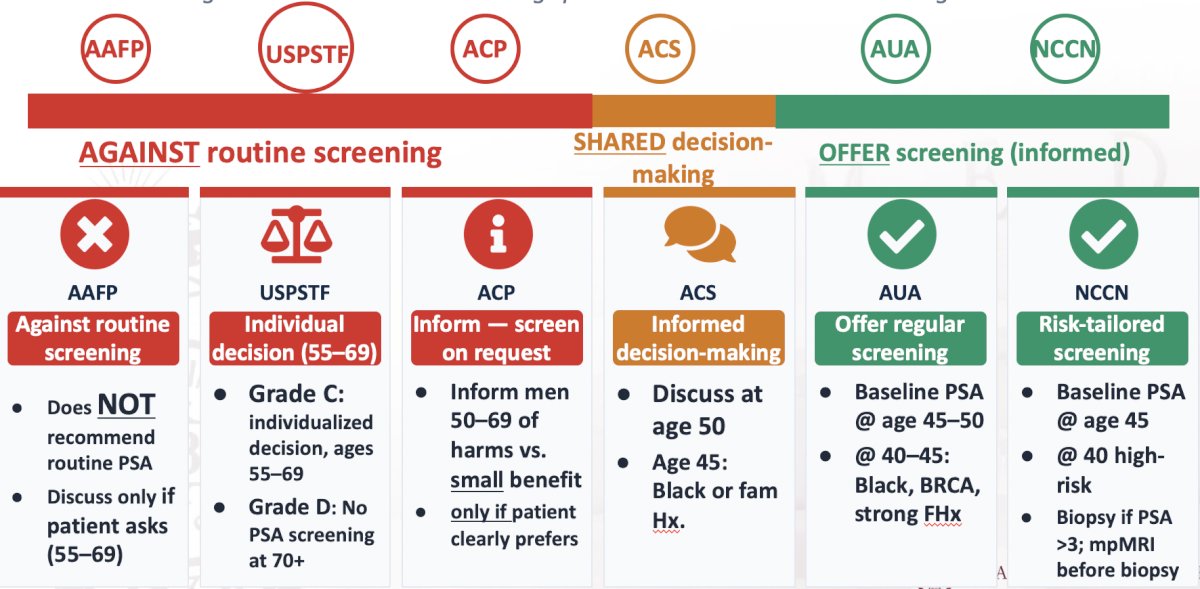
(UroToday.com) The 2026 AUA annual meeting featured the International Prostate Forum and a presentation by Dr. Badar Mian discussing guidelines, real-world practice, and recent evidence for prostate cancer screening, detection, and surveillance. Dr. Mian started his presentation by highlighting where each key organization in the United States sits on the PSA screening spectrum and what makes their guidance distinctive:
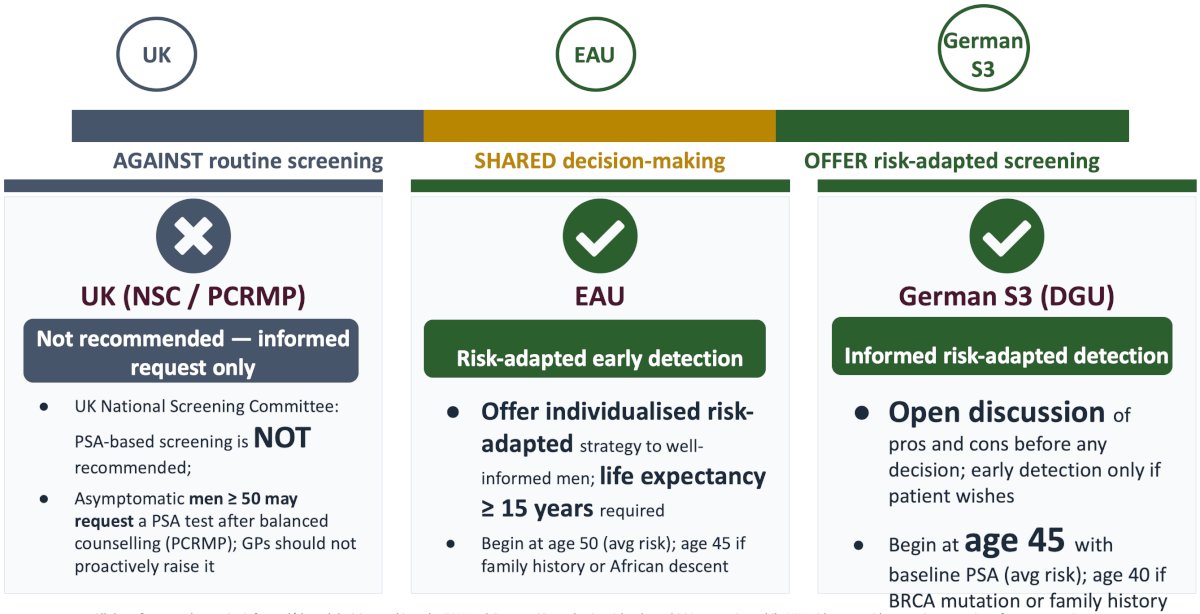
In Europe, there are also different perspectives compared to the United Kingdom, including the European Association of Urology (EAU), and the German S3 recommendations:
When we decide to start the prostate cancer screening process in the USA varies drastically between the AAFP, USPSTF, ACP, ACS, AUA, and NCCN:

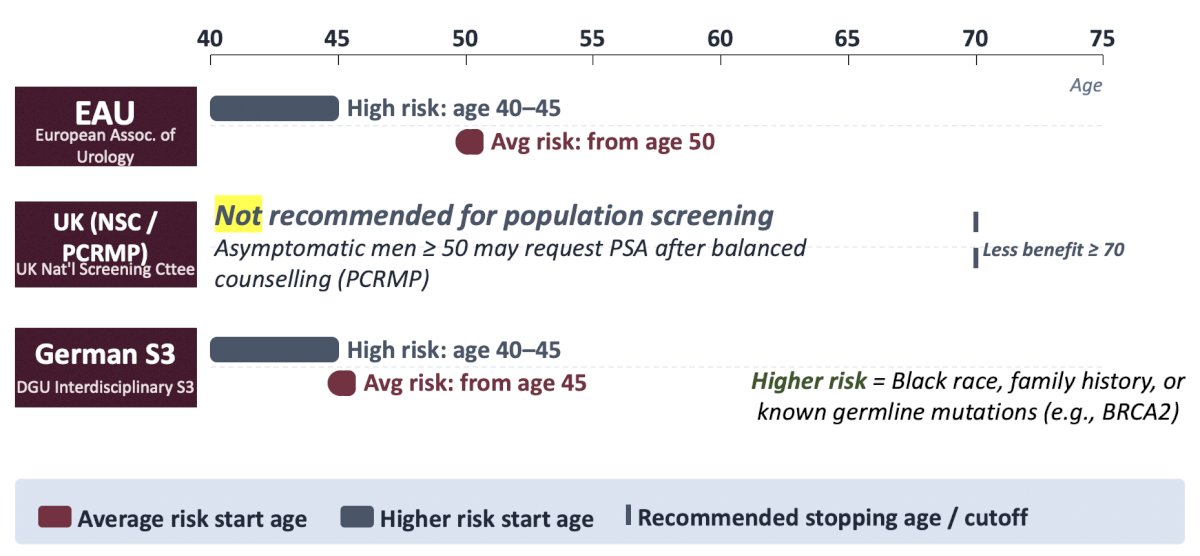
Similar variability in when to start prostate cancer screening in Europe is also noted:
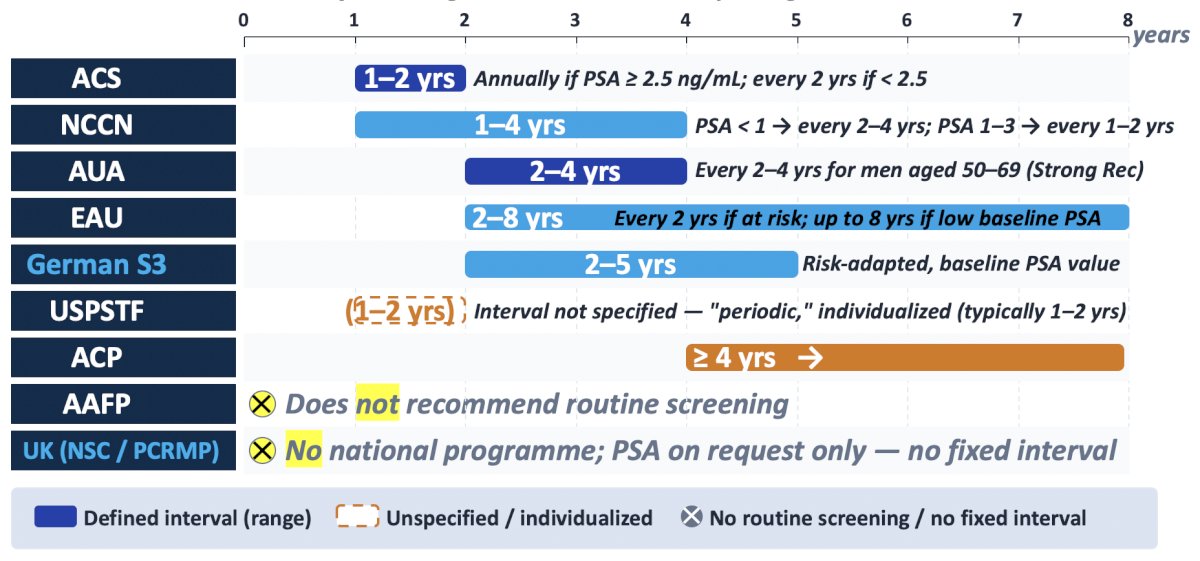
How often each guideline recommends repeat PSA testing also varies from 1-2 years (ACS) to 4+ years (ACP):
In the United Kingdom, there is no national prostate cancer screening program. PSA testing is opportunistic and general practitioner-mediated, governed by two parallel governing bodies. First, NICE covers symptomatic men only, using age-adjusted PSA thresholds for a 2-week wait referral:
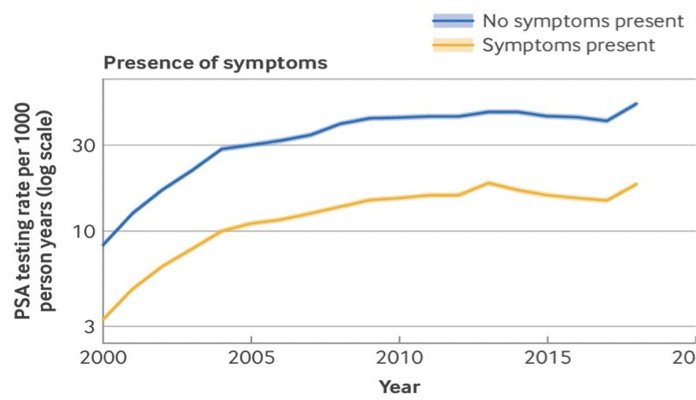
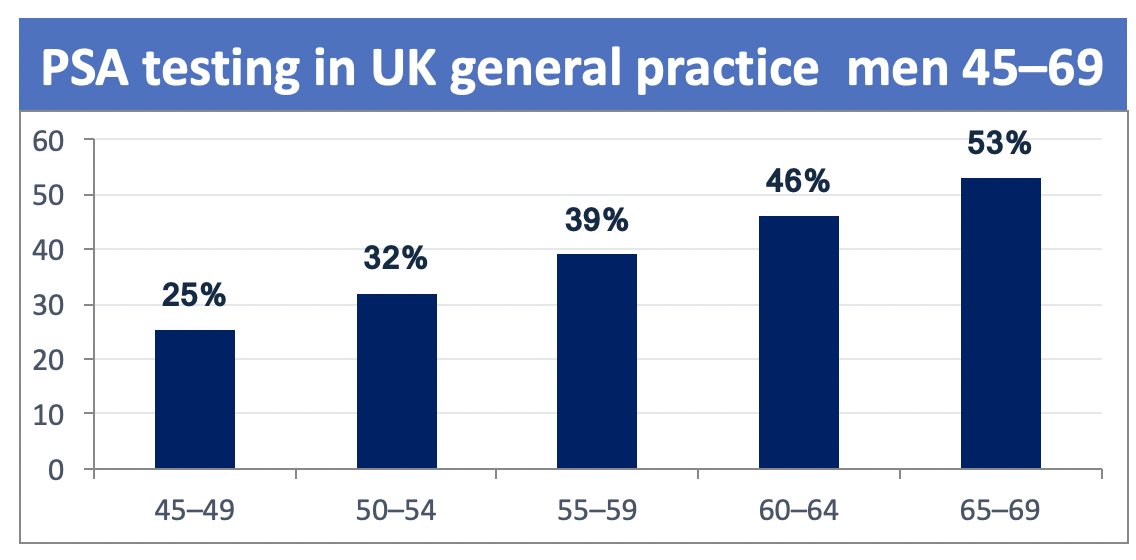
The second is the Prostate Cancer Risk Management Programme (PCRMP), where asymptomatic men aged 50+ can request a free NHS PSA test after counselling on harms and benefits, but general practitioners are explicitly told not to raise the screening proactively. Secondary to these screening practices in the United Kingdom, 63,000+ cases and 12,000 deaths per year are attributed to prostate cancer, the most commonly diagnosed cancer among men. In 2017, Young et al.1 performed a cross-sectional analysis of >430,000 men in the United Kingdom, noting a cumulative PSA screening rate increasing sharply with age, from 25% at 45–49 years to 53% at 65–69 years:
Dr. Mian notes that this level of testing is comparable in volume — though not in protocol — to organized screening. The annual cross-sectional PSA testing rate is ≈ 6%, and ≈ 2% in fully asymptomatic men. Thus, many United Kingdom PSA tests are prompted by lower-urinary tract symptoms rather than pure screening intent. In November 2025, the United Kingdom National Screening Committee published a draft recommendation against population-wide PSA screening, but proposed a targeted program (PSA every 2 years, ages 45–61) for men with confirmed BRCA1/BRCA2 variants.
In Germany, there is also no national PSA screening program; PSA is mainly self-paid as an Individuelle Gesundheitsleistung (IGeL). In an assessment of an insurance utilization review in Germany from 2009 to 2021, 20–30% of men aged 60–70 use any prostate early detection service annually, rising steadily by age: 
Use has been remarkably stable, varying only 1–2 percentage points across the decade. Surveys suggest that most German urologists believe PSA screening is helpful (87%), compared to only 52% of general practitioners. Of note, PSA testing is one of the most frequently offered elective (out-of-pocket) health services in Germany. Among the three data sources typically used to assess PSA screening trends in Germany, surveys have self-reporting bias, but do cover insured and non-insured behaviors. Insurance claims analyses are robust, but typically miss the IGeL and self-pay individuals using PSA screening, which is problematic given that the self-pay channel is the most commonly used in Germany. Finally, registries only capture the downstream effect of PSA screening (or not screening), not the test itself.
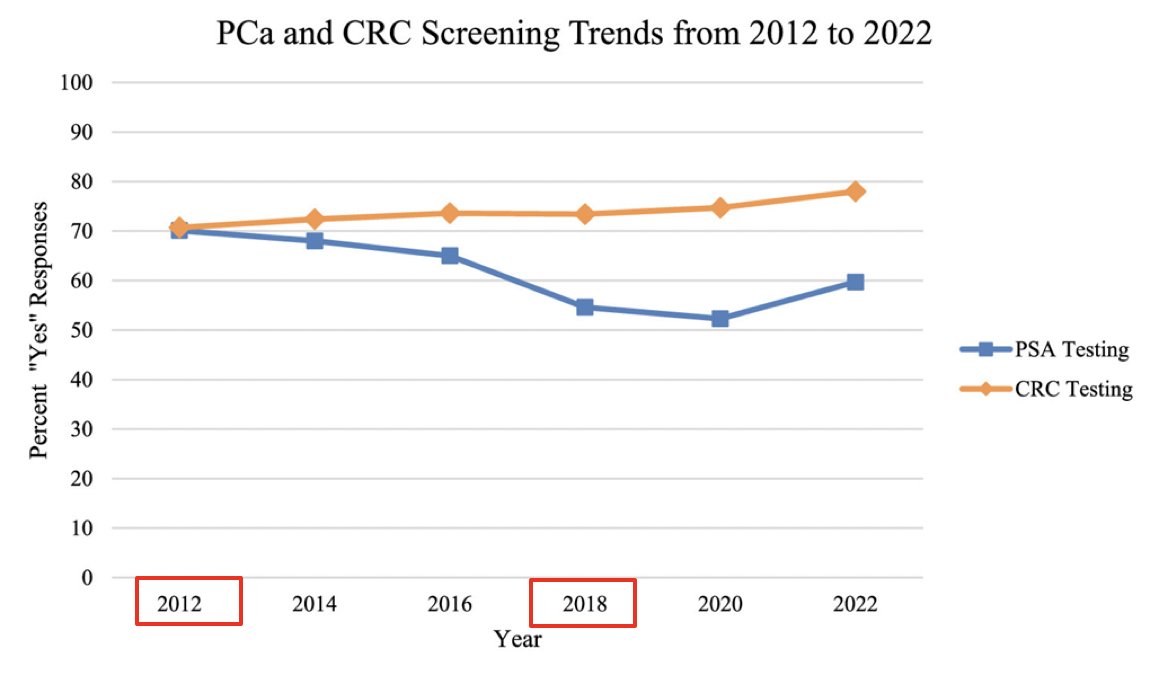
In the United States, in 2012, the USPSTF provided its recommendation for no PSA screening. Data from the CDC suggests that PSA testing declined after 2012, but also appears to have stabilized, albeit below the 2012 screening rates:
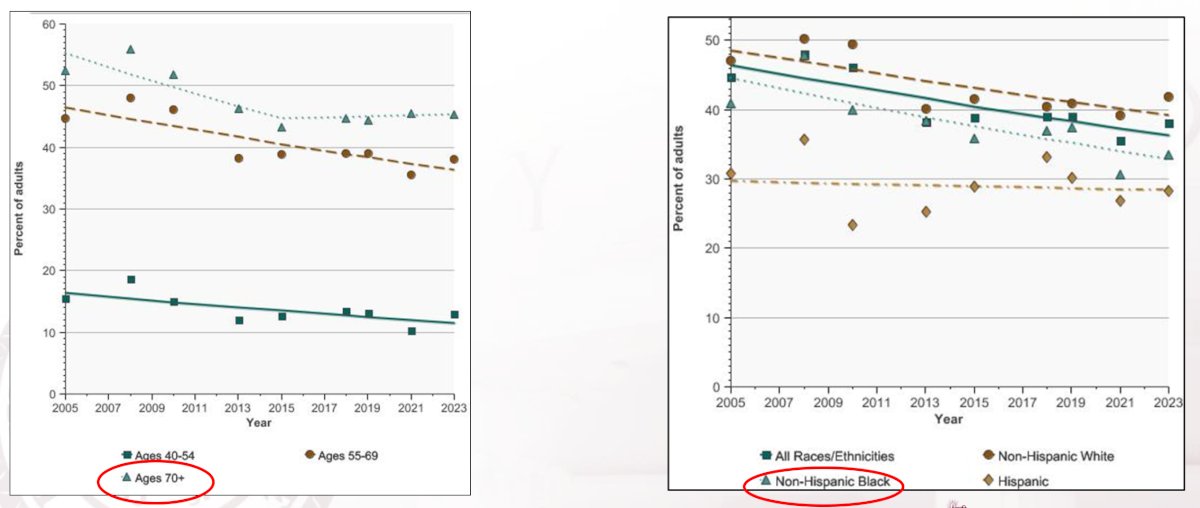
According to the NCI’s Cancer Trends Progress Report, from 2005 to 2023, PSA testing among men aged > 70 years was not decreasing, but unfortunately, for Black men, PSA testing was not increasing:
Two studies from the National Health Interview Survey assessing “discussing the pros/cons of PSA” testing2-3 – shared decision making – noted that 39.5% of practitioners discussed the advantages, and 25.6% discussed the disadvantages of PSA testing. Moreover, although Black men were more likely to discuss PSA advantages (OR 1.421, 95% CI 1.150-1.756, p = 0.001) and disadvantages (OR 1.554, 95% CI 1.240-1.947, p < 0.001) than White men, this did not correlate with higher rates of PSA screening (OR 1.086; 95% CI 0.865-1.364, p = 0.477):
![Two studies from the National Health Interview Survey assessing “discussing the pros/cons of PSA” testing [2-3] – shared decision making – noted that 39.5% of practitioners discussed the advantages, and 25.6% discussed the disadvantages of PSA testing. Moreover, although Black men were more likely to discuss PSA advantages (OR 1.421, 95% CI 1.150-1.756, p = 0.001) and disadvantages (OR 1.554, 95% CI 1.240-1.947, p < 0.001) than White men, this did not correlate with higher rates of PSA screening (OR 1.086; 95% CI 0.865-1.364, p = 0.477):](/images/com-doc-importer/263-aua-2026/aua-2026-prostate-cancer-screening-detection-and-surveillance-guidelines-versus-real-world-practice-versus-recent-evidence/image-10.jpg)
There is mounting evidence that shared decision-making is an uncommon occurrence in PSA screening.
Dr. Mian concluded his presentation discussing guidelines, real-world practice, and recent evidence for prostate cancer screening, detection, and surveillance with the following open-ended questions:
- Are we creating a standard, shared decision-making that no one can meet?
- Can highly nuanced screening guidelines be effective?
- What may be a simpler, less nuanced message for primary care physicians?
Presented by: Badar Mian, MD, Albany Medical Center, Albany, NY
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
References:
- Young GJ, Harrison S, Turner EL, et al. Prostate-specific antigen (PSA) testing of men in the UK general practice: a 10-year longitudinal cohort study. BMJ Open 2017 Oct 30;7(10):e017729.
- Han PKJ, Kobrin S, Breen N, et al. National evidence on the use of shared decision making in prostate cancer-specific antigen screening. Ann Fam Med. 2013 Jul-Aug;11(4):306-314.
- Basin MF, Crane K, Basnet A, et al. Disparities associated with shared decision-making in prostate cancer. Eur Urol Focus. 2023 Nov;9(6):1008-1015.