohort consisted of 16 patients. The median age was 73 years (interquartile range [IQR] 57–80), and 56% were male. Primary tumors originated in the renal pelvis in 69% and the ureter in 31%. Metastatic disease was present at initial diagnosis in 69%, while 31% developed secondary metastatic disease. Most patients had ECOG performance status 0–1 (88%), and 75% harbored multiple metastatic sites. Prior surgical treatment had been performed in 38%, and 38% had received previous systemic therapy.](/images/com-doc-importer/265-aua-2026/aua-2026-evaluating-deep-early-tumor-shrinkage-in-metastatic-upper-tract-urothelial-carcinoma-treated-with-enfortumab-vedotin-plus-pembrolizumab/image-0.jpg)
At a median time on EV+P of 8 months (IQR 3–11), the median progression-free survival was 11 months (IQR: 8–NR), and the median overall survival was 13 months (IQR: 11–NR). The objective response rate was 69%, including complete responses in 13% and partial responses in 56%.
The median reduction in overall tumor burden at first follow-up imaging was 39% (IQR: 25–55%), and 27% of patients achieved deep early tumor shrinkage, defined as ≥50% decrease in tumor burden.
Lesion-specific analyses demonstrated substantial heterogeneity in response by metastatic site. Primary upper tract lesions exhibited a median shrinkage of 16% (IQR: 11–30). Among metastatic lesions, median shrinkage was 47% (IQR: 30–100) for lymph nodes, 39% (IQR: 19–48) for bone metastases, 55% (IQR: 27–61) for liver metastases, 80% (IQR: 70–90) for lung lesions, and 100% (IQR: 50–100) for other metastatic sites.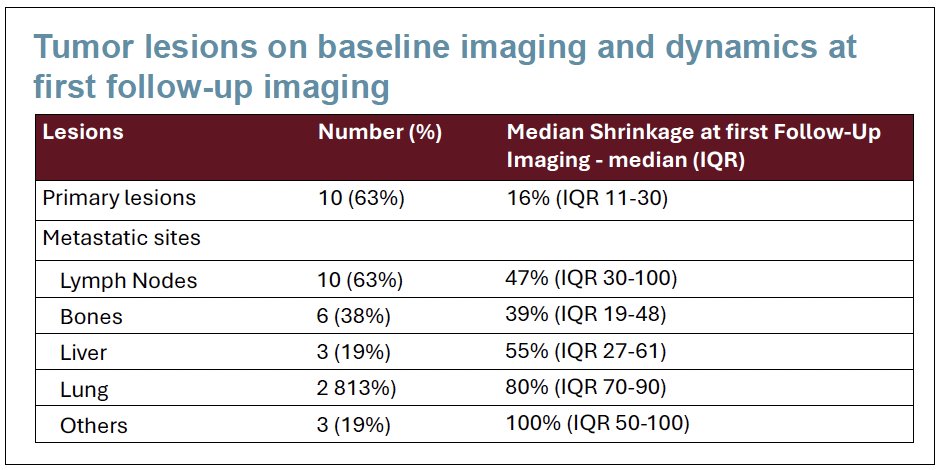

Kaplan–Meier analyses demonstrated that conventional RECIST response categories (partial or complete response versus stable disease) were associated with differences in progression-free and overall survival.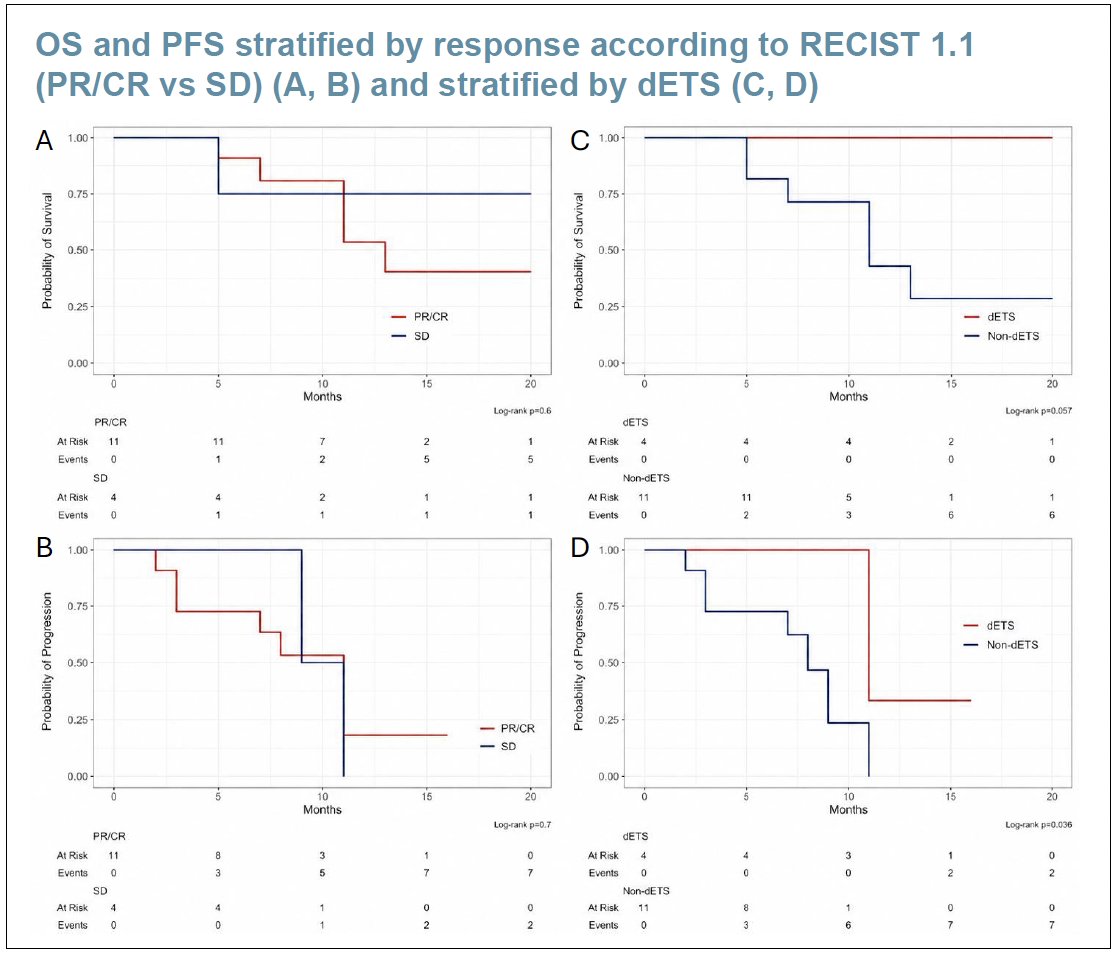
The tumor burden dynamics plot further supports the prognostic significance of deep early tumor shrinkage. Patients who achieved deep early tumor shrinkage (red lines), defined as a ≥50% reduction in tumor burden at the 3-month assessment, demonstrated consistently high levels of tumor reduction that were largely maintained through months 6 and 9. In contrast, patients who did not achieve deep early tumor shrinkage (blue lines) exhibited more heterogeneous trajectories, including smaller initial responses, fluctuating tumor burden over time, and several cases of subsequent disease progression. Together, these findings suggest that achieving dETS identifies a subset of patients with more durable and sustained responses to enfortumab vedotin plus pembrolizumab and supports its role as an early prognostic marker of long-term clinical benefit.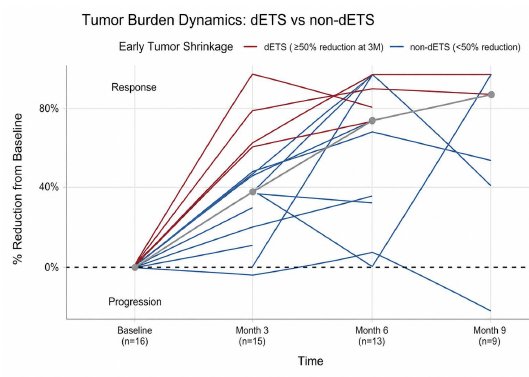
The investigators concluded that RECIST-based response assessment alone may be insufficient to fully capture durable clinical benefit in patients with metastatic UTUC treated with EV+P. Deep early tumor shrinkage may help identify patients who derive sustained benefit and could complement conventional radiographic response assessment to guide early treatment decisions. Future efforts will focus on integrating artificial intelligence-assisted multivariable imaging analysis along with tumor dynamics, tumor biology, and circulating biomarkers to improve early response prediction.
Presented by: Marie Semmler, MD, Department of Urology, LMU University Hospital, LMU Munich, Munich, Germany
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the AUA 2026 Annual Meeting, Washington, DC, May 15th–18th, 2026
References:- Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45(2):228–247.
- Therasse P, Arbuck SG, Eisenhauer EA, et al. New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J Natl Cancer Inst. 2000;92(3):205–216.
- Seymour L, Bogaerts J, Perrone A, et al. iRECIST: Guidelines for response criteria for use in trials testing immunotherapeutics. Lancet Oncol. 2017;18(3):e143–e152.
- Powles T, Valderrama BP, Gupta S, et al. Enfortumab vedotin and pembrolizumab in untreated advanced urothelial cancer. N Engl J Med. 2024;390(10):875–888.