(UroToday.com) The 2026 AUA annual meeting featured the International Prostate Forum and a presentation by Dr. John Davis discussing the daily triage of Grade Group 2 prostate cancer. Dr. Davis started his presentation highlighting that there has been an evolving scope of active surveillance over the decades:
- 1990’s/early 2000’s: it’s dangerous and there’s a risk of stage migration
- 2005: ok, maybe low grade prostate cancer on a clinical trial
- 2010 NCCN: now part of the guidelines
- 2015: now part of clinical practice
- 2016-2023: ok, maybe Grade Group 2 as well?

For new patient consults with low to intermediate risk prostate cancer, it is important to optimize diagnostics, review the current medical advice/literature, and use shared decision making to finalize the treatment plan:

To assist with these discussions and decisions, there are several prognostic variables at our disposal:
- PSA density
- Volume of cores
- Add the percentage of pattern 4
- Family history
- Genetic mutations
- Genomic scores: Decipher, Prolaris, Oncotype, etc
- MRI visible disease
For Grade Group 1 patients, the goals should be to follow these patients carefully, predict progression to treatment, de-escalate monitoring if feasible, and not pre-emptively treat, even if there are multiple risk factors for progression.
Over the last several years, there has been conflicting evidence and opinions in the literature regarding whether active surveillance should be routinely used for intermediate-risk prostate cancer. There have been 3 historic randomized clinical trials in this space. Dr. Davis notes that PIVOT1 and SPCG-42 make it difficult to make modern Grade Group 2 active surveillance conclusions. In ProtecT,3 we can assess 15-year survival metrics, with a higher incidence of metastases, but without the use of structured biopsies and the use of MRI. Regardless, Dr. Davis emphasized that the data are not clear as to whether active surveillance is safe or unsafe for Grade Group 2 prostate cancer without further details.
There are several consistencies when assessing candidacy for active surveillance:
- There are more events in intermediate risk versus low risk prostate cancer
- Details from the prognostic variables checklist matter
- Certain factors should trigger consideration for intervention, including a high Decipher score and ductal or cribriform variants
- MRI PI-RADS 4-5 scores portend increased progression to treatment
Where disagreement arises, it is difficult to handle findings from large, non-randomized studies where risk sub-classification is less well-known. The following table summarizes the oncological outcomes of Grade Group 2 prostate cancer enrolled in active surveillance protocols:

Dr. Davis emphasized that there are several scenarios where a patient wants treatment no matter what:
- Low risk: Dr. Davis debates the patient and tries to win
- Favorable intermediate risk: Dr. Davis discusses the situation and may recommend surveillance, but they can overrule him
- Unfavorable intermediate risk: Dr. Davis finalizes treatment plans
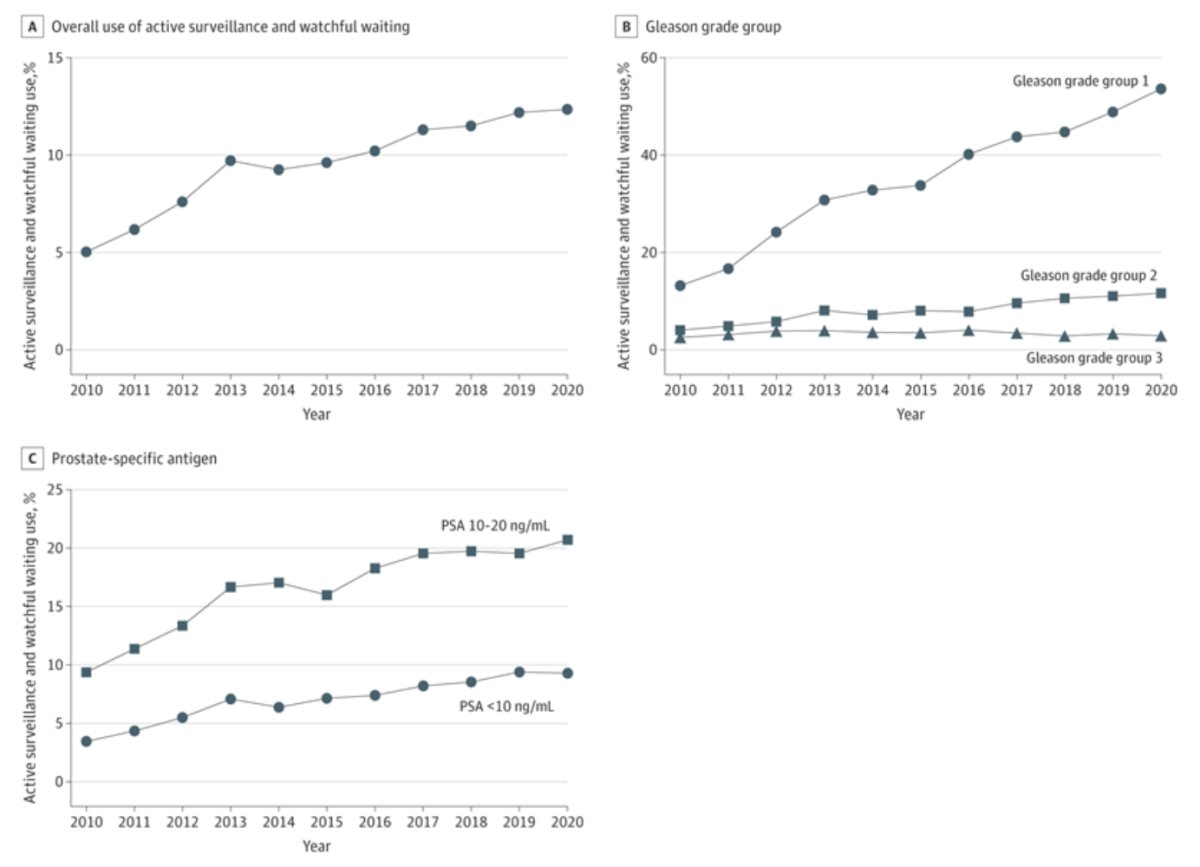
In 2024, Ajjawi et al.4 assessed active surveillance and watchful waiting trends in the SEER database. Among 147,205 individuals with intermediate risk prostate cancer from 2010-2020, the proportion of individuals diagnosed with intermediate risk prostate cancer increased from 41.7% in 2010 to 47.3% in 2020 (p < 0 .001). Active surveillance and watchful waiting use also increased from 5.0% in 2010 to 12.3% in 2020 (p < 0 .001). Moreover, its use increased from 13.2% in 2010 to 53.8% in 2020 among intermediate risk patients with Grade Group 1 (p < 0 .001), 4.0% to 11.6% among those with Grade Group 2 (p < 0 .001), and from 2.5% to 2.8% among those with Grade Group 3 (p = 0 .85). Active surveillance and watchful waiting use also increased from 3.4% in 2010 to 9.2% in 2020 among intermediate risk cases with PSA values lower than 10 ng/mL (p < 0 .001) and from 9.3% to 20.7% among those with PSA values ranging from 10 to 20 ng/mL (p <0 .001):
The 25-year follow-up of the GÖTEBORG-1 trial5 assessing active surveillance for screen-detected low and intermediate risk prostate cancer showed a 25-year overall survival rate of 94% and a treatment-free rate of 48% at 15 years:
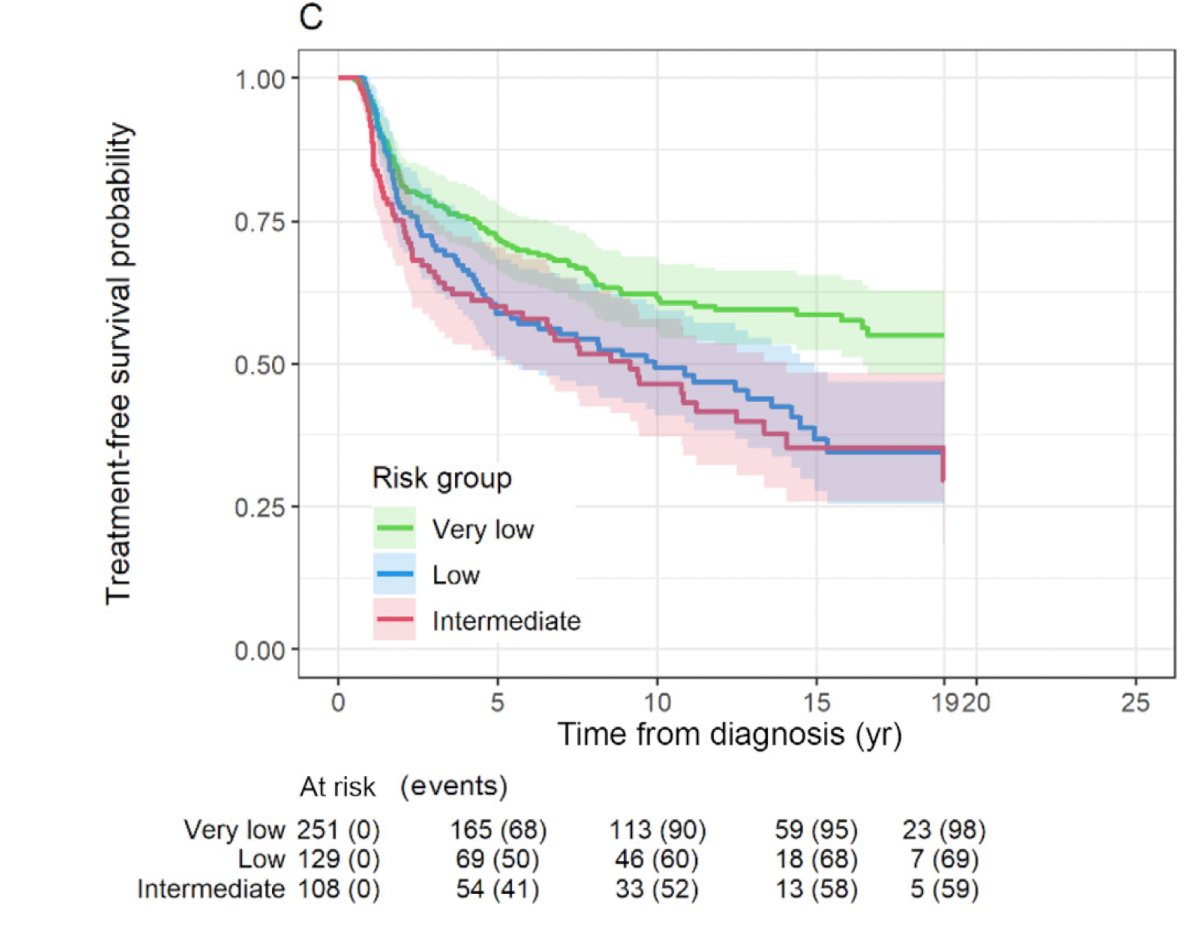
Higher failure rates were associated with shorter PSA doubling times, cT2 disease, and Gleason 7 prostate cancer. There were 264 all-cause deaths and 14 prostate cancer-specific mortalities.
In 2025, Petrelli et al.6 reported a contemporary synthesis of the evidence for active surveillance in intermediate risk prostate cancer. The 10-year outcome patterns from this study stratified by low, favorable intermediate, and unfavorable intermediate risk patients are highlighted in the following table:

This study suggests that the best candidates are those with limited Gleason 3+4 prostate cancer (specifically, limited pattern 4), low PSA density (< 0.15), and few positive cores/low tumor volume. There are several selection tools available, including mpMRI and PI-RADS, targeted + systematic biopsy, and use of genomic classifiers when uncertainty remains. Active surveillance should be used very cautiously in unfavorable intermediate risk disease, given that progression and dropout risk are higher, and standardized and durable follow-up is essential. The main conclusion from this assessment is that active surveillance is a viable option for carefully selected, favorable intermediate-risk patients, especially low-volume Gleason Grade 2 / Gleason 3+4 disease with reassuring PSA density, MRI findings, and genomic features.
With regards to the Decipher genomic classifier risk and active surveillance, a study from UCSF led by Shee et al.7 assessed the impact of a high Decipher genomic risk score (>= 0.6) on active surveillance outcomes. Primary outcomes were any upgrading (any increase in Grade Group), major upgrading (Grade Group ≥3), and unfavorable histology on subsequent biopsy. Among 486 patients, Decipher scores were associated with major upgrading after adjusting for either the CAPRA score (HR 2.00, 95% CI 1.14-3.49) or clinicodemographic variables (HR 2.65, 95% CI 1.36-5.17). Further, the Decipher score was associated with unfavorable histology after adjustment for clinicodemographic variables (HR 4.53, 95% CI 2.03-10.15) but not after adjustment for the CAPRA score:
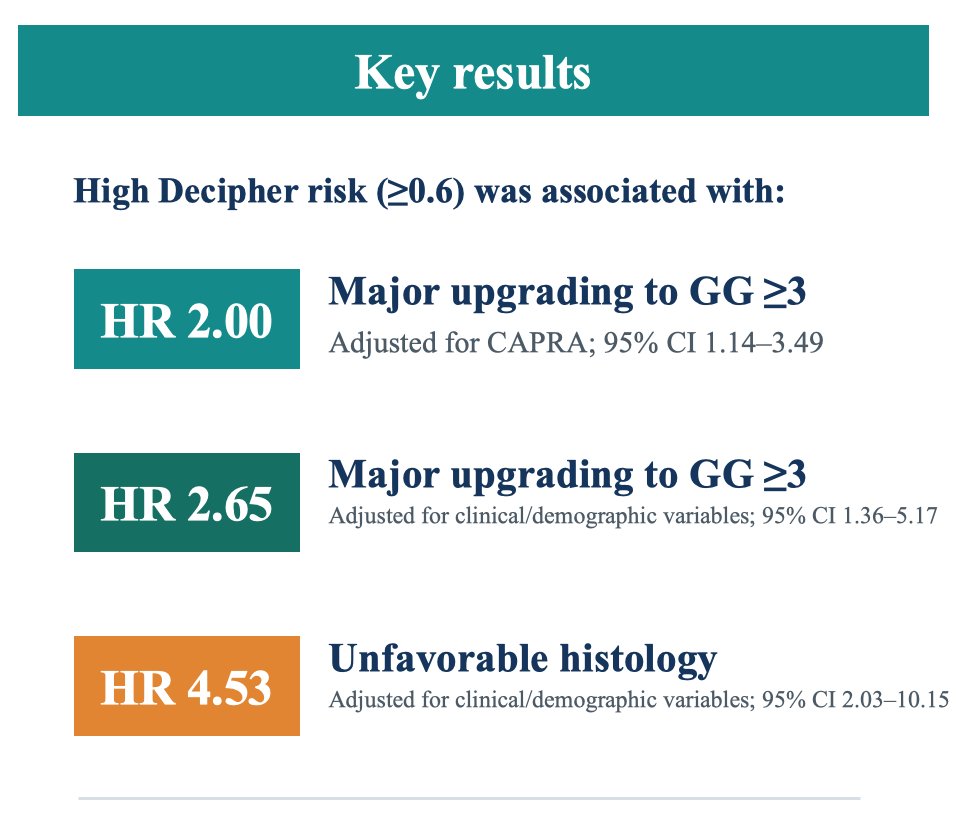
The key take-home message from this study is that Decipher appears to be most useful for identifying clinically meaningful progression on active surveillance – upgrading to Grade Group 3 or unfavorable histology – rather than any upgrade.
Finally, Dr. Davis highlighted three studies assessing MRI visible versus MRI invisible intermediate risk prostate cancer:

Taken together, among favorable intermediate risk / Grade Group 2 patients, MRI invisible status – especially without cribriform morphology – supports a more favorable surveillance profile, whereas MRI visible and cribriform disease warrant greater caution.
Dr. Davis concluded his presentation discussing the daily triage of Grade Group 2 prostate cancer with the following take-home points:
- Active surveillance for Grade Group 1 is mostly simplified by now
- Active surveillance for Grade Group 2 has room for active surveillance with further risk refinement, more counseling, optimized diagnostics, and follow-up
- For triage to treatment, there are multiple themes for “friendlier” treatment options than higher-grade/risk disease
Presented by: John Davis, MD, FACS, MD Anderson Cancer Center, Houston, TX
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
References:
- Wilt TJ, Jones KM, Barry MJ, et al. Follow-up of prostatectomy versus observation for early prostate cancer. N Engl J Med 2017;377(2):132-142.
- Bill-Axelson A, Holmberg L, Garmo H, et al. Radical prostatectomy or watchful waiting in early prostate cancer. N Engl J Med 2014;370(10):932-942.
- Hamdy FC, Donovan JL, Lane JA, et al. Fifteen-Year Outcomes after Monitoring, Surgery, or Radiotherapy for Prostate Cancer. N Engl J Med. 2023 Apr 27;388(17):1547-1558.
- Ajjawi I, Loeb S, Cooperberg MR, et al. Active surveillance or watchful waiting for intermediate-risk prostate cancer, 2010-2020. JAMA. 2024 Dec 17;332(23):2033-2036.
- Palmstedt E, Mansson M Hugosson J, Godtman RA, et al. Active surveillance for screen-detected low- and intermediate-risk prostate cancer: Extended follow-up up to 25 years in the GÖTEBORG-1 trial. Eur Urol. 2025 Oct;88(4):373-380.
- Petrelli F, Dottorini L, Parsani G, et al. Active surveillance in intermediate-risk prostate cancer: A contemporary synthesis of evidence. Clin Genitourin Cancer. 2025 Oct;23(5):102407.
- Shee K, Pace WA, Song JJ, et al. A high Decipher genomic risk score is associated with major pathological progression in patients undergoing active surveillance for prostate cancer. Eur Urol Oncol. 2026 Jan 30:S2588-9311(26)00027-1.