(UroToday.com) The 2026 AUA annual meeting featured the International Prostate Forum and a presentation by Dr. Karen Hoffman discussing the management of biochemical recurrence in 2026. Dr. Hoffman began by revisiting the historical evidence supporting adjuvant radiation therapy following radical prostatectomy. Landmark randomized trials, including SWOG 8794, EORTC 22911, and ARO 96-02, demonstrated that adjuvant radiation improved PSA failure outcomes, reduced locoregional recurrence, and decreased the need for subsequent salvage therapy in men with pT3 disease or positive surgical margins:
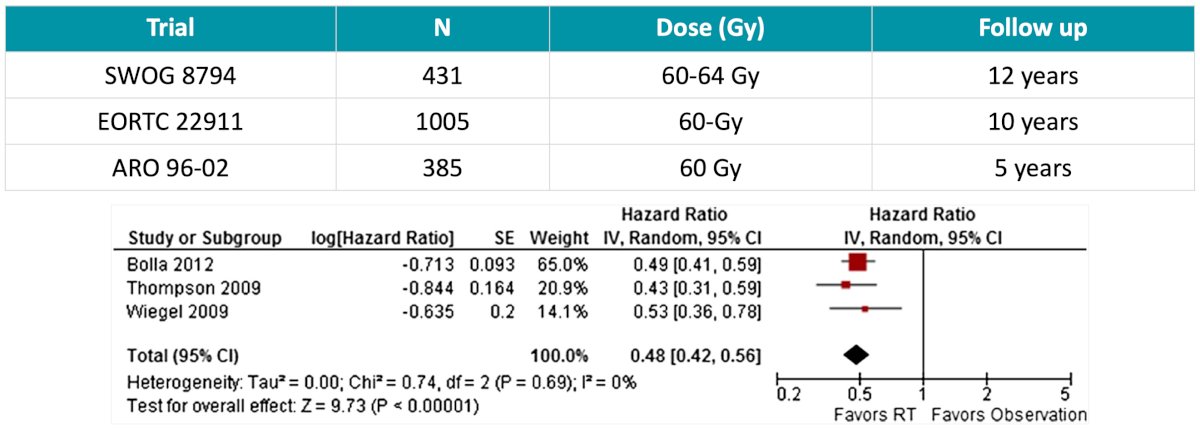
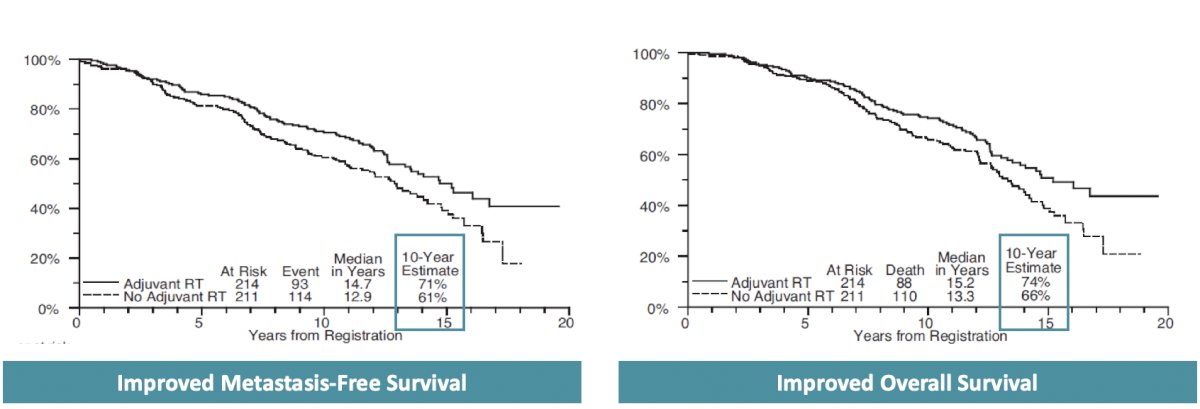
The SWOG trial demonstrated improvements in metastasis-free survival and overall survival, outcomes that were not replicated in the EORTC study:
However, Dr. Hoffman noted that adjuvant radiation therapy has important drawbacks, particularly treatment-related toxicity and overtreatment. Several studies have demonstrated higher rates of gastrointestinal and genitourinary toxicity among patients receiving adjuvant radiation compared to observation, including increased rates of urethral stricture and urinary incontinence. Furthermore, many of these earlier studies utilized delayed salvage treatment and often incorporated ADT at the time of relapse, making interpretation more challenging in the modern era:
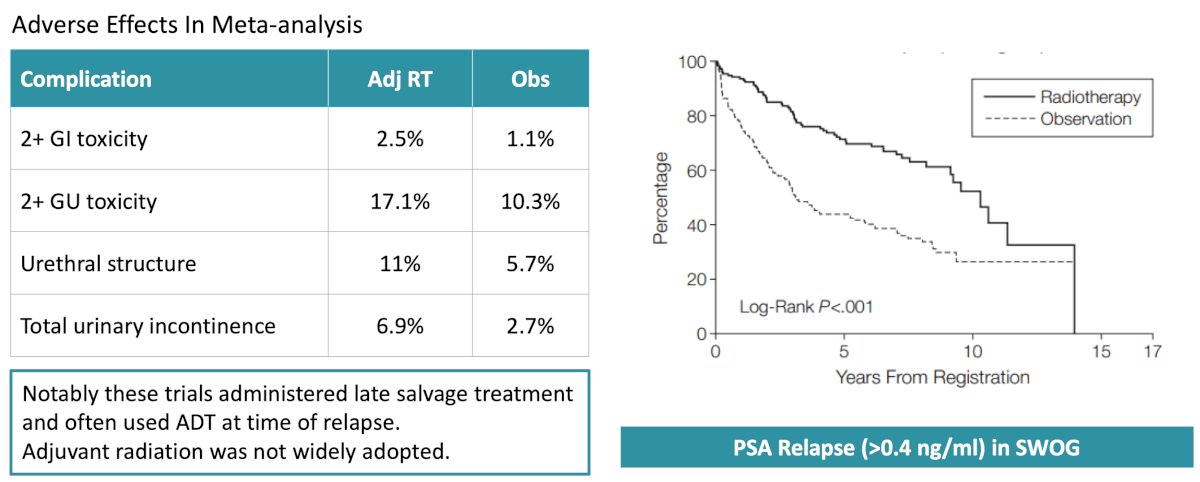
Because many patients would never recur following surgery alone, adjuvant radiation was never widely adopted.
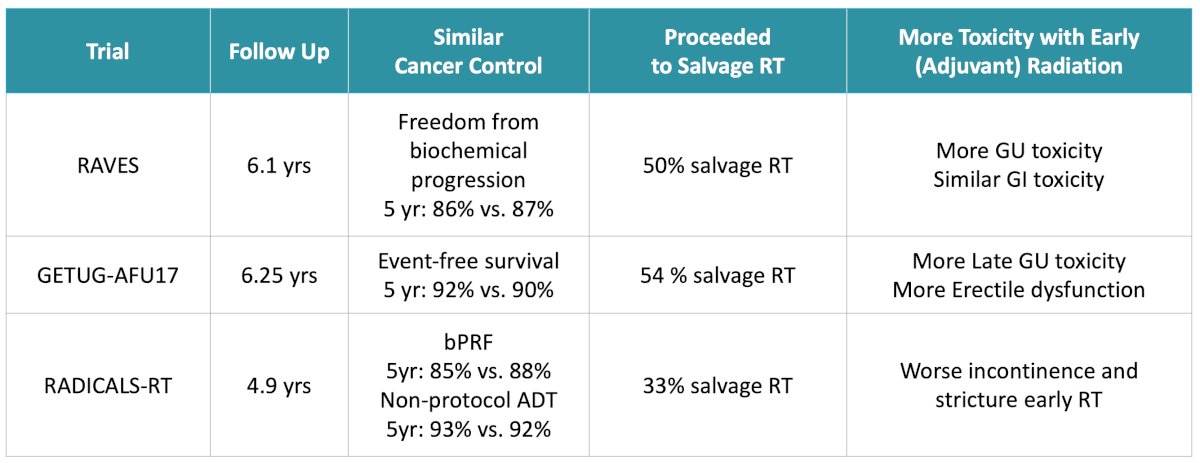
Dr. Hoffman then discussed modern randomized trials directly comparing adjuvant radiation with early salvage radiation. Dr. Hoffman reviewed the RAVES,1 GETUG-AFU17,2 and RADICALS-RT trials,3 each of which evaluated immediate postoperative radiation versus observation with salvage radiation initiated at low PSA thresholds:
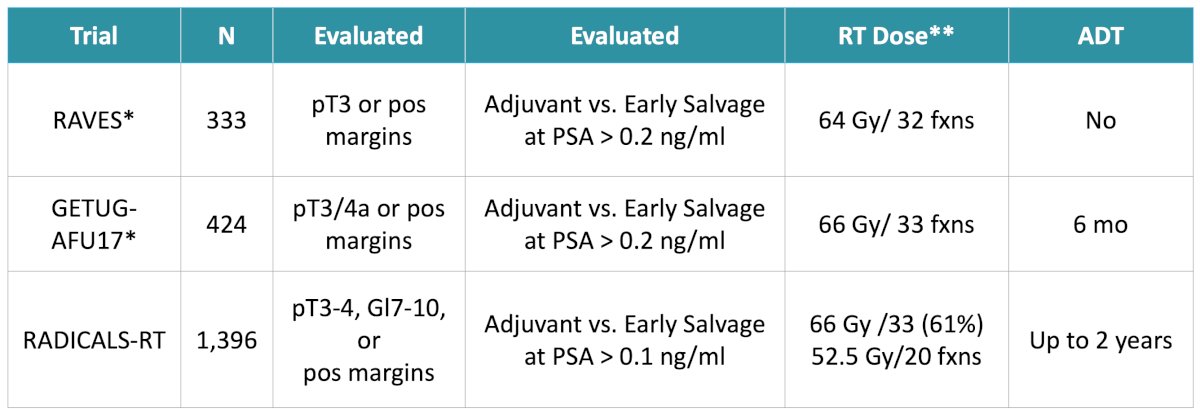
These studies consistently demonstrated similar oncologic outcomes between the two approaches. In RAVES, 5-year freedom from biochemical progression was 86% versus 87%, while GETUG-AFU17 demonstrated 5-year event-free survival rates of 92% versus 90%. RADICALS-RT similarly demonstrated nearly identical biochemical progression-free outcomes between adjuvant and early salvage approaches. Importantly, only 33% to 54% of patients assigned to observation ultimately required salvage radiation, supporting the notion that many men can safely avoid immediate postoperative therapy. Dr. Hoffman also emphasized that early salvage therapy was associated with lower toxicity compared to adjuvant treatment. RAVES demonstrated reduced genitourinary toxicity, GETUG-AFU17 showed lower rates of late genitourinary toxicity and erectile dysfunction, and RADICALS-RT demonstrated less incontinence and urethral stricture formation with delayed treatment:
The ARTISTIC collaborative meta-analysis pooled data from these modern postoperative radiation trials.4 ARTISTIC demonstrated comparable 5-year event-free survival rates between adjuvant and early salvage therapy at 89% versus 88%, respectively:
![The ARTISTIC collaborative meta-analysis pooled data from these modern postoperative radiation trials [4]. ARTISTIC demonstrated comparable 5-year event free survival rates between adjuvant and early salvage therapy at 89% versus 88%, respectively:](/images/com-doc-importer/263-aua-2026/aua-2026-locally-advanced-and-recurrent-prostate-cancer-updates-management-of-biochemical-recurrence-in-2026/image-5.jpg)
Dr. Hoffman highlighted that these trials largely enrolled favorable risk patients, with only 16% harboring Gleason 8 or higher disease and only 20% demonstrating seminal vesicle involvement.
Despite the growing preference for early salvage radiation, select patients with very high-risk pathologic features may still benefit from adjuvant treatment. In 2021, Tilki et al.5 performed a multi-institutional analysis involving 26,118 patients with pT2-3N0 or N1M0 prostate cancer. Among men with adverse pathology (n = 2,424) — including pN1 disease, Grade Group 4 or 5 disease, or pT3/4 tumors — adjuvant radiation was associated with reduced all-cause mortality compared to early salvage therapy. This association persisted even when node-positive patients were excluded:
![Despite the growing preference for early salvage radiation, select patients with very high-risk pathologic features may still benefit from adjuvant treatment. In 2021, Tilki et al. [5] performed a multi-institutional analysis involving 26,118 patients with pT2-3N0 or N1M0 prostate cancer. Among men with adverse pathology (n = 2,424) — including pN1 disease, Grade Group 4 or 5 disease, or pT3/4 tumors — adjuvant radiation was associated with reduced all-cause mortality compared to early salvage therapy. This association persisted even when node positive patients were excluded:](/images/com-doc-importer/263-aua-2026/aua-2026-locally-advanced-and-recurrent-prostate-cancer-updates-management-of-biochemical-recurrence-in-2026/image-6.jpg)
Dr. Hoffman summarized the postoperative radiation timing data by concluding that:
- Early salvage radiation is appropriate for most patients
- Patients with high-risk disease (pN1) can be counseled about the risks and potential benefits of adjuvant radiation
- Adjuvant radiation can be considered for patients whose disease does not reliably produce PSA and has adverse pathologic features
- Urinary function should be optimized prior to initiation of postoperative radiation therapy
Next, Dr. Hoffman discussed the role of ADT in combination with salvage radiation. Dr. Hoffman reviewed three pivotal randomized trials: GETUG-AFU16,6 RTOG 9601,7 and RTOG 0534 SPPORT:8
![Next, Dr. Hoffman discussed the role of ADT in combination with salvage radiation. Dr. Hoffman reviewed three pivotal randomized trials: GETUG-AFU16 [6], RTOG 9601 [7], and RTOG 0534 SPPORT:8](/images/com-doc-importer/263-aua-2026/aua-2026-locally-advanced-and-recurrent-prostate-cancer-updates-management-of-biochemical-recurrence-in-2026/image-7.jpg)
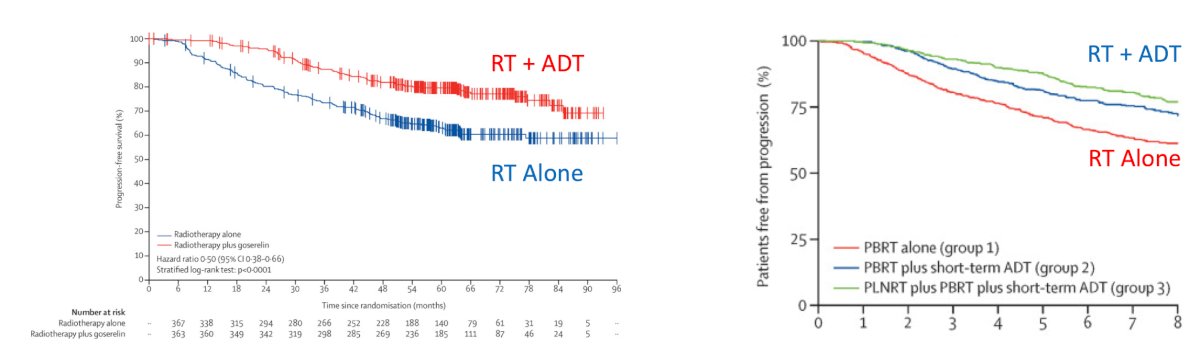
GETUG-AFU16 evaluated six months of goserelin combined with prostate bed radiation in men with detectable PSA recurrence following prostatectomy. At 10 years, the addition of ADT significantly improved progression-free survival (HR 0.54, p < 0.001) and metastasis-free survival (HR 0.73, p < 0.001):
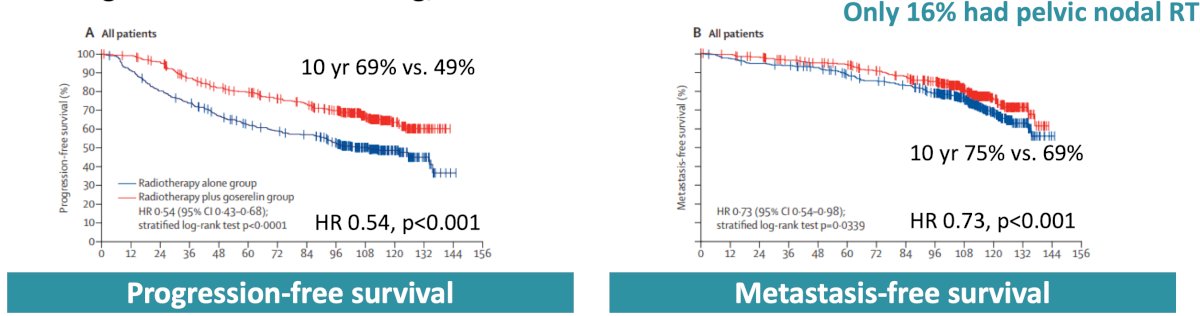
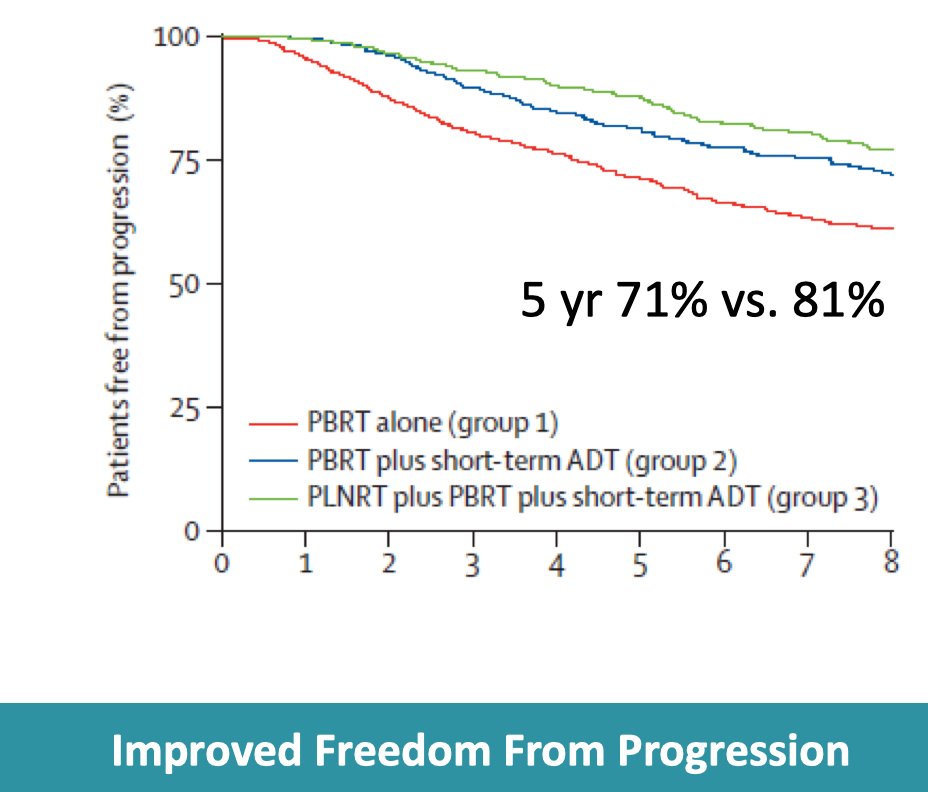
Improvements in progression-free survival were observed in both low-risk and high-risk subgroups, though no overall survival benefit was seen. Similarly, SPPORT demonstrated that 4-6 months of ADT improved freedom from progression among patients receiving salvage radiation:
Dr. Hoffman emphasized that these studies enrolled patients with relatively low median PSA levels of ~0.3 ng/mL, suggesting that even patients treated very early in the salvage setting may derive benefit from short-term ADT. Evan at low PSAs, adding ADT to postoperative radiation can provide benefit:
- Improves biochemical progression-free survival and metastasis-free survival
- May eradicate micrometastatic disease not addressed by radiotherapy alone
- Provides radiosensitization → improved local control
- Potential to delay initiation of long-term/lifelong ADT
- May reduce PSA-related anxiety
- Provides a sense of maximal upfront therapy (“do everything possible”)
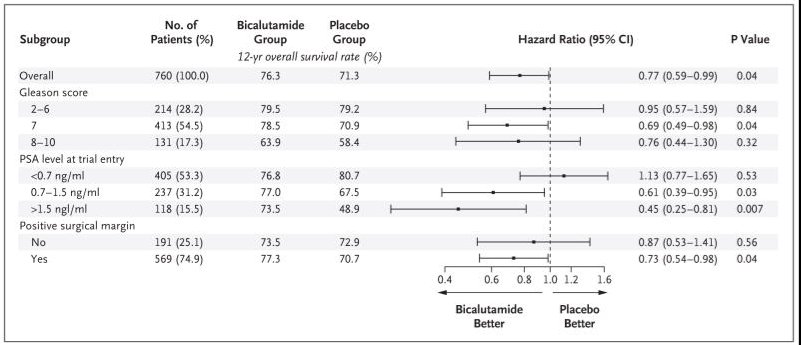
Dr. Hoffman then discussed the RTOG 9601 trial, which demonstrated improved overall survival (HR 0.77, 95% CI 0.59-0.99) and reduced prostate cancer mortality (HR 0.49, 95% CI 0.32-0.74) with the addition of two years of bicalutamide to salvage radiation:
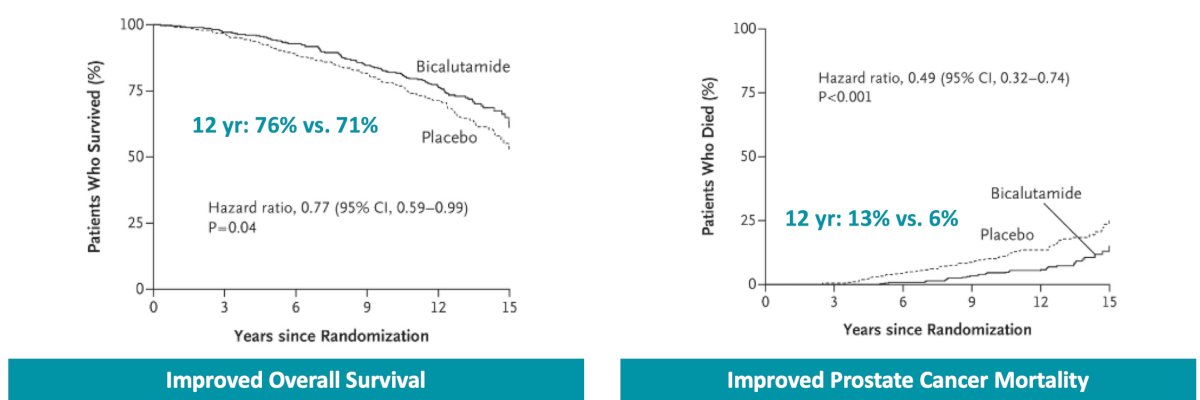
However, subgroup analyses revealed that patients with PSA values < 0.7 ng/mL did not derive an overall survival benefit from prolonged ADT:
Dr. Hoffman also discussed the recent POSEIDON meta-analysis from the MARCAP consortium, which pooled data from 6,057 patients evaluating the addition of ADT to postoperative radiation therapy. The analysis suggested that adding ADT did not improve overall survival among patients with PSA values ≤0.5 ng/mL:
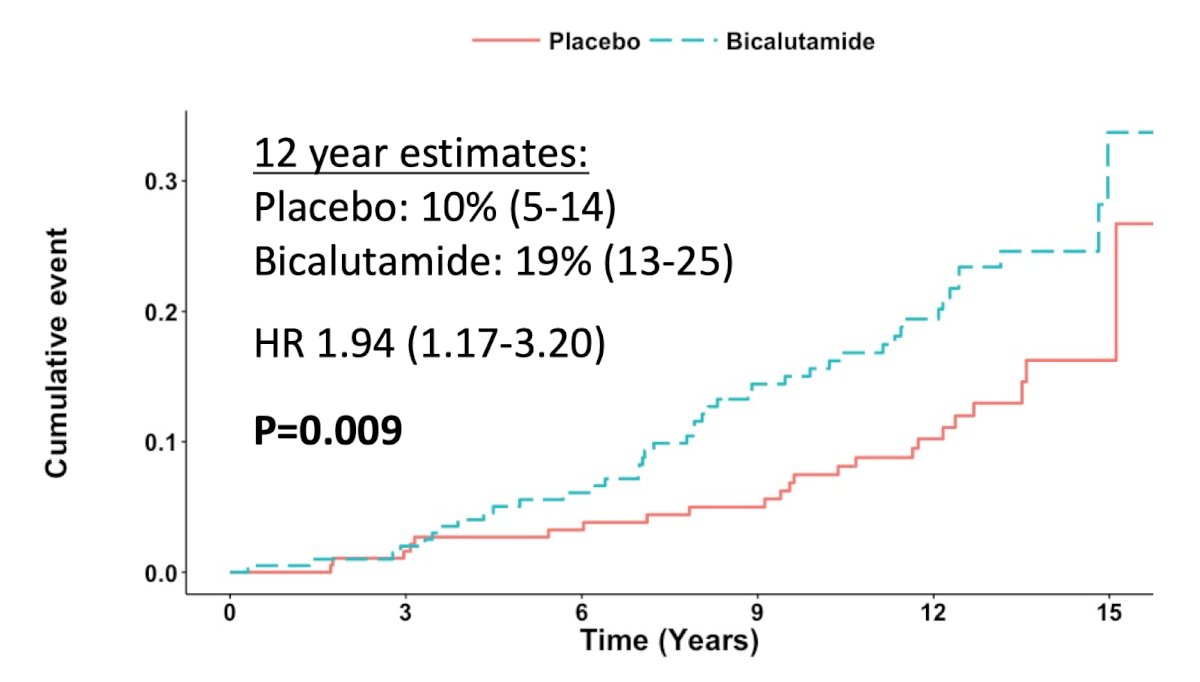
However, Dr. Hoffman cautioned that these results were heavily influenced by RTOG 9601, particularly the prolonged exposure to high-dose bicalutamide. Secondary analyses from RTOG 9601 demonstrated increased other cause mortality among patients with PSA values between 0.2-0.6 ng/mL treated with two years of bicalutamide (HR 1.94, 95% CI 1.17-3.20):
Dr. Hoffman provided the following context for the POSEIDON meta-analysis:
- POSEIDON may underestimate the benefit of ADT since results were heavily influenced by RTOG 9601
- Individual trials with median PSAs of 0.3 ng/ml demonstrate biochemical progression-free survival and metastasis-free survival benefits from the addition of short-term ADT
- Genomic classifiers will help us determine who truly needs ADT
- It is important to investigate less toxic androgen axis therapy in this space
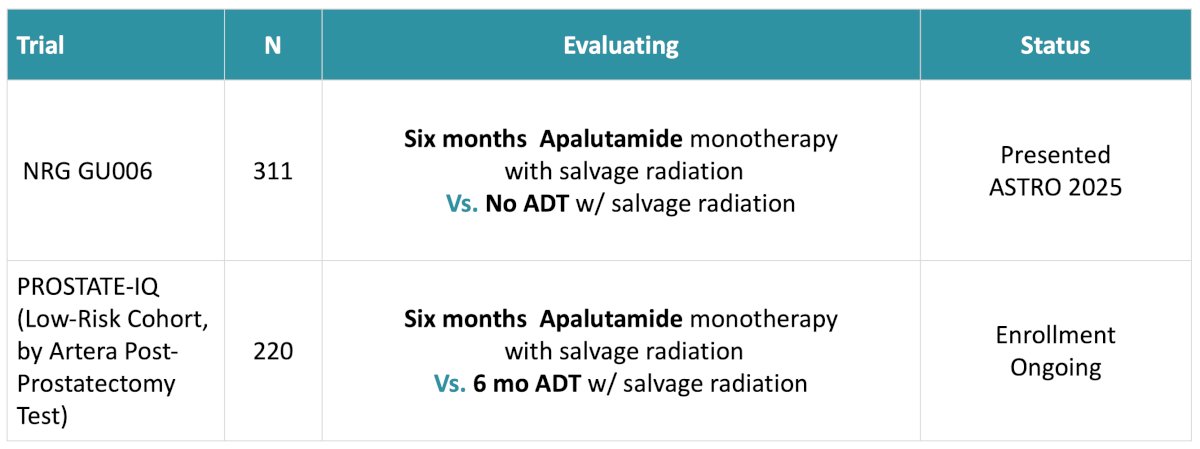
Both the NRG GU006 and PROSTATE-IQ trials are evaluating alternative ADT options that may have less toxicity in combination with salvage radiation:
ADT is not required for all patients. In GETUG-16, approximately 50% of patients treated with radiation alone remained recurrence-free at 10 years, while in SPPORT, approximately 70% remained recurrence-free at 5 years without ADT:
These findings underscore the importance of improved biomarkers capable of identifying patients most likely to benefit from hormonal intensification.
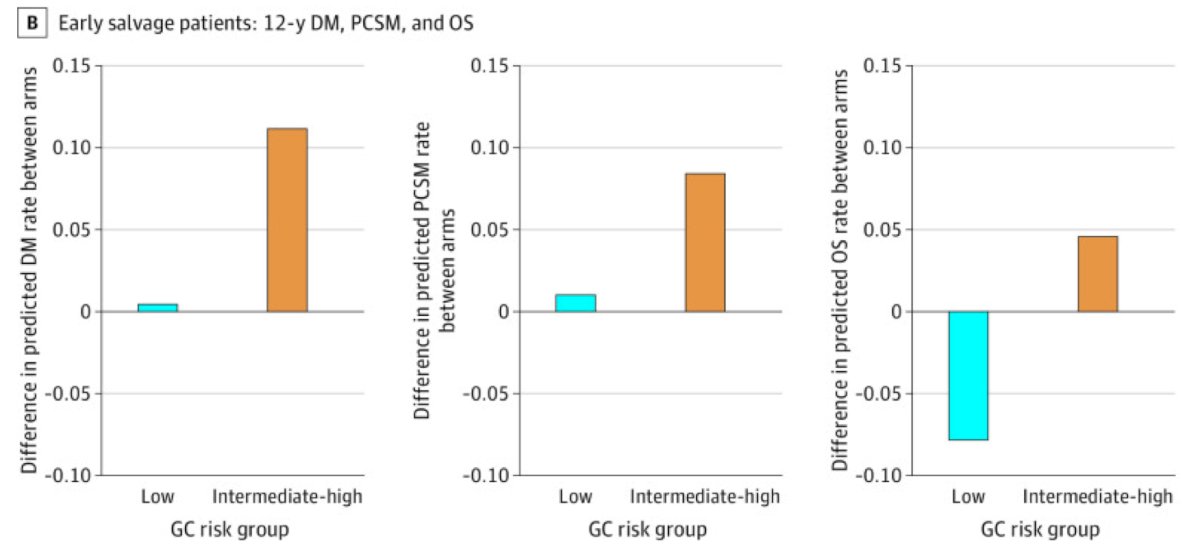
Dr. Hoffman then transitioned to genomic classifiers and biomarker-driven treatment personalization. First, RTOG 9601 demonstrated that the Decipher genomic classifier independently predicted distant metastasis, prostate cancer mortality, and overall survival:
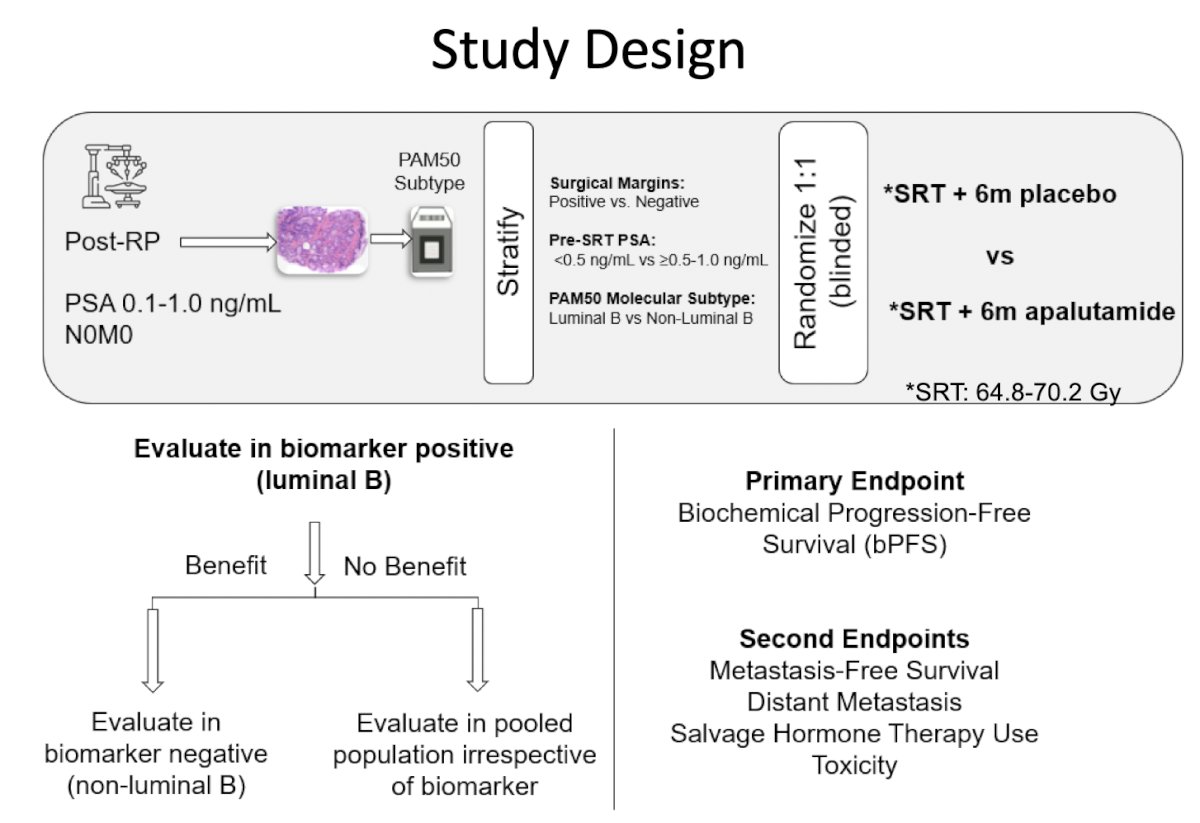
Second, the NRG GU006 trial prospectively evaluated the PAM50 molecular subtype, initially presented at ASTRO 2025. PAM50 classifies tumors into luminal and basal subtypes, adapted from breast cancer biology. NRG GU006, a phase II biomarker-stratified randomized trial of patients receiving salvage radiotherapy with or without apalutamide, was designed with the hypothesis that transcriptionally defined molecular subtypes would differentially benefit from apalutamide. Patients were enrolled between April 2018 – February 2020 and were required to be post-radical prostatectomy with a PSA 0.1-1.0 ng/mL without evidence of nodal or distant metastasis and randomized to salvage radiotherapy with placebo or apalutamide 240 mg daily for 6 months. Patients were stratified by PAM50 molecular subtype (luminal B versus non-luminal B):
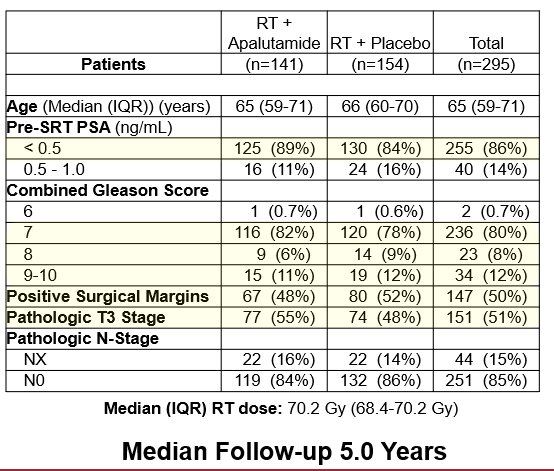
A total of 295 eligible patients were enrolled with a median follow-up of 5.0 years. The arms were well balanced, with a median age of 65 years (IQR 59-71), 50% with positive surgical margins, 51% with pathologic T3 disease, and 86% with entry PSA of <0.5 ng/mL. There were 20% of patients with grade group 4-5 prostate cancer:
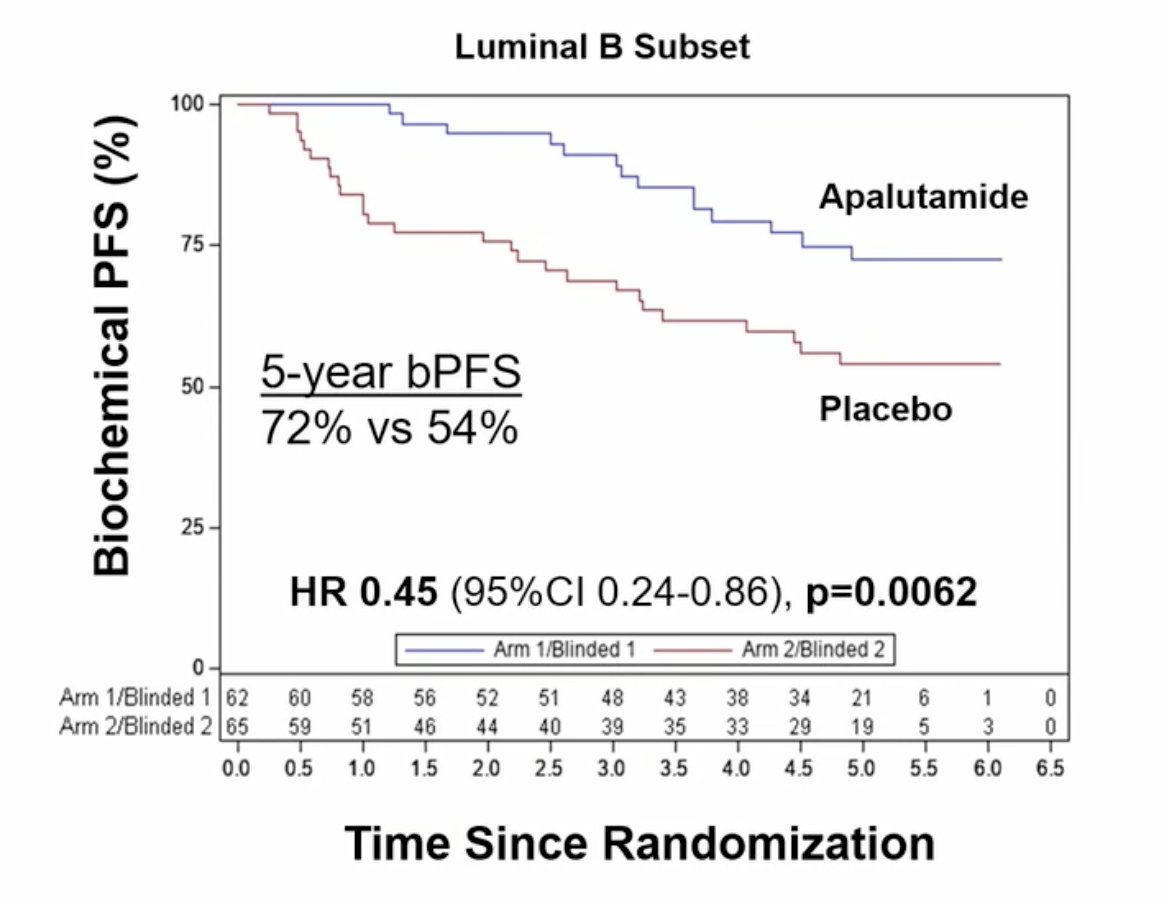
In luminal B patients, apalutamide significantly improved biochemical progression-free survival (HR 0.45, 80% CI 0.29-0.68, one-sided p = 0.0062), with 5-year estimated biochemical progression-free survival of 72% versus 54% in the apalutamide and placebo arms, respectively:
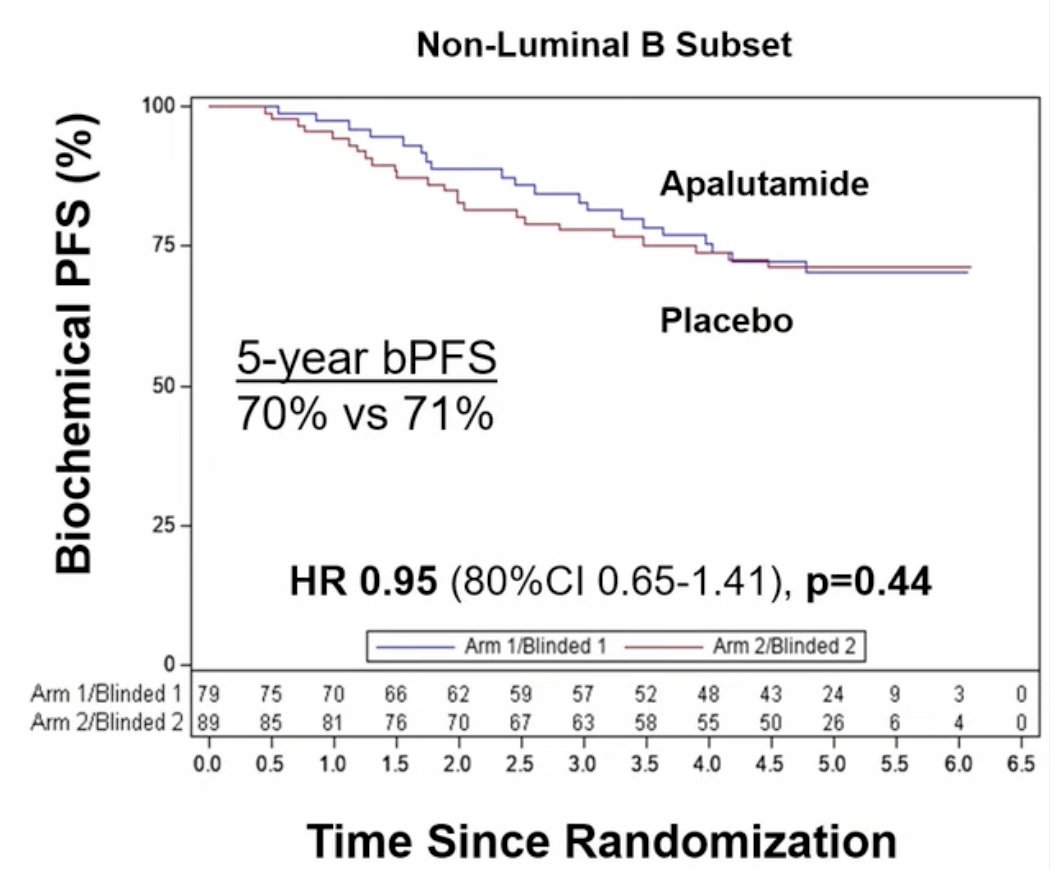
In contrast, non-luminal B patients did not demonstrate improvement in biochemical progression-free survival (HR 0.95, 80% CI 0.65-1.41, p = 0.44), with 5-year estimated biochemical progression-free survival of 70% versus 71%, although the lower CI limit was <0.77:
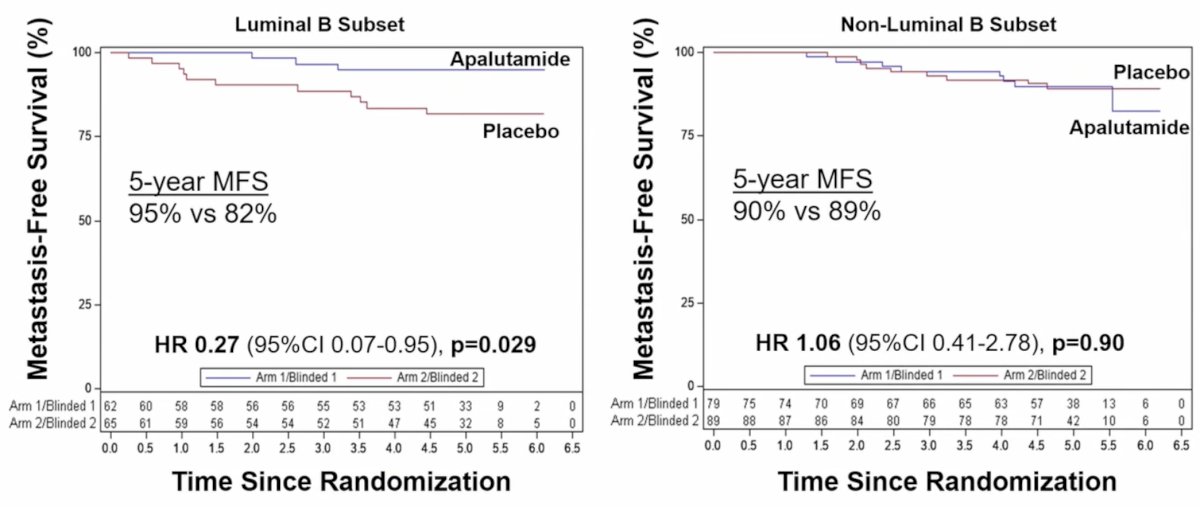
Metastasis-free survival was also improved with apalutamide in luminal B patients (HR 0.27, 95% CI 0.07-0.95, p = 0.029; 5-year estimates of 95% versus 82%), but not in non-luminal B patients (HR 1.06, 95% CI 0.41-2.78, p=0.90; 5-year estimates of 90% versus 89%):
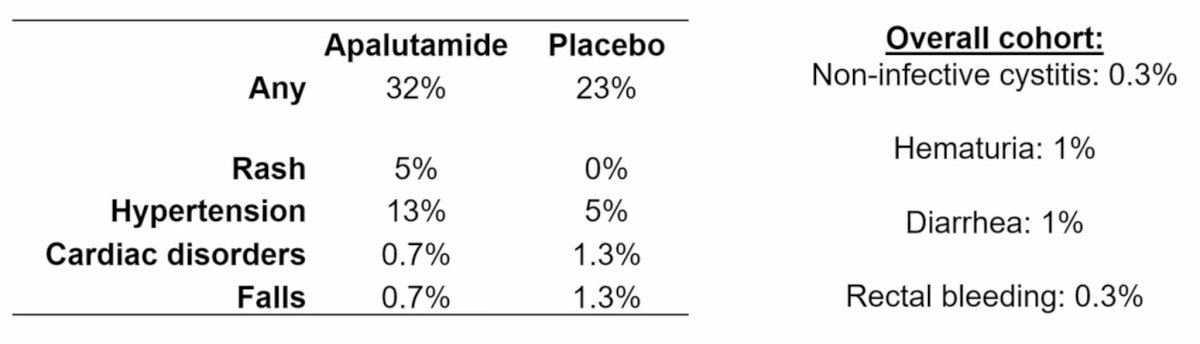
In the apalutamide versus placebo arm (regardless of attribution), grade 3+ gastrointestinal toxicity occurred in 5.7% versus 2.6%, and genitourinary toxicity in 3.5% versus 4.5%, respectively. In the apalutamide arm, grade 3+ rash occurred in 5% of patients and breast pain in 0.7%:
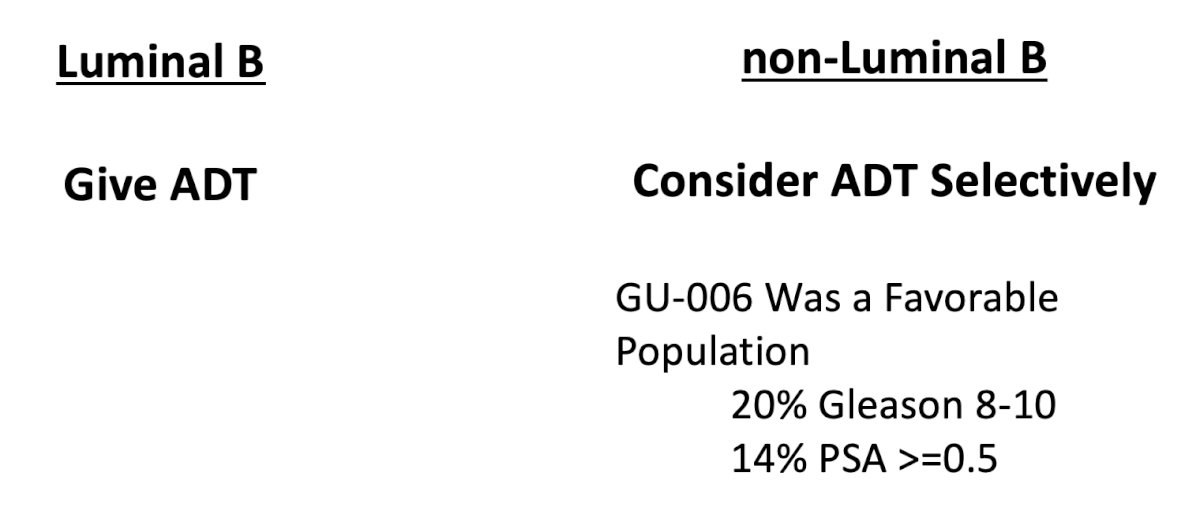
As such, PAM50 is the first advanced biomarker prospectively validated in a biomarker-driven clinical trial in non-metastatic prostate cancer. By comparison, all tools we currently use in the clinic were either validated in retrospective cohorts or had post-hoc validation in prospective trials. Dr. Hoffman notes that this trial should impact how we give ADT. For patients with a PSA < 1.0 ng/mL:
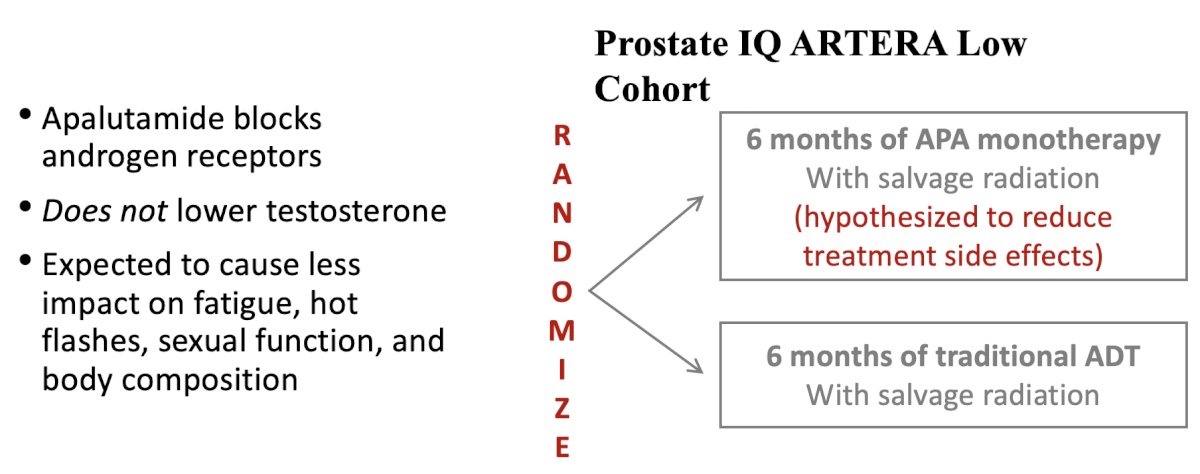
Importantly, NRG GU006 also supports the use of apalutamide monotherapy in the postoperative setting. Unlike traditional ADT, apalutamide blocks androgen receptors without lowering testosterone levels, theoretically reducing fatigue, hot flashes, sexual dysfunction, and body composition changes. Future directions, including the ongoing PROSTATE-IQ trial evaluating apalutamide monotherapy versus traditional ADT in lower-risk patients identified using the ArteraAI post-prostatectomy test:
Should PAM50 be used in other disease settings? Not yet, future work is needed to understand the performance of PAM50 in recurrent prostate cancer with PSAs > 1.0 or with nodal involvement, in localized prostate cancer, and oligometastatic prostate cancer.
Dr. Hoffman subsequently reviewed intensified systemic therapy approaches for higher-risk patients:
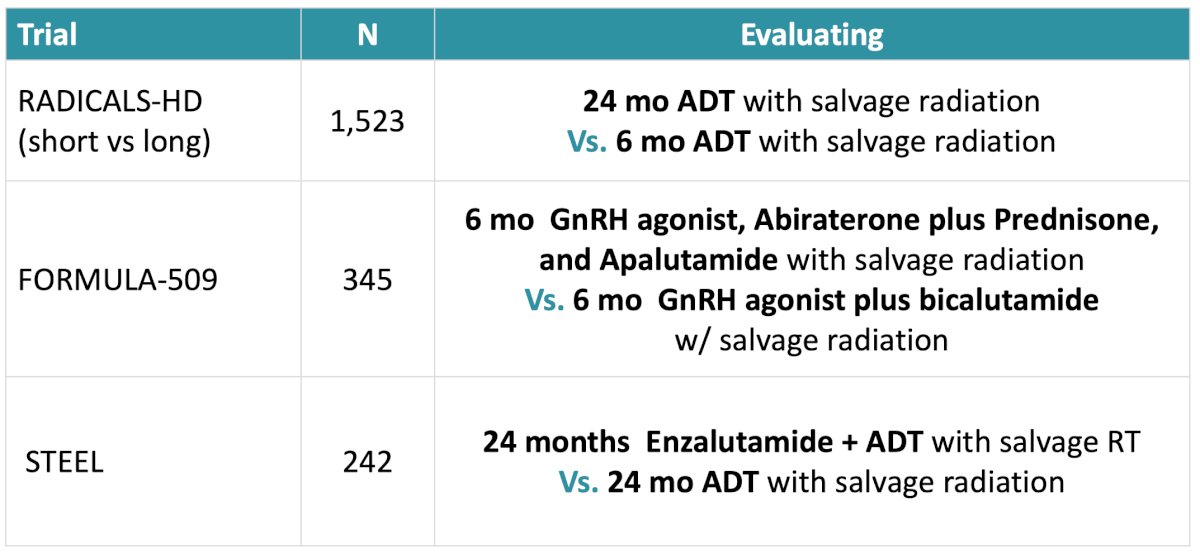
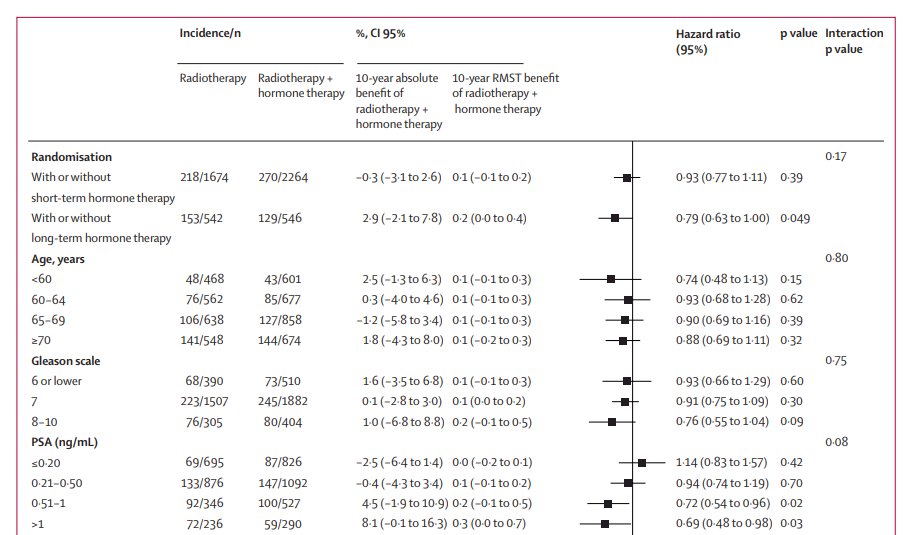
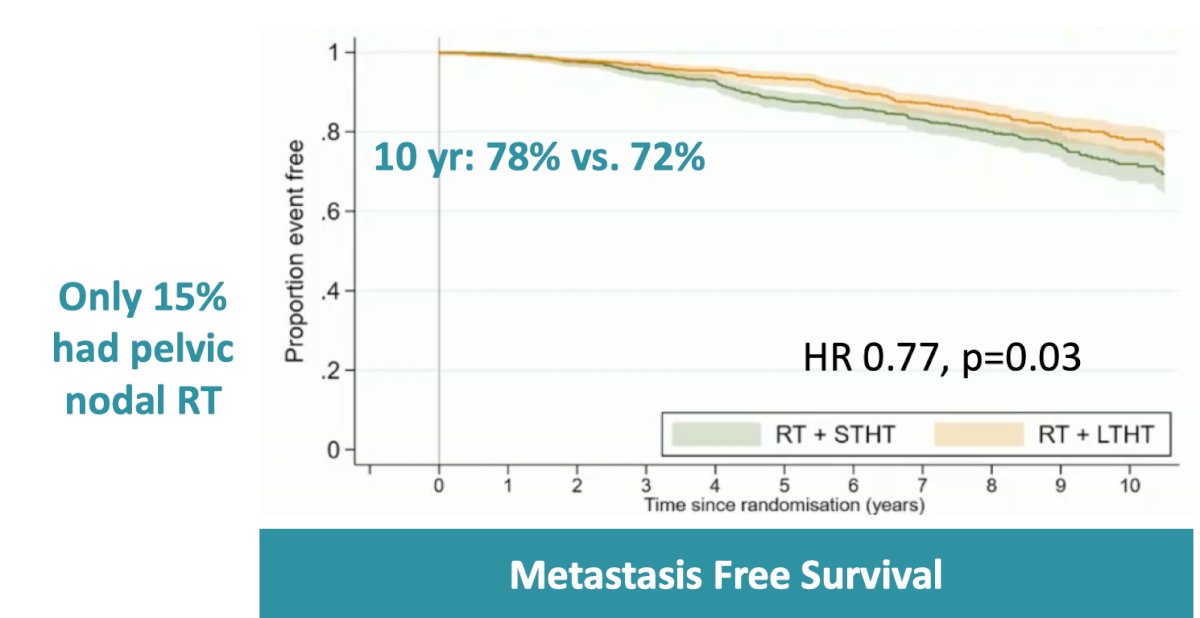
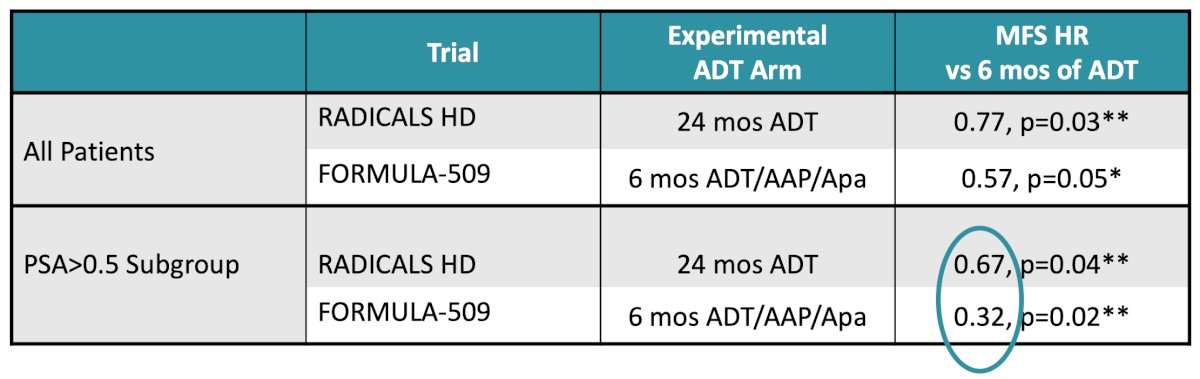
Presented at ESMO 2022, RADICALS-HD compared 24 months versus 6 months of ADT and demonstrated improved metastasis-free survival with prolonged hormonal therapy (HR 0.77, p = 0.03):
FORMULA-509 evaluated intensified therapy using abiraterone, prednisone, and apalutamide in addition to salvage radiation. Although the overall cohort did not achieve statistical significance, patients with PSA values greater than 0.5 ng/mL demonstrated marked improvements in progression-free and metastasis-free survival:
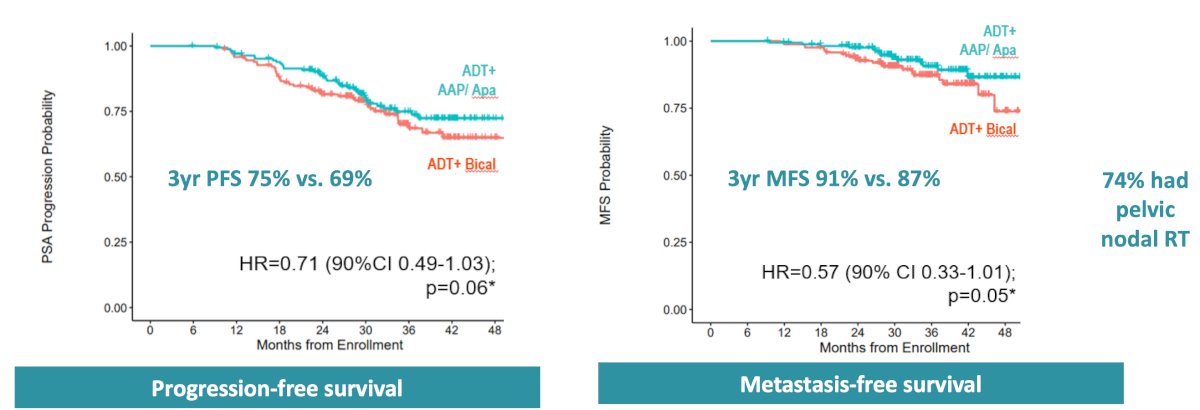
Notably, FORMULA-509 patient-reported outcomes demonstrated no major differences in hormonal function, fatigue, or cognitive function despite treatment intensification. Dr. Hoffman suggested that comparisons between FORMULA-509 and RADICALS-HD raise the possibility that shorter duration intensified therapy may provide superior disease control while reducing treatment burden:
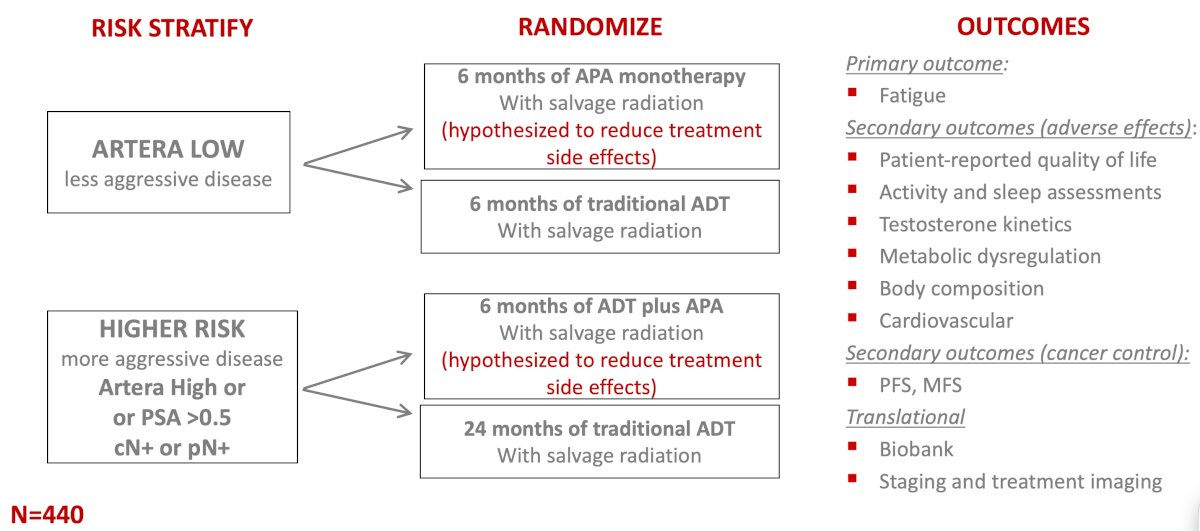
The ongoing PROSTATE-IQ trial was also highlighted as a study comparing the “winning arms” from RADICALS-HD and FORMULA-509 using ArteraAI risk stratification:
Dr. Hoffman summarized this section on administering ADT with salvage radiation therapy:
- Take into account patient age, comorbidities, and disease aggressiveness
- Dr. Hoffman typically gives 6 months of ADT to most patients
- After counseling about side effects and the expected incremental benefit
- Anticipate using once PAM50 is commercially available
- Usually, we can omit ADT for the most favorable patients
- Gleason 7, positive margins, low PSA
- Always give in the context of pelvic nodal treatment
- Consider intensifying ADT by adding a second-generation anti-androgen for patients with PSA >0.5 (though trial enrollment preferred)
With regards to pelvic nodal radiation, updated SPPORT data demonstrated improved progression-free survival with the addition of pelvic nodal radiation, though at the cost of increased grade 2+ acute gastrointestinal and bone marrow toxicity:

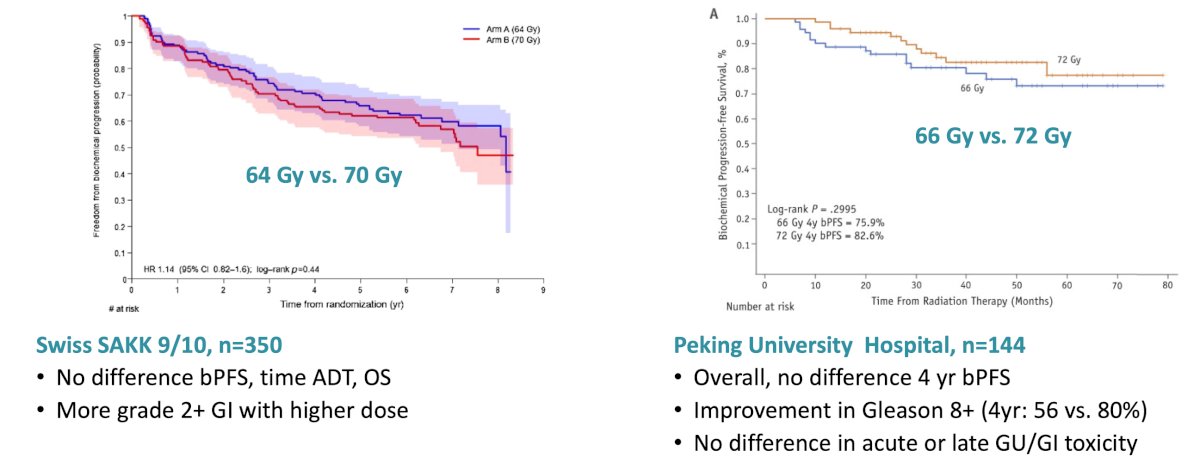
Dr. Hoffman also reviewed retrospective and randomized data evaluating salvage radiation dose escalation. Retrospective analyses suggested that doses ≥66 Gy may improve biochemical control. However, the SAKK 9/10 trial comparing 64 versus 70 Gy and a trial from the Peking University Hospital comparing 66 versus 72 Gy demonstrated limited differences overall, with increased gastrointestinal toxicity observed in some higher-dose cohorts:
With regards to hypofractionation, NRG GU003 demonstrated similar physician-reported and patient-reported toxicity between conventional and hypofractionated salvage radiation approaches:
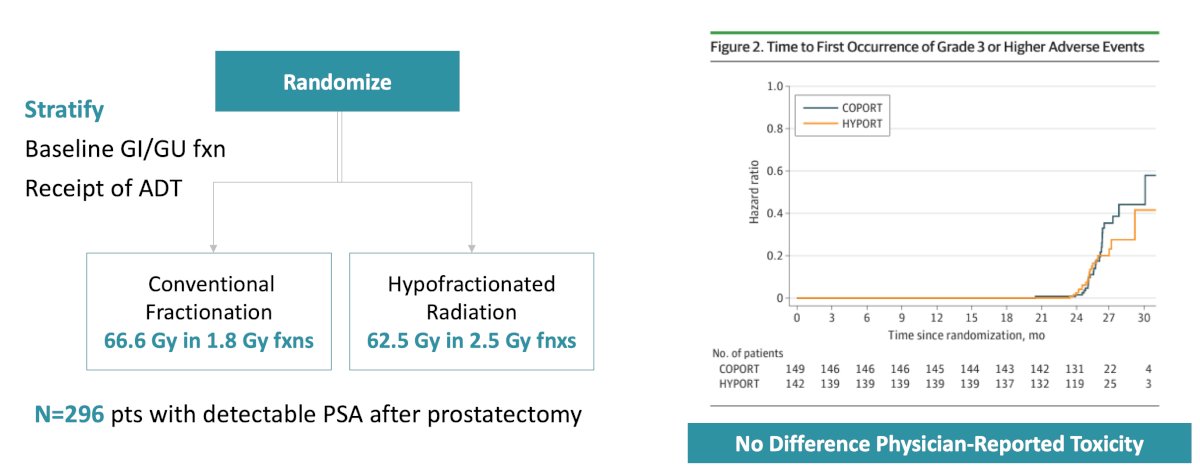
Similarly, RADICALS-RT demonstrated favorable early and late toxicity with hypofractionated treatment. Dr. Hoffman concluded the salvage radiation dose and technique section with the following key takeaways:
- 64-72 Gy to the prostate bed is appropriate
- Dr. Hoffman uses 66 to 70 Gy
- Possible higher dose to gross recurrences
- Dr. Hoffman uses a simultaneous integrated boost of 72.5-73.5 Gy over 35 fractions
- Adjuvant pelvic nodal radiation can improve cancer control
- Dr. Hoffman favors this approach for Gleason 8-10, limited nodal dissection, or PSA 0.4 and higher
- Hypofractionation
- Dr. Hoffman currently treats post-op hypofractionation on trial
The final part of the presentation focused on molecular imaging. The EMPIRE-1 study demonstrated that molecular imaging with 18F-fluciclovine PET altered radiation treatment planning in approximately 35% (28/79) of patients with biochemical recurrence and negative conventional imaging.10 Molecular imaging-guided treatment also improved 3-year event-free survival (63% versus 76%) compared to conventional imaging-directed radiation:
![The final part of the presentation focused on molecular imaging. The EMPIRE-1 study demonstrated that molecular imaging with 18F-fluciclovine PET altered radiation treatment planning in approximately 35% (28/79) of patients with biochemical recurrence and negative conventional imaging [10]. Molecular imaging guided treatment also improved 3-year event free survival (63% versus 76%) compared to conventional imaging-directed radiation:](/images/com-doc-importer/263-aua-2026/aua-2026-locally-advanced-and-recurrent-prostate-cancer-updates-management-of-biochemical-recurrence-in-2026/image-33.jpg)
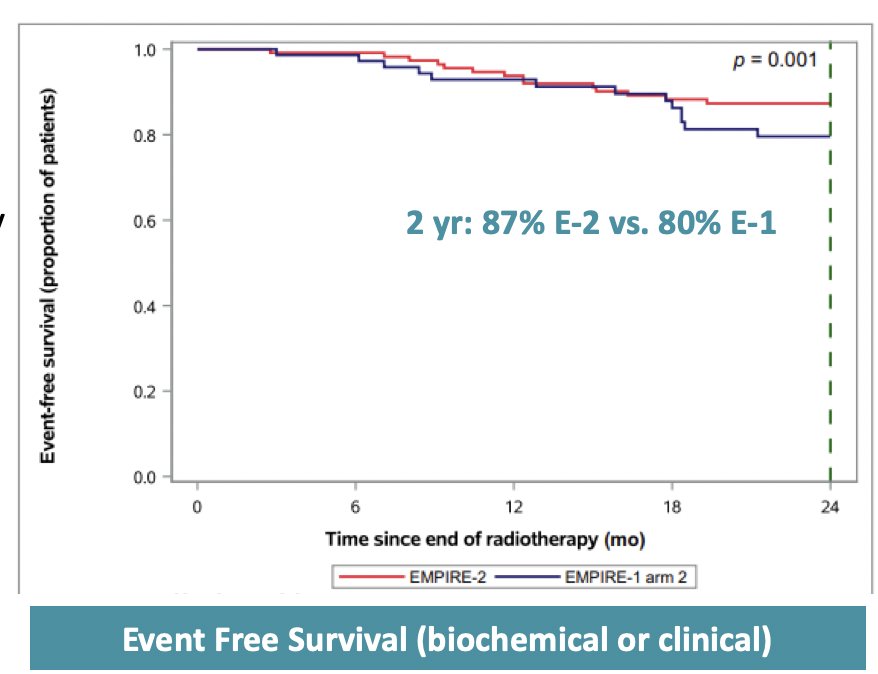
The EMPIRE-2 trial is evaluating PSMA PET-guided salvage radiation (pelvic nodes: 45-50.4 Gy/25-28 w/SIB of 56 Gy; prostate bed: 64.8-70.2 Gy/36-39 w/ SIB to 76 Gy) with dose-escalated image-guided treatment. PSMA PET-guided therapy improved 2-year event-free survival compared to prior fluciclovine-based approaches (87% in EMPIRE-2 versus 80% in EMPIRE-1):
Dr. Hoffman concluded her presentation discussing the management of biochemical recurrence in 2026 with the following take-home points:
- When administering ADT with salvage radiation, it is important to take into account patient age, comorbidities, and disease aggressiveness
- Genomic classifiers will help us determine who truly needs ADT
- Trials are investigating less toxic androgen axis therapy in this space
- 64-72 Gy to the prostate bed is appropriate; however, a lower dose may reduce toxicity
- Pelvic nodal radiation can improve cancer control
- Molecular imaging is preferred over biochemical recurrence to help define targets
Presented by: Karen Hoffman, MD, MHSc, MPH, FASTRO, The University of Texas, MD Anderson Cancer Center, Houston, TX
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
References:
- Kneebone A, Fraser-Browne C, Duchesne GM, et al. Adjuvant radiotherapy versus early salvage radiotherapy following radical prostatectomy (TROG 08.03/ANZUP RAVES): A randomized, controlled, phase 3, non-inferiority trial. Lancet Oncol. 2020;21(10):1331-1340.
- Sargos P, Chabaud S, Latorzeff I, et al. Adjuvant radiotherapy versus early salvage radiotherapy plus short-term androgen deprivation therapy in men with localized prostate cancer after radical prostatectomy (GETUG-AFU 17): A randomized, phase 3 trial. Lancet Oncol 2020;21(10):1341-1352.
- Parker CC, Clarke NW, Cook AD, et al. Timing of radiotherapy after radical prostatectomy (RADICALS-RT): A randomized, controlled phase 3 trial. Lancet 2020;396(10260):1413-1421.
- Vale CL, Fisher D, Kneebone A, et al. Adjuvant or early salvage radiotherapy for the treatment of localized and locally advanced prostate cancer: A prospectively planned systematic review and meta-analysis of aggregate data. Lancet 2020 Oct 31;396(10260):1422-1431.
- Tilki D, Chen MH, Wu J, et al. Adjuvant versus early salvage radiation therapy for men at high risk for recurrence following radical prostatectomy for prostate cancer and the risk of death. J Clin Oncol. 2021 Jul 10;39(20):2284-2293.
- Carrie C, Hasbini A, de Laroche G, et al. Salvage radiotherapy with or without short-term hormone therapy for rising prostate-specific antigen concentration after radical prostatectomy (GETUG-AFU 16): A randomized, multicentre, open-label phase 3 trial. Lancet Oncol 2016;17(6):747-756.
- Shipley WU, Seiferheld W, Lukka HR, et al. Radiation with or without Antiandrogen Therapy in Recurrent Prostate Cancer. N Engl J Med 2017;376(5):417-428.
- Pollack A, Karrison TG, Balogh AG, et al. The addition of androgen deprivation therapy and pelvic lymph node treatment to prostate bed salvage radiotherapy (NRG Oncology/RTOG 0534 SPPORT): An international, multicentre, randomized phase 3 trial. Lancet. 2022 May 14;399(10338):1886-1901.
- Feng FY, Huang HC, Spratt DE, et al. Validation of a 22-gene genomic classifier in patients with recurrent prostate cancer: An ancillary study of NRG/RTOG 9601 randomized clinical trial. JAMA Oncol. 2021 Apr 1;7(4):544-552.
- Jani AB, Schreibmann E, Goyal S, et al. 18F-fluciclovine-PET/CT imaging versus conventional imaging alone to guide postprostatectomy salvage radiotherapy for prostate cancer (EMPIRE-1): A single centre, open-label, phase 2/3 randomized controlled trial. Lancet. 2021 May 22;397(10288):1895-1904.