(UroToday.com) The 2026 American Urologic Association (AUA) Annual Meeting featured an innovative presentation by Dr. Soichiro Yoshida evaluating the time-dependent overall survival benefit of enzalutamide plus radium-223 in men with metastatic castration-resistant prostate cancer (mCRPC) using reconstructed individual patient data (rIPD) from the EORTC 1333/PEACE-3 trial.
While the recently published PEACE-3 analysis demonstrated a significant overall survival advantage with this combination,1 early crossing of the Kaplan-Meier curves raised important questions regarding whether the treatment effect varied over time and whether standard proportional hazards modeling underestimated the true magnitude and timing of benefit.
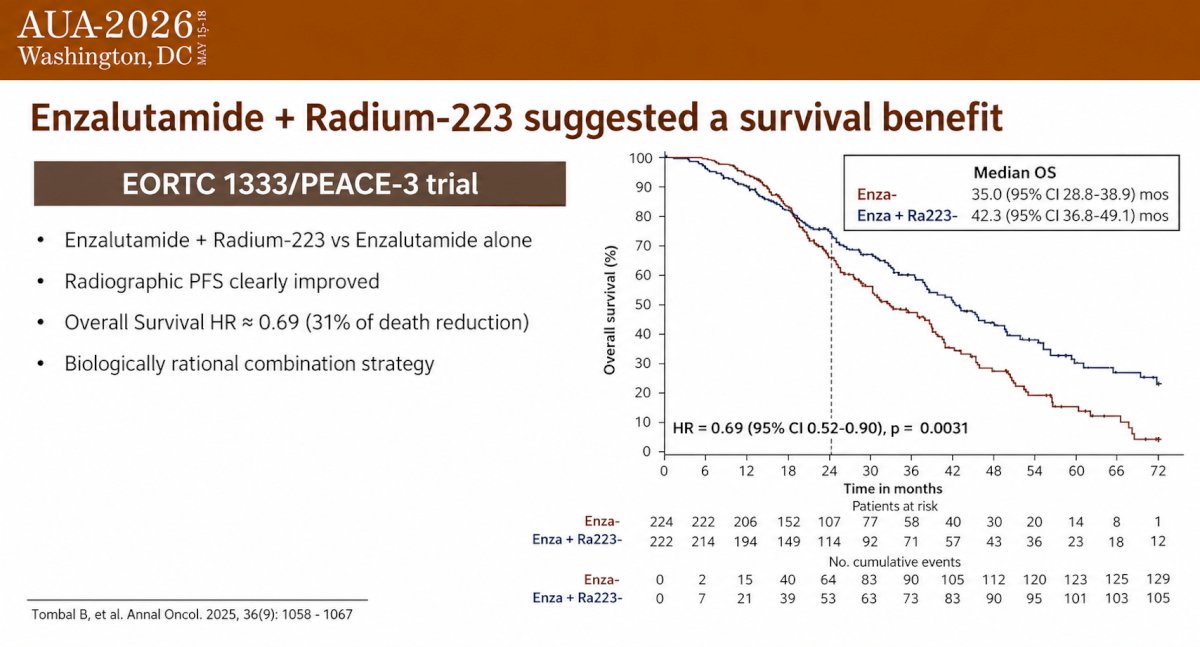
The EORTC 1333/PEACE-3 trial randomized patients with bone-metastatic mCRPC to receive enzalutamide plus radium-223 versus enzalutamide alone. The study demonstrated significant improvements in radiographic progression-free survival and overall survival, with a hazard ratio for death of 0.69 (95% CI 0.52–0.90; p = 0.0031), corresponding to a 31% reduction in the risk of death. Median overall survival improved from 35.0 months (95% CI 28.8–38.9) with enzalutamide alone to 42.3 months (95% CI 36.8–49.1) with the addition of radium-223.
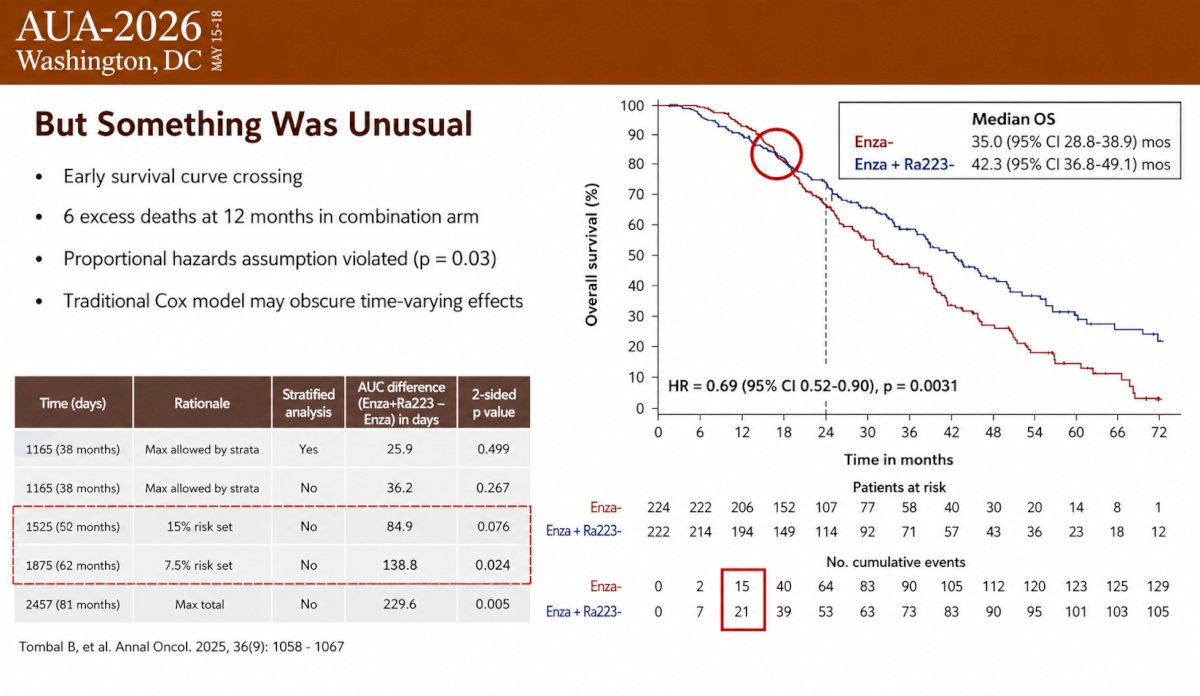
Despite these favorable results, the investigators noted several unusual features of the survival curves:
- Early crossing of the Kaplan-Meier curves
- Six excess deaths in the combination arm at 12 months
- Violation of the proportional hazards assumption (p = 0.03)
- Concern that conventional Cox regression may obscure time-varying treatment effects
These observations led the investigators to ask three key questions:
- Is the treatment benefit time-dependent?
- Is there early harm followed by delayed benefit?
- When does the survival advantage truly emerge?
To address these questions, the investigators reconstructed individual patient data from the published overall survival curves and performed a comprehensive non-proportional hazards (NPH) analysis. Quantitative validation confirmed excellent agreement between the reconstructed and original trial data, with a consistency test demonstrating z = 0.04 and p = 0.97.
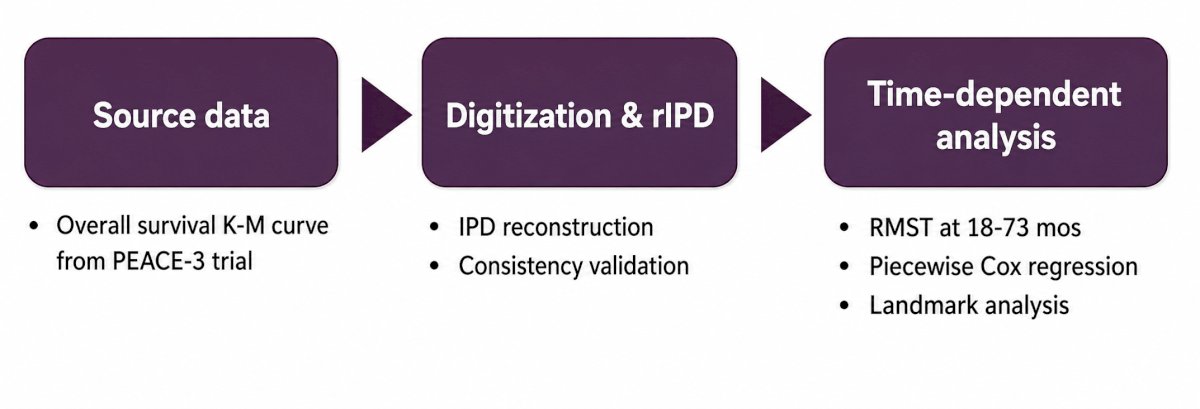
The analytical approach consisted of three sequential steps:
- Extraction of source data from the original PEACE-3 Kaplan-Meier curves
- Digitization and reconstruction of individual patient data with consistency validation
- Time-dependent analyses using:
- Restricted mean survival time (RMST)
- Piecewise Cox regression
- Landmark analyses
Formal testing confirmed a significant violation of the proportional hazards assumption (χ² = 5.01, p = 0.03).
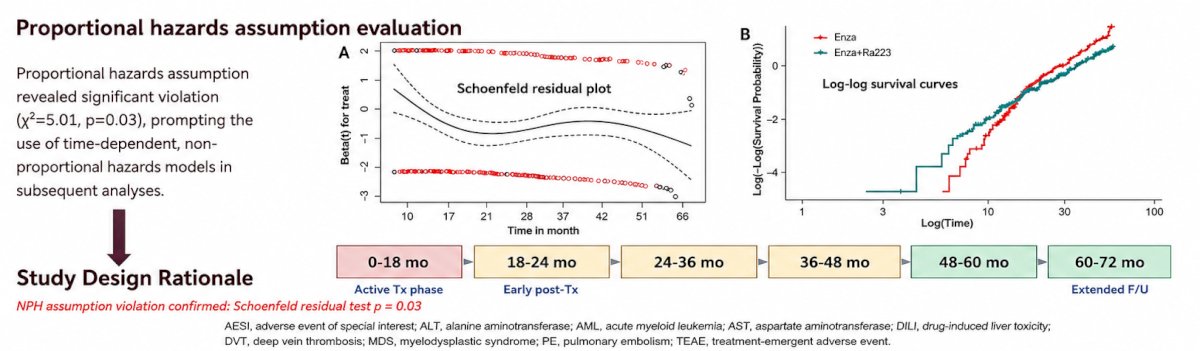
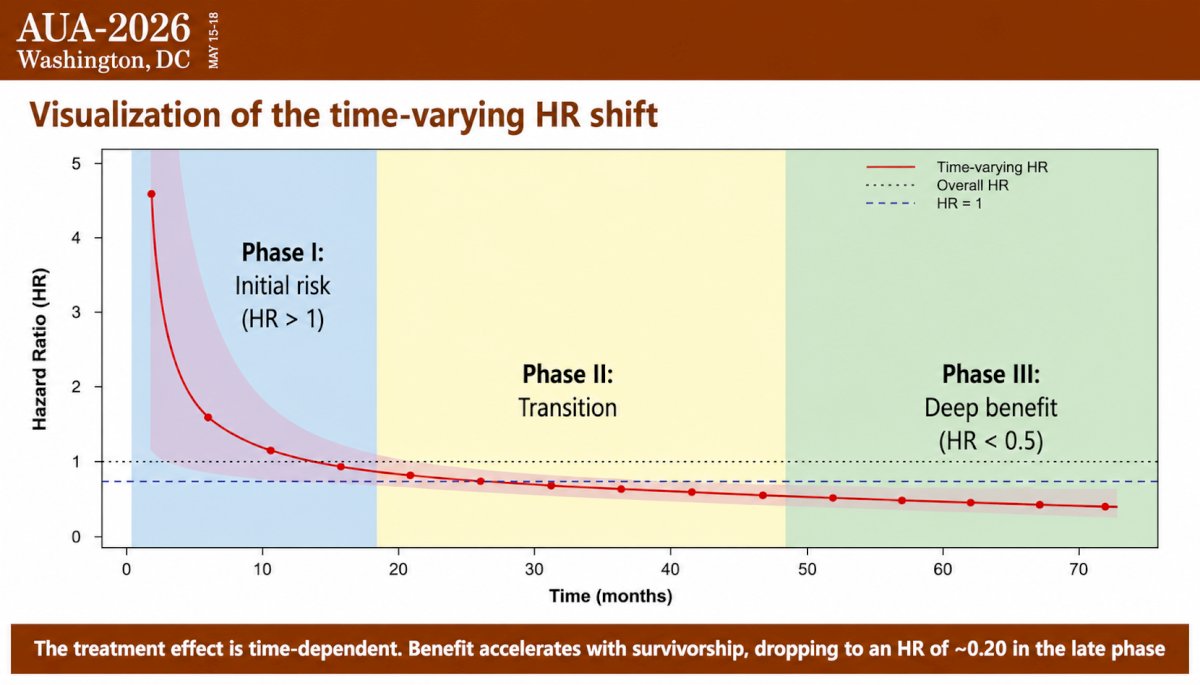
Based on these findings, the investigators divided the treatment effect into three clinically meaningful phases:
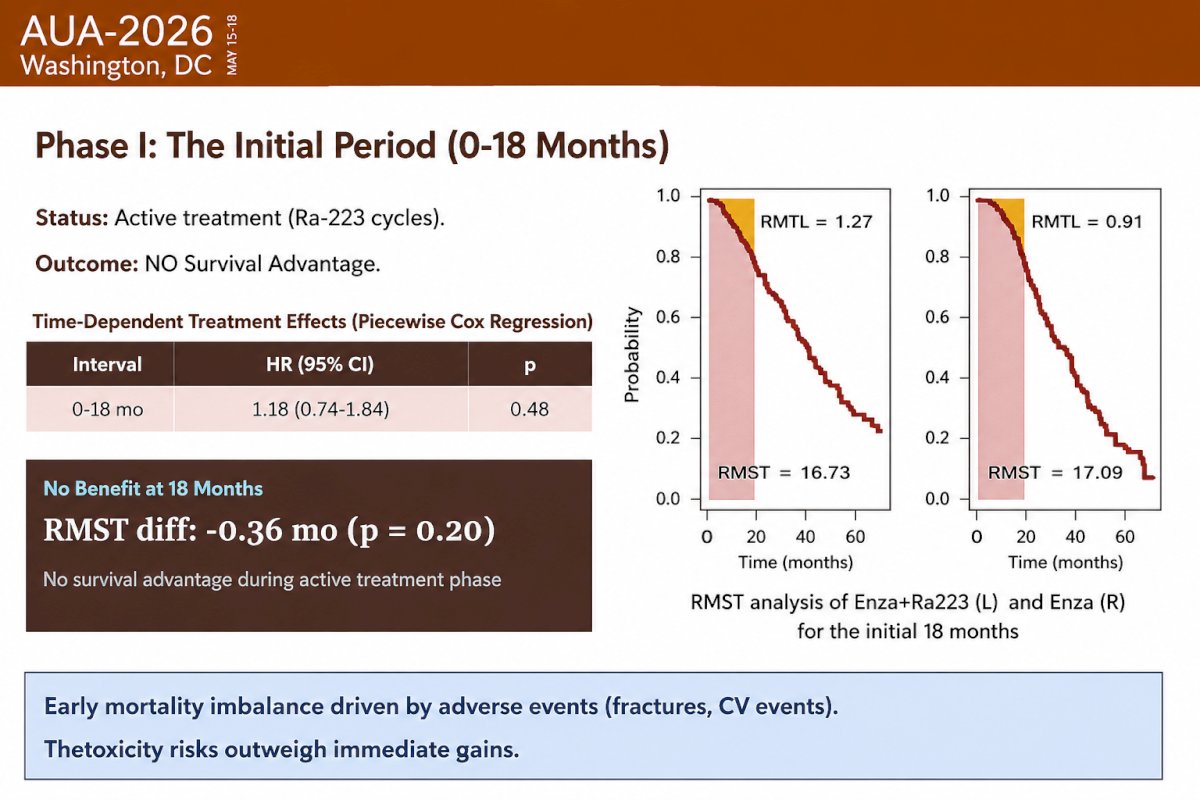
- Phase I: Initial period (0–18 months)
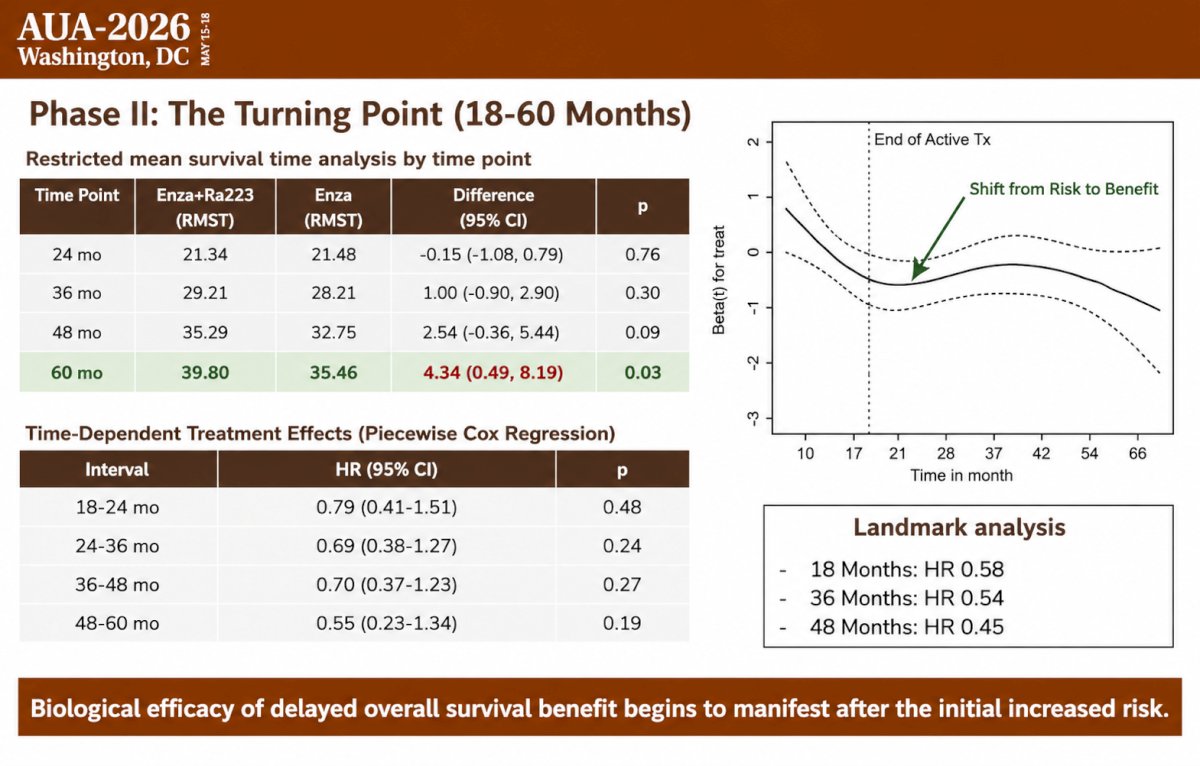
- Phase II: Turning point (18–60 months)
- Phase III: Long-term benefit (60+ months)
Phase I represented the active treatment period during which patients received radium-223. During this interval, there was no evidence of an overall survival advantage:
- Piecewise Cox HR: 1.18 (95% CI 0.74–1.84; p = 0.48)
- RMST difference at 18 months: −0.36 months (p = 0.20)
The investigators hypothesized that early mortality imbalance may have been driven by treatment-related adverse events, particularly fractures and cardiovascular events, and concluded that toxicity risks outweighed any immediate gains during the active treatment period.
Phase II represented the transition period during which the biological effects of radium-223 began to emerge. RMST analyses demonstrated progressively widening separation over time:
- 24 months: −0.15 months (p = 0.76)
- 36 months: +1.00 month (p = 0.30)
- 48 months: +2.54 months (p = 0.09)
- 60 months: +4.34 months (95% CI 0.49–8.19; p = 0.03)
Piecewise Cox modeling showed numerically favorable but individually nonsignificant hazard ratios during this period:
- 18–24 months: HR 0.79
- 24–36 months: HR 0.69
- 36–48 months: HR 0.70
- 48–60 months: HR 0.55
Landmark analyses also demonstrated increasingly favorable hazard ratios when conditioning on longer survival:
- From 18 months: HR 0.58
- From 36 months: HR 0.54
- From 48 months: HR 0.45
These findings indicate that the biological efficacy of radium-223 begins to manifest after the initial treatment-related risk period.
Phase III captured the late survival benefit among long-term survivors. At 72 months, the treatment effect became both clinically and statistically significant:
- RMST at 72 months:
- Enzalutamide + radium-223: 43.23 months
- Enzalutamide alone: 36.98 months
- RMST difference: +6.25 months (95% CI 1.56–10.95; p = 0.01)
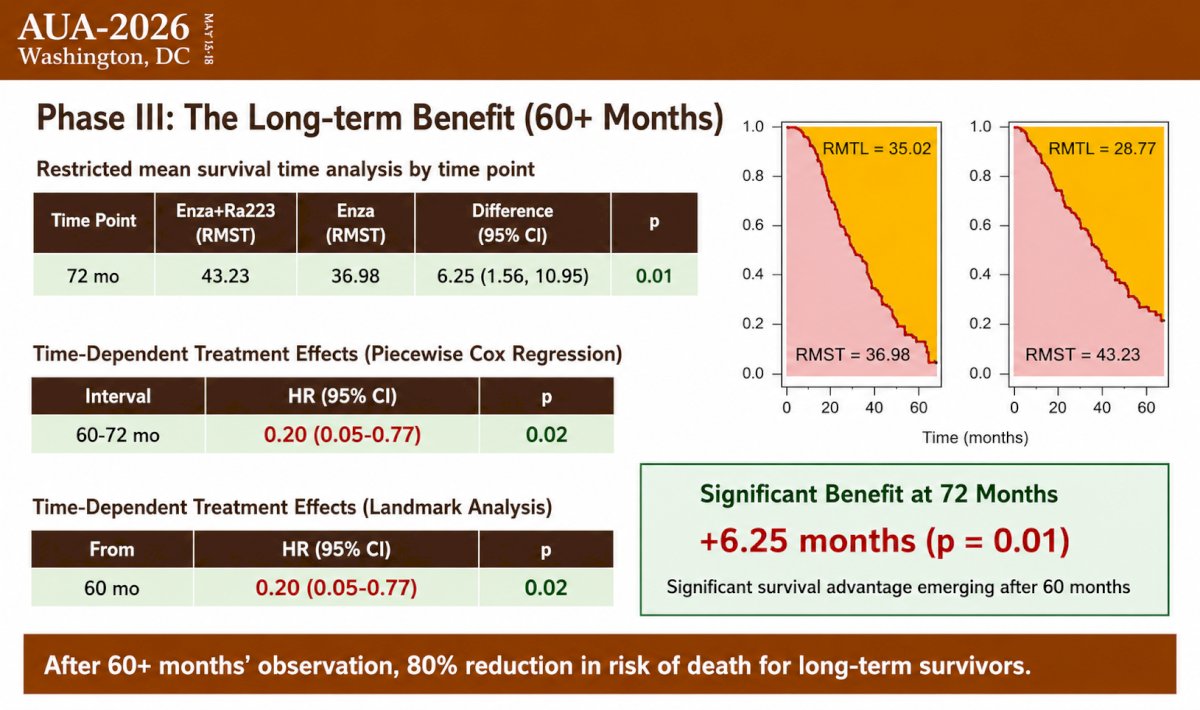
During the 60–72 month interval, the magnitude of benefit was particularly striking:
- Piecewise Cox HR: 0.20 (95% CI 0.05–0.77; p = 0.02)
- Landmark analysis from 60 months: HR 0.20 (95% CI 0.05–0.77; p = 0.02)
These results correspond to an 80% reduction in the risk of death among patients surviving beyond five years.
The investigators also provided several biological explanations for this delayed treatment effect. Radium-223 is not a rapidly cytoreductive therapy; rather, it delivers targeted alpha radiation to bone metastases through calcium-mimetic properties. Its biological impact likely accumulates over time and may only become clinically apparent months after completion of the six-month treatment course. Additionally, dual targeting with enzalutamide and radium-223 may disrupt multiple resistance pathways over time. Mandatory use of bone-protecting agents, instituted during the PEACE-3 trial, substantially reduced fracture risk and may also have contributed to improved long-term outcomes.
Dr. Chen concluded that enzalutamide plus radium-223 demonstrates a delayed but substantial overall survival benefit in men with bone-metastatic mCRPC. No survival advantage is evident during the first 18 months, but the benefit emerges gradually and becomes statistically significant after 60 months, resulting in more than six months of additional survival at 72 months and an 80% reduction in the risk of death among long-term survivors. These findings underscore the importance of non-proportional hazards analyses for therapies with time-varying effects and suggest that conventional Cox modeling may underestimate the long-term impact of treatments such as radium-223.
From a clinical standpoint, these results indicate that patients require sufficient life expectancy to realize the full benefits of this treatment strategy. Both clinicians and patients should adopt a long-term perspective, recognizing that meaningful survival gains may take several years to materialize. The findings support consideration of enzalutamide plus radium-223 as a first-line option for appropriately selected patients with bone-metastatic mCRPC and favorable prognostic features. Final overall survival analyses from PEACE-3 are anticipated and may reveal an even greater long-term survival advantage.
Presented by: Soichiro Yoshida, MD, PhD, Tokyo Medical and Dental University, Tokyo, Japan
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
Reference: