(UroToday.com) The 2026 American Urological Association (AUA) Annual Meeting featured a podium presentation by Dr. Neal D. Shore reporting a post hoc exploratory analysis from the phase 3 EMBARK trial evaluating the duration of treatment suspension among all randomized patients with high-risk biochemically recurrent prostate cancer.
EMBARK is a randomized phase III trial of patients with biochemically recurrent prostate cancer and high-risk disease, defined as a prostate-specific antigen doubling time (PSADT) ≤9 months and a PSA level of ≥2 ng/mL above nadir following external beam radiation therapy or ≥1 ng/mL after radical prostatectomy, with or without postoperative radiation therapy.1 Eligible patients had no evidence of metastasis on conventional imaging and baseline eugonadal testosterone levels ≥150 ng/dL. Prior hormone therapy completed at least 9 months before enrollment was permitted.
Patients were randomized 1:1:1 to one of three treatment arms:
- Enzalutamide 160 mg daily plus Leuprolide acetate 22.5 mg intramuscularly every 12 weeks (blinded combination arm; n=355)
- Placebo plus leuprolide acetate (blinded control arm; n=358)
- Enzalutamide monotherapy 160 mg daily (open-label arm; n=355)
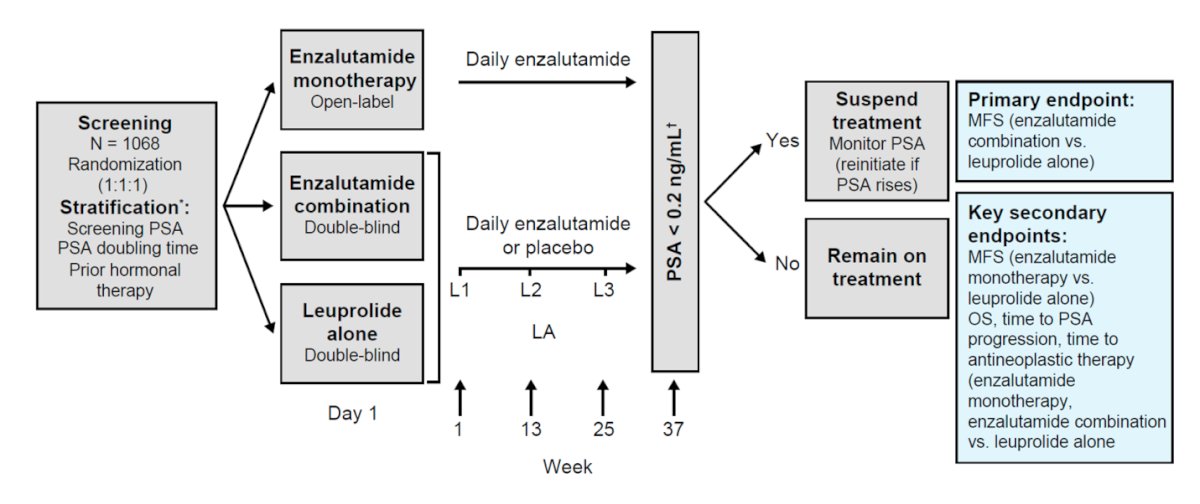
Importantly, EMBARK was not only a study of treatment intensification, but also prospectively incorporated a treatment de-intensification strategy. At week 36, patients with a PSA <0.2 ng/mL became eligible for treatment suspension beginning at week 37, with serial PSA monitoring and treatment re-initiation upon PSA rise. Patients with PSA ≥0.2 ng/mL continued assigned therapy until progression, unacceptable toxicity, or treatment discontinuation for other reasons.
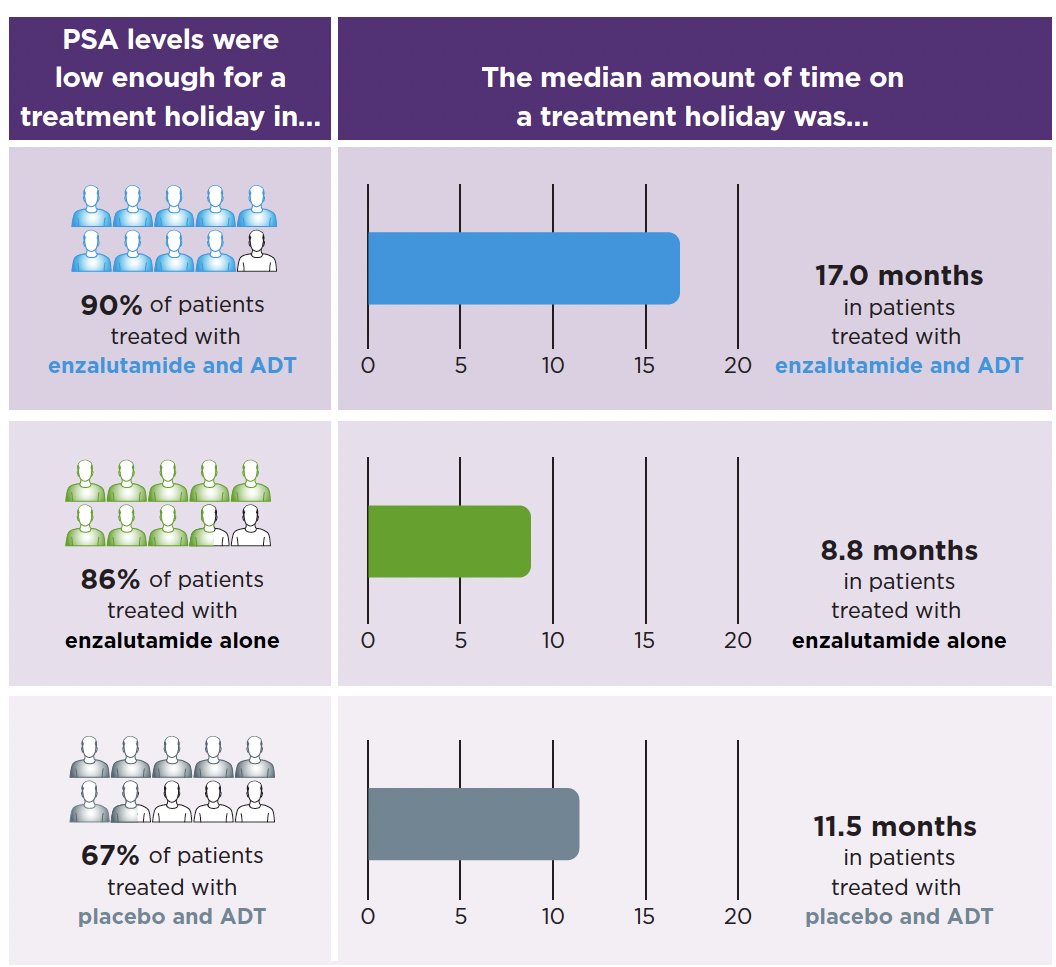
Previously published analyses of treatment suspension duration were limited to patients who actually suspended therapy and therefore did not account for the substantially lower suspension rates observed in the control arm. Specifically, treatment was suspended in 90% of patients receiving enzalutamide plus leuprolide, 86% receiving enzalutamide monotherapy, and only 67% receiving leuprolide alone. To avoid this post-randomization selection bias, the current post hoc analysis included all randomized patients in the intention-to-treat population, assigning a treatment suspension duration of 0 months to patients who never suspended therapy.
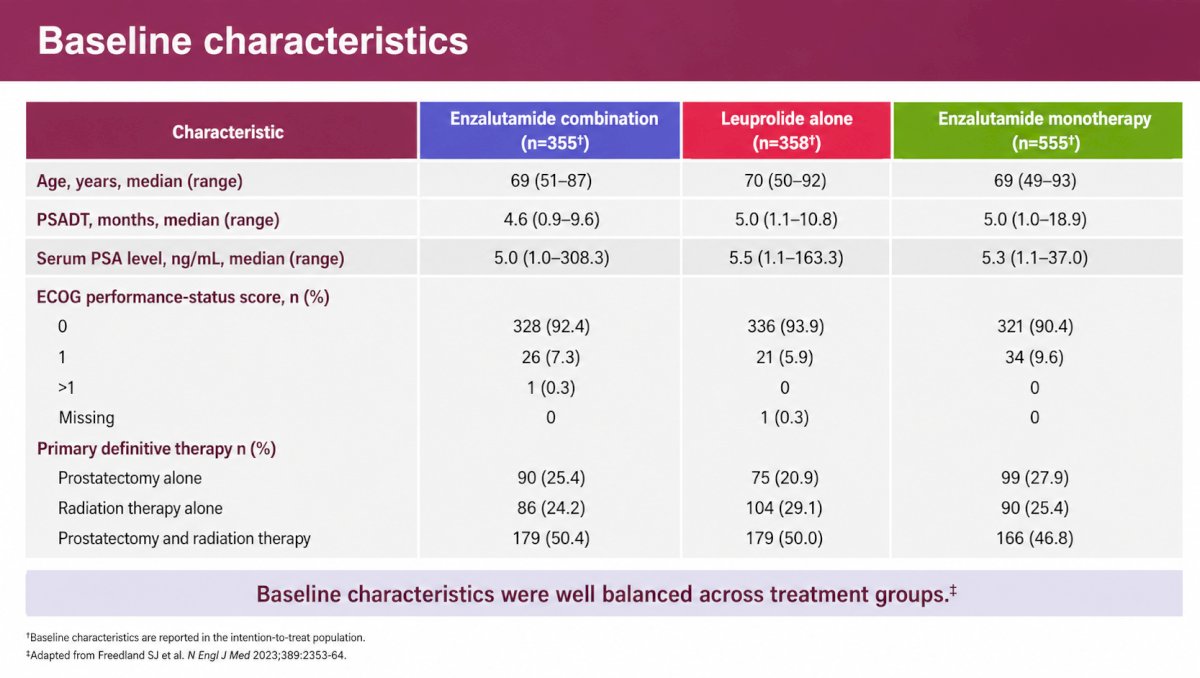
Baseline characteristics were well balanced across the three treatment groups. The median age ranged from 69 to 70 years. The median PSADT ranged from 4.6 to 5.0 months, and the median baseline PSA ranged from 5.0 to 5.5 ng/mL. ECOG performance status was 0 in 90.4–93.9% of patients and 1 in 5.9–9.6%. Approximately half of patients in each arm had undergone both radical prostatectomy and radiation therapy (46.8–50.4%), while 20.9–27.9% had prostatectomy alone and 24.2–29.1% had radiation therapy alone.
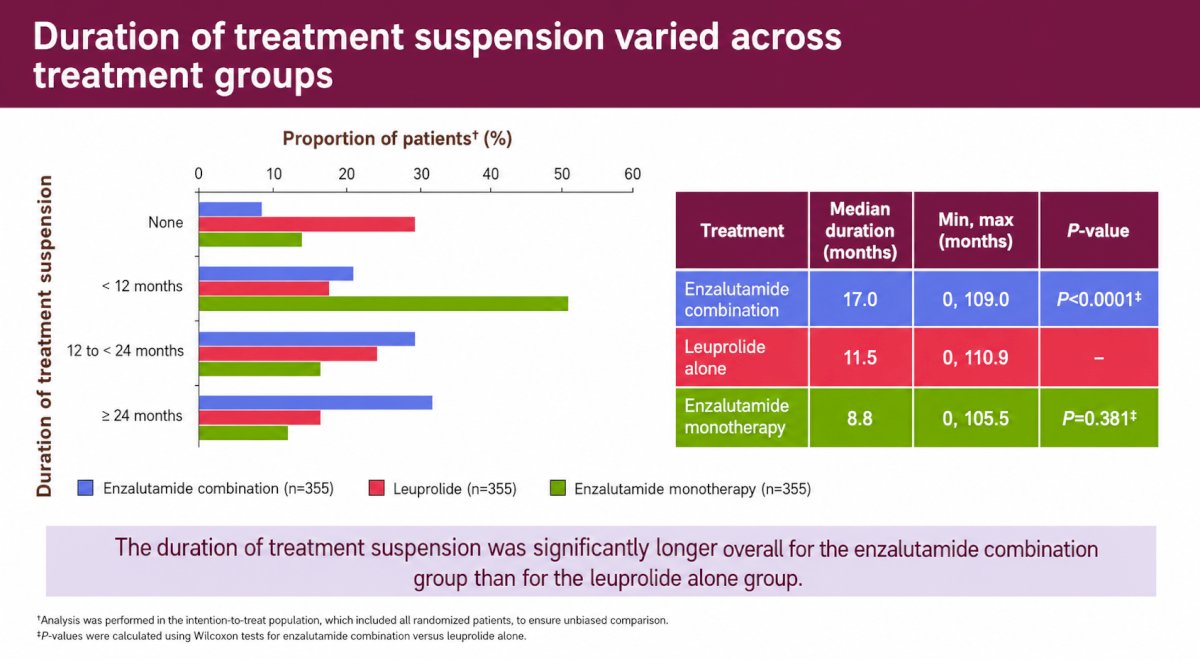
The principal efficacy figure demonstrated significant differences in treatment suspension duration across treatment groups. Median duration of treatment suspension was:
- 17.0 months for enzalutamide plus leuprolide
- 11.5 months for leuprolide alone
- 8.8 months for enzalutamide monotherapy
Compared with leuprolide alone, the combination of enzalutamide plus leuprolide prolonged the median treatment-free interval by 5.5 months, a statistically significant improvement (P<0.0001). In contrast, enzalutamide monotherapy did not significantly differ from leuprolide alone (P=0.3811). The maximum treatment suspension durations exceeded 100 months in all three arms, reaching 109.0 months with combination therapy, 110.9 months with leuprolide alone, and 105.5 months with enzalutamide monotherapy.
The bar graph provided additional insight into the distribution of treatment holidays. Patients treated with enzalutamide plus leuprolide were most likely to achieve prolonged treatment suspension lasting ≥24 months. In contrast, patients receiving enzalutamide monotherapy most commonly experienced shorter treatment holidays of <12 months, whereas those treated with leuprolide alone were most likely to have no treatment suspension at all.
Dr. Shore emphasized that these findings should be interpreted in the context of the primary EMBARK results, which demonstrated that enzalutamide plus leuprolide significantly improved metastasis-free survival and overall survival compared with leuprolide alone. Thus, despite nearly six additional months off therapy, the combination arm maintained superior long-term oncologic outcomes.
Dr. Neal Shore concluded his presentation of the post-hoc EMBARK analyses as follows:
- Despite nearly 6 months longer treatment suspension, the enzalutamide combination demonstrated superior OS compared with leuprolide alone.
- The duration of treatment suspension was not significantly different between enzalutamide monotherapy and leuprolide alone.
- Treatment suspension was most likely to last for ≥2 years in the enzalutamide combination group, and <1 year in the enzalutamide monotherapy group; patients who received leuprolide alone were most likely to have no treatment suspension.
- These findings support the potential for a treatment holiday with enzalutamide combination to maintain efficacy, while reducing the treatment burden in patients with high-risk biochemically recurrent prostate cancer.
Presented by: Neal D. Shore, MD, FACS, Director, CPI (Certified Principal Investigator by the Association of Clinical Research Professionals), START Carolinas/Carolina Urologic Research Center, Head of GU Oncology and Radiopharm, START Center for Cancer Research Institute, AUC Urology Specialists, Myrtle Beach, SC
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
Reference: