(UroToday.com) The 2026 American Urologic Association Annual Meeting featured a presentation by Dr. Alan H. Bryce evaluating the safety and tolerability of rucaparib compared with physician’s choice of docetaxel or a second-generation androgen receptor pathway inhibitor (ARPI) in patients with BRCA-mutated metastatic castration-resistant prostate cancer (mCRPC) enrolled in the phase III TRITON3 trial.
TRITON3 previously demonstrated that rucaparib significantly improved radiographic progression-free survival (rPFS) compared with physician’s choice therapy in chemotherapy-naïve patients with mCRPC harboring BRCA alterations, reducing the risk of progression or death by 50%.1 In this presentation, Dr. Bryce focused on the detailed safety profile of rucaparib, including the incidence, timing, and management of the most common treatment-emergent adverse events (TEAEs), as well as adverse events of special interest such as anemia, thromboembolic events, and myelodysplastic syndrome/acute myeloid leukemia (MDS/AML).
TRITON3 was a global, randomized, open-label phase III trial that enrolled patients with:
- Chemotherapy-naïve mCRPC
- A deleterious BRCA1, BRCA2, or ATM alteration identified by tissue or plasma testing
- Prior treatment with one second-generation ARPI in any disease setting
- ECOG performance status 0–1
Patients were randomized in a 2:1 ratio to:
- Rucaparib 600 mg twice daily (n = 270)
- Physician’s choice (n = 135), consisting of:
- Docetaxel (n = 75), or
- Abiraterone acetate or enzalutamide (n = 60)
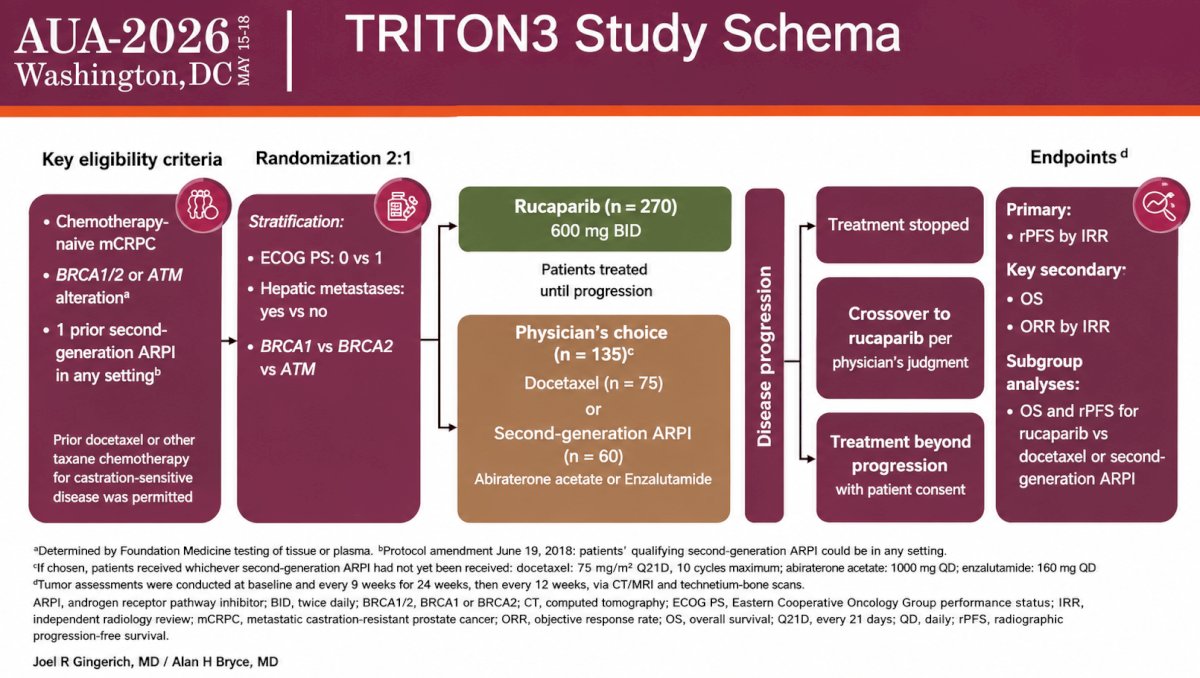
Randomization was stratified by ECOG performance status, presence of hepatic metastases, and genomic alteration subtype (BRCA1 vs BRCA2 vs ATM). The primary endpoint was independent radiology review (IRR)-assessed rPFS, with overall survival (OS) and objective response rate (ORR) as key secondary endpoints.
The current safety analysis focused specifically on the BRCA-mutated population, which included:
- Rucaparib: 201 patients
- Physician’s choice: 97 patients
- Docetaxel: 57 patients
- Second-generation ARPI: 40 patients
At the August 25, 2022, data cutoff, all patients experienced at least one TEAE.
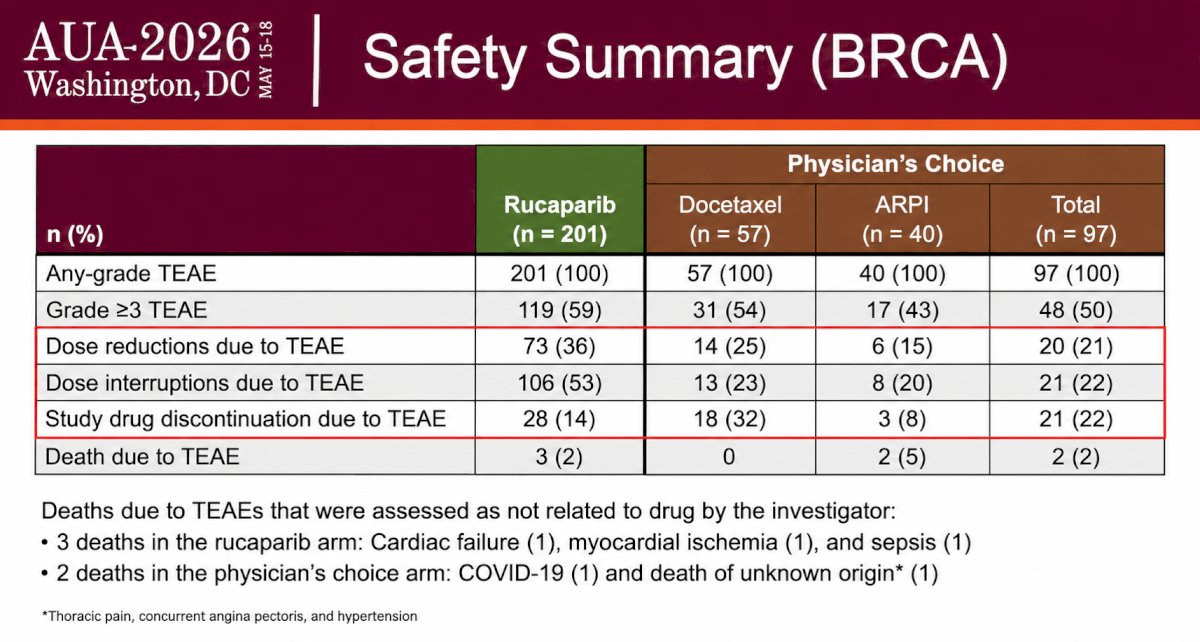
Grade ≥3 TEAEs were reported in:
- 59% of rucaparib-treated patients
- 50% of patients receiving the physician’s choice
- 54% with docetaxel
- 43% with ARPI therapy
Dose modifications were common with rucaparib but rarely led to permanent discontinuation:
- Dose reductions due to TEAEs: 36% with rucaparib vs 21% with physician’s choice
- Dose interruptions: 53% vs 22%
- Treatment discontinuation due to TEAEs: 14% vs 22%
Deaths attributed to TEAEs occurred in 3 rucaparib-treated patients (2%) and 2 patients receiving physician’s choice (2%). All were considered unrelated to the study treatment by the investigators.
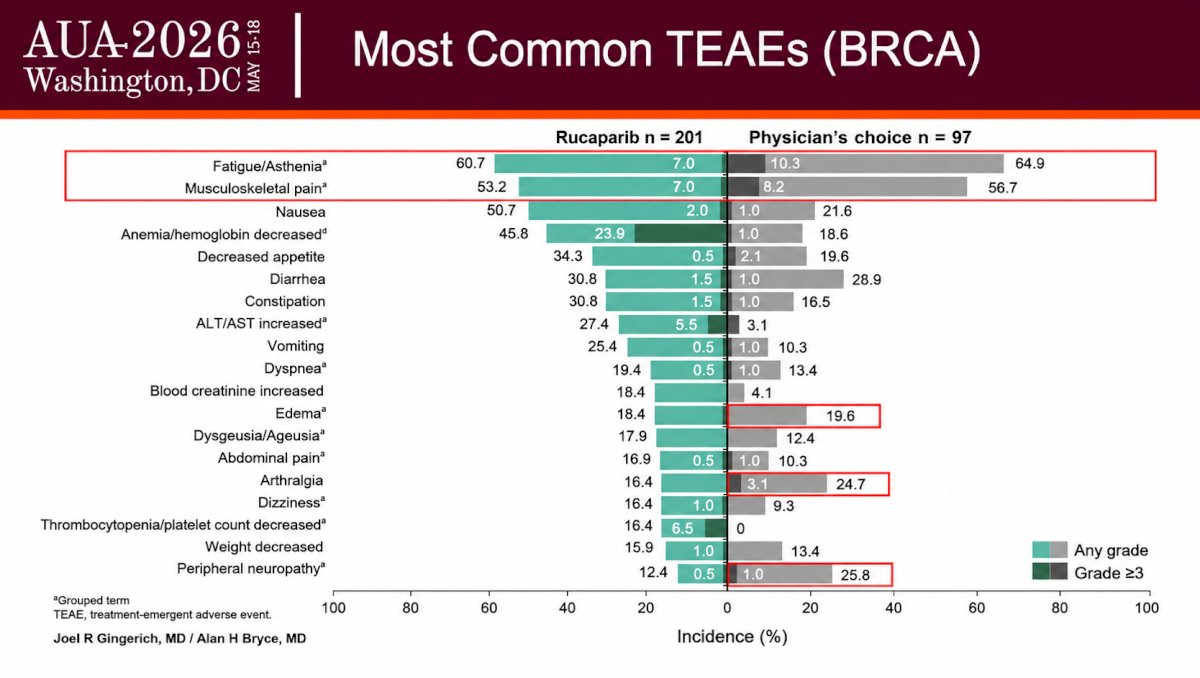
The most common any-grade TEAEs with rucaparib included:
- Fatigue/asthenia: 60.7% (Grade ≥3: 7.0%)
- Musculoskeletal pain: 53.2% (Grade ≥3: 7.0%)
- Nausea: 50.7% (Grade ≥3: 2.0%)
- Anemia/hemoglobin decreased: 45.8% (Grade ≥3: 23.9%)
Compared with the physician’s choice, rucaparib was associated with lower rates of several toxicities commonly observed with chemotherapy:
- Peripheral neuropathy: 12.4% vs 25.8%
- Arthralgia: 16.4% vs 24.7%
- Edema: 18.4% vs 19.6%
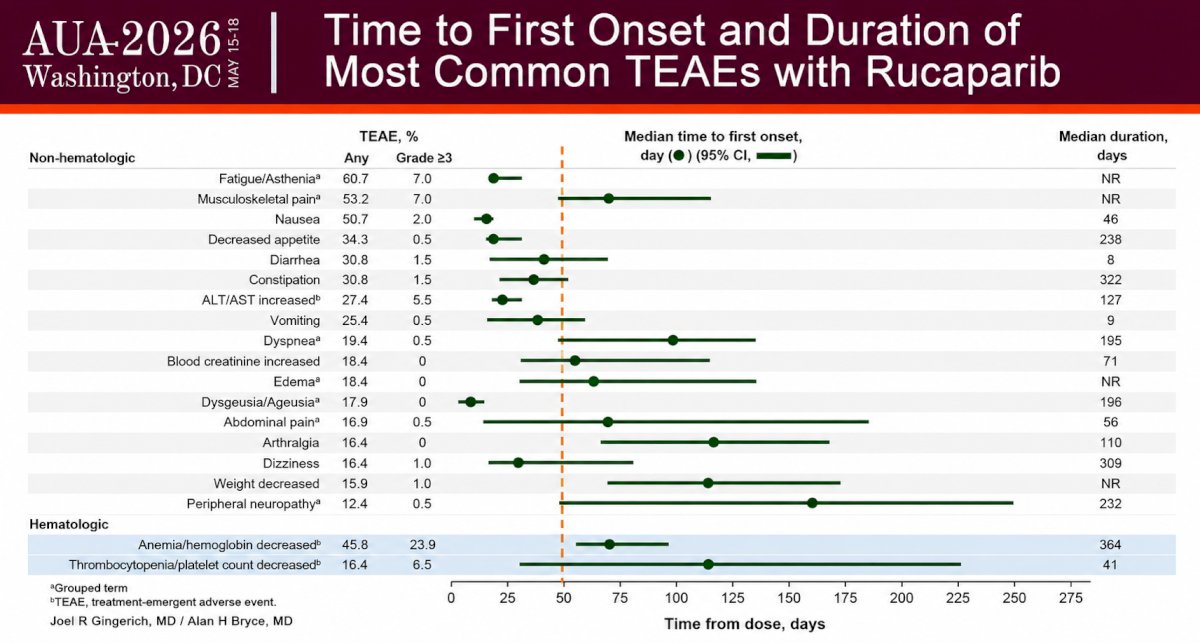
The temporal profile of adverse events demonstrated that many nonhematologic toxicities developed early and were manageable with supportive care and dose adjustments.
Median time to first onset with rucaparib included:
- Fatigue/asthenia: ~57 days
- Nausea: ~27 days
- ALT/AST elevation: ~21 days
- Anemia/hemoglobin decreased: ~67 days
- Thrombocytopenia: ~112 days
Median duration of select events included:
- Anemia: 364 days
- Thrombocytopenia: 41 days
- Nausea: 46 days
- Fatigue/asthenia: not reached
The recommended rucaparib dose modifications for TEAEs were:
- Starting dose: 600 mg twice daily
- First reduction: 500 mg twice daily
- Second reduction: 400 mg twice daily
- Third reduction: 300 mg twice daily
Despite dose modifications, treatment intensity remained high. The median dose intensity was 98% (range: 36–100%), and among patients who remained on treatment, more than 75% continued receiving 500 mg or 600 mg twice daily for over one year.
Adverse events of special interest with rucaparib included:
- Anemia requiring transfusion: 28%
- Pulmonary embolism: 4.5% any grade; 3.0% Grade ≥3
- Deep vein thrombosis: 1.5% any grade; 0.5% Grade ≥3
- MDS/AML: 2 patients (1%)
- Pneumonitis: 1 patient (0.5%)
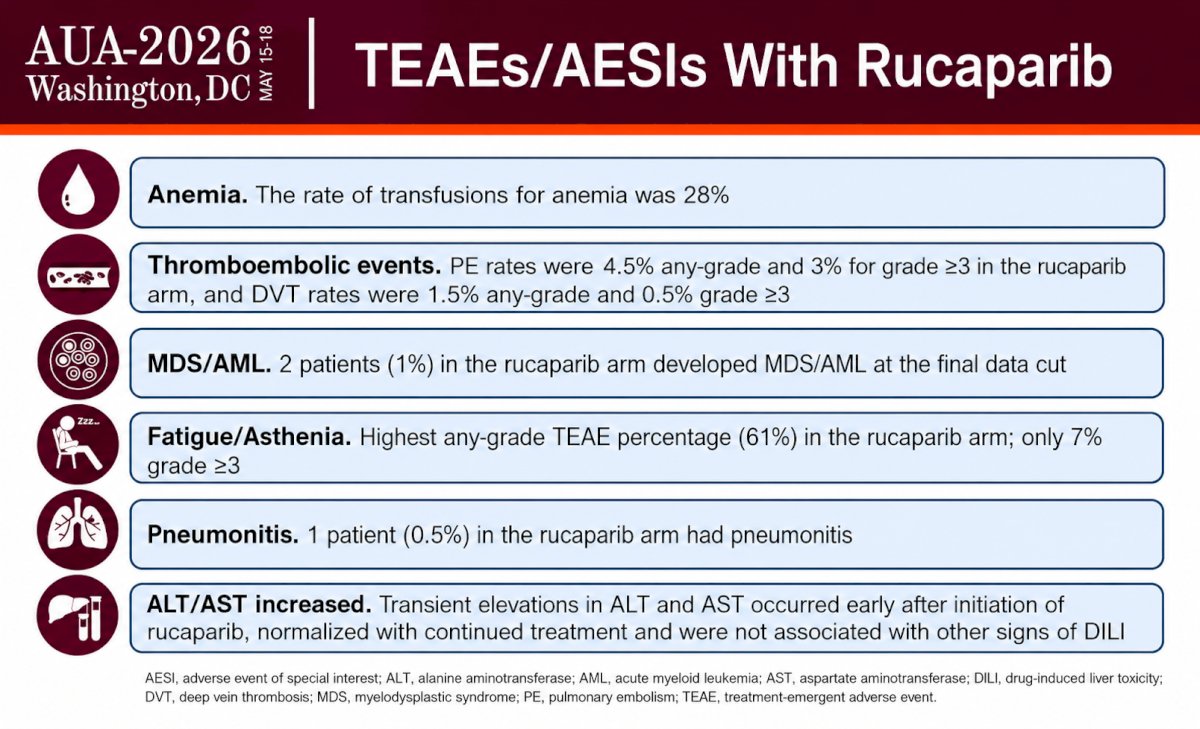
Transient elevations in ALT and AST occurred early after treatment initiation, normalized with continued therapy, and were not associated with other signs of drug-induced liver injury.
Dr. Bryce concluded his presentation of the TRITON3 safety analysis in BRCA patients as follows:
- Rucaparib has a well-defined and manageable safety profile in patients with BRCA-mutated prostate cancer in TRITON3.
- There was a low rate of discontinuation due to TEAEs, suggesting that supportive care and dose adjustments are effective strategies for mitigating TEAEs.
Presented by: Alan Bryce, MD, Professor of Molecular Medicine at Translational Genomics Research Institute, Chief Clinical Officer, City of Hope, Phoenix, AZ
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
Reference: