(UroToday.com) The 2026 American Urologic Association (AUA) Annual Meeting was host to an upper tract urothelial carcinoma (UTUC) poster session. Dr. Patrick Mershon presented the results of a retrospective TriNetX cohort study evaluating the incidence of ureteral strictures and subsequent interventions following mitomycin treatment for UTUC.
UTUC is a relatively uncommon malignancy, with an annual incidence of approximately 2 cases per 100,000 persons in Western countries.1 Management options for low-risk UTUC include endoscopic resection, radical nephroureterectomy, and pelvicalyceal chemoablation.2 A reverse thermal gel formulation of mitomycin was approved by the U.S. Food and Drug Administration in 2020 for the treatment of low-risk UTUC.3 In the pivotal OLYMPUS trial, ureteral stenosis was the most common complication, occurring in 44% (31/71) of treated patients.4
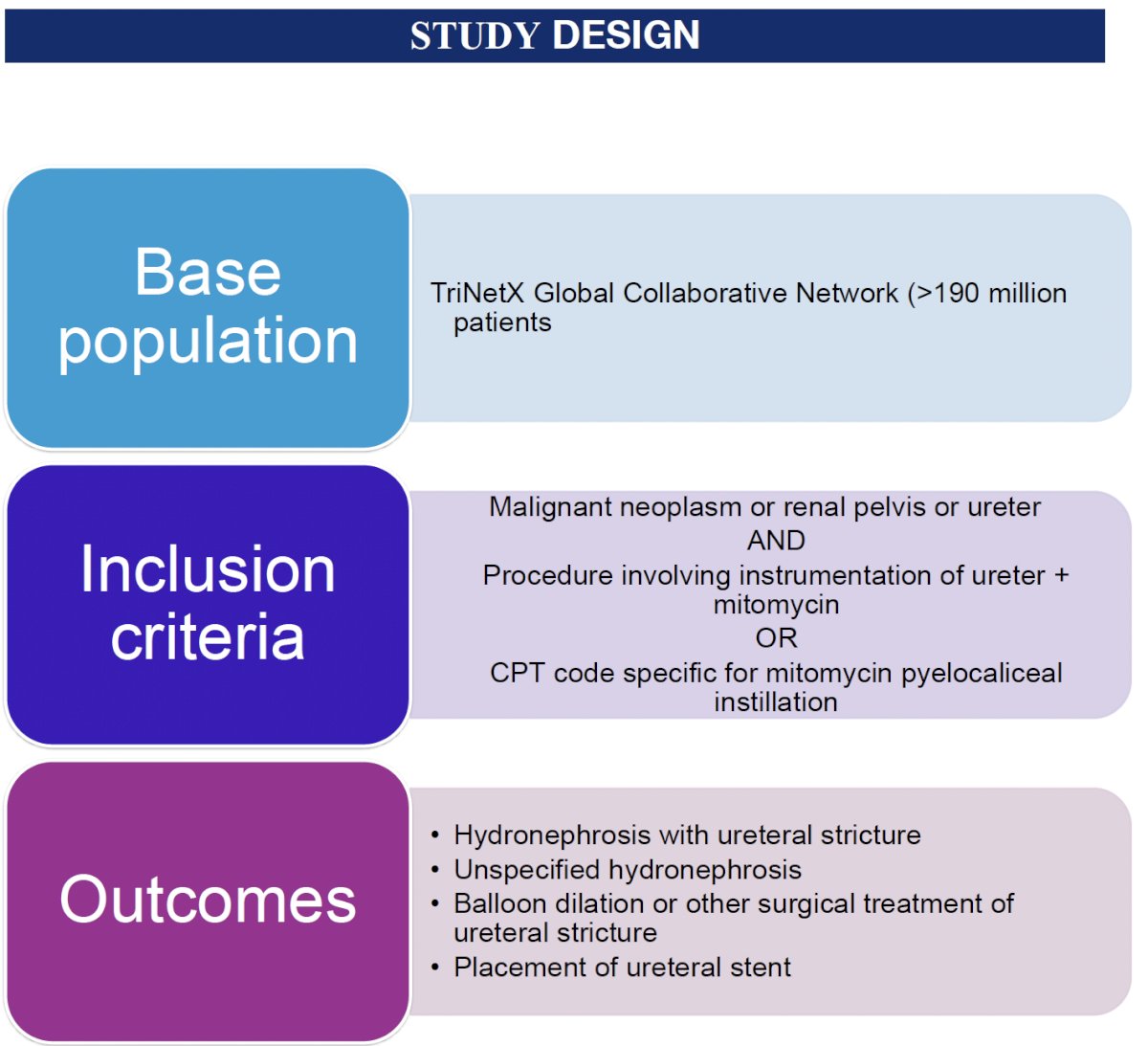
The objective of the current study was to characterize real-world rates of ureteral stricture and stricture-related interventions in a large cohort of patients receiving mitomycin for UTUC.
The investigators used the TriNetX Global Collaborative Network, which includes data from more than 190 million patients worldwide. Eligible patients had a diagnosis of malignant neoplasm of the renal pelvis or ureter and underwent ureteral instrumentation with mitomycin administration, including identification through a CPT code specific for mitomycin pyelocaliceal instillation. Outcomes of interest included hydronephrosis with ureteral stricture, unspecified hydronephrosis, balloon dilation or other surgical treatment of ureteral stricture, and ureteral stent placement.
The study cohort consisted of 750 patients, with a mean age of 79.2 years (standard deviation [SD] 9.3) and a mean age at the index event of 72.8 years (SD 9.6). Seventy percent of patients were male, 84% were White, 53% had malignant neoplasms of the ureter, and 46% had tumors involving the renal pelvis.![The study cohort consisted of 750 patients, with a mean age of 79.2 years (standard deviation [SD] 9.3) and a mean age at the index event of 72.8 years (SD 9.6). Seventy percent of patients were male, 84% were White, 53% had malignant neoplasms of the ureter, and 46% had tumors involving the renal pelvis.](/images/com-doc-importer/265-aua-2026/aua-2026-ureteral-stricture-and-subsequent-intervention-after-mitomycin-treatment-for-upper-tract-urothelial-carcinoma-a-retrospective-trinetx-cohort-study/image-1.jpg)
The cumulative incidence of upper tract obstruction and related interventions increased substantially over time. Within one month of treatment, approximately 7% of patients had hydronephrosis, and 6% underwent ureteral stent placement. By three months, these figures increased to roughly 12% and 14%, respectively. At one year, the burden became more pronounced, with 24% of patients experiencing hydronephrosis, 18% undergoing balloon dilation or other endoscopic repair for ureteral stricture, and 35% requiring ureteral stent placement.

Longer-term follow-up demonstrated that these complications continued to accumulate. At five years, 45% of patients had an encounter diagnosis of hydronephrosis, approximately one-third had undergone endoscopic or surgical repair of a ureteral stricture, and nearly half required ureteral stent placement.
These findings closely mirror those reported in the OLYMPUS trial, in which 68% of patients experienced a renal or urinary system adverse event, and 34% underwent temporary ureteral stent placement.4 Importantly, the present analysis extends those observations by demonstrating that ureteral obstruction frequently necessitates repeated interventions in routine clinical practice.
The investigators concluded that this large, real-world study corroborates the pivotal OLYMPUS findings and highlights the substantial long-term burden of ureteral stricture and associated procedures after mitomycin treatment for UTUC. These data underscore the importance of counseling patients regarding the risk of delayed upper tract obstruction and the potential need for subsequent stent placement or endoscopic stricture management.
Presented by: Patrick Mershon, MD, Urology Institute, University Hospitals, Cleveland, Ohio, USA
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the AUA 2026 Annual Meeting, Washington, DC, May 15th–18th, 2026
References:- Rouprêt M, Babjuk M, Compérat E, et al. European Association of Urology guidelines on upper urinary tract urothelial carcinoma: 2017 update. Eur Urol. 2018;73(1):111–122.
- Coleman JA, Clark PE, Bixler BR, et al. Diagnosis and management of non-metastatic upper tract urothelial carcinoma: AUA/SUO guideline. J Urol. 2023;209(6):1071–1081.
- U.S. Food and Drug Administration. FDA approves mitomycin for low-grade upper tract urothelial cancer. April 15, 2020. Available at: https://bit.ly/2xxaVMu.
- Ourfali S, Colombel M. Re: Primary chemoablation of low-grade upper tract urothelial carcinoma using UGN-101, a mitomycin-containing reverse thermal gel (OLYMPUS): An open-label, single-arm, phase 3 trial. Eur Urol. 2021;79(1):162.