(UroToday.com) The 2026 American Urological Association (AUA) Annual Meeting featured a poster presentation by Dr. Murilo de Almeida Luz and colleagues reporting post hoc analyses from the international DAROL study evaluating the safety, effectiveness, and health-related quality of life (HRQoL) of darolutamide in patients with nonmetastatic castration-resistant prostate cancer (nmCRPC) stratified by comorbidity burden.
Darolutamide is a standard-of-care treatment for men with nmCRPC, supported by the phase III ARAMIS trial.1 However, patients with nmCRPC are frequently elderly and often have substantial comorbidity burdens and polypharmacy, raising important questions regarding the tolerability and effectiveness of darolutamide in routine clinical practice.
The DAROL study (NCT04122976) is an ongoing international, prospective, observational study designed to assess the real-world safety and effectiveness of darolutamide and to complement the ARAMIS trial experience. In this interim analysis, patients were stratified using the Charlson Comorbidity Index (CCI), with scores ≤5 categorized as low to moderate comorbidities and scores >5 categorized as high comorbidities.
The safety analysis set included 799 patients, of whom 269 (34%) had low to moderate comorbidities and 530 (66%) had high comorbidity burdens. Most patients had at least one ongoing comorbidity at study entry, most commonly vascular and metabolic disorders, and the majority were receiving concomitant medications.
As shown in the baseline characteristics table, patients with high comorbidity burdens were substantially older, with a median age of 82 years compared with 72 years in the low to moderate comorbidity group. They also had worse performance status, with ECOG 0 in 50% versus 69.1%, and a greater proportion with ECOG 2–3 (7.2% versus 2.2%). Despite these differences, key disease characteristics were generally balanced, including Gleason score, baseline PSA, and PSA doubling time. Median PSA doubling time was 4.6 months in the low to moderate group and 5.8 months in the high comorbidity group.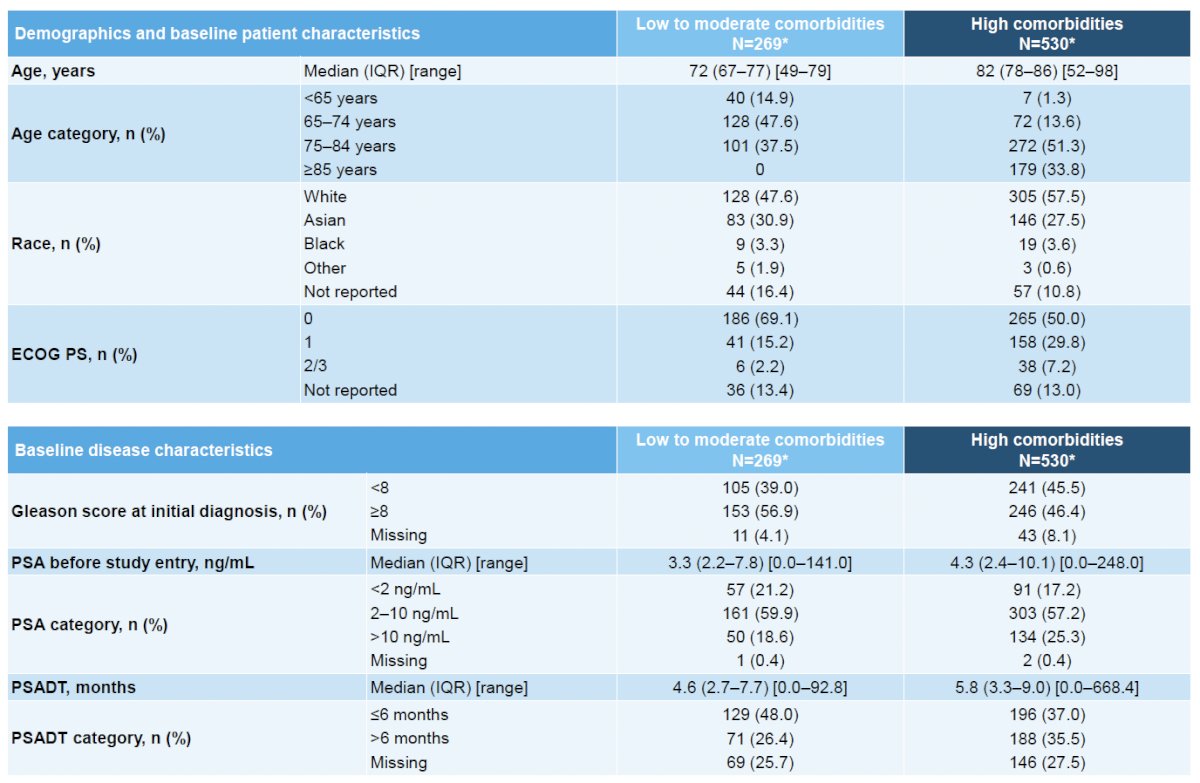
The concomitant medication table highlighted the extent of polypharmacy in this population. Any concomitant medication was reported in 69.9% of patients with low to moderate comorbidities and 82.6% of those with high comorbidities. Common medication classes included cardiovascular agents (52.4% and 68.3%, respectively), alimentary tract and metabolism drugs (47.6% and 65.5%), nervous system agents (31.6% and 54%), and blood and blood-forming agents (27.1% and 48.7%).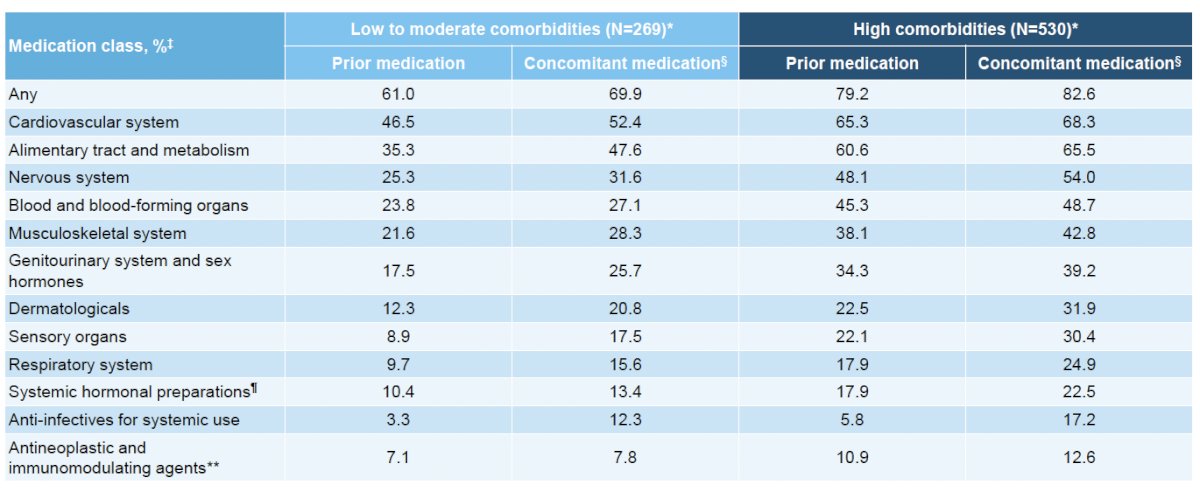
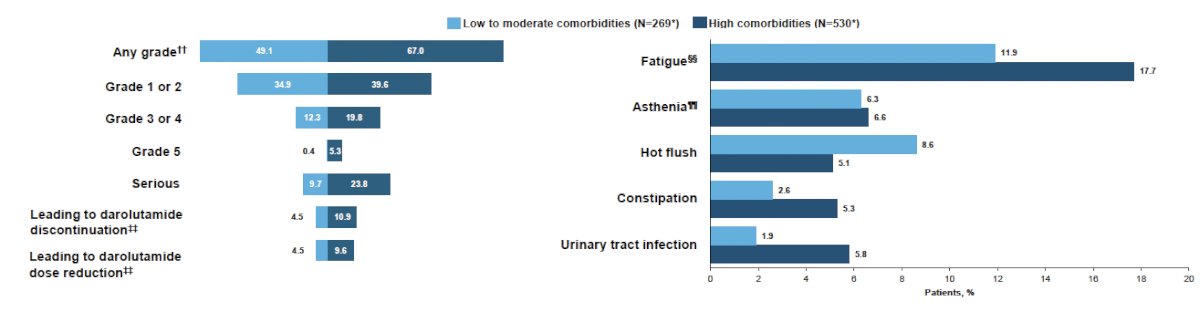
The safety overview demonstrated that treatment-emergent adverse events (TEAEs) were more frequent among patients with higher comorbidity burdens, although most were low-grade. Any-grade TEAEs occurred in 67% of patients with high comorbidities compared with 39.6% in those with low to moderate comorbidities. Serious TEAEs were reported in 23.8% versus 10.9%, and discontinuations due to TEAEs occurred in 12.3% versus 9.7%, respectively. Fatigue was the most commonly reported individual TEAE, occurring in 17.7% of patients with high comorbidities compared with 5.8% in the low to moderate comorbidity subgroup.
Importantly, effectiveness outcomes were generally similar between the two groups. The proportion of patients achieving a ≥50% PSA decline at any time was 81.6% in the low to moderate comorbidity subgroup and 79.4% in the high comorbidity subgroup. Corresponding PSA90 response rates were 59% and 56.6%, respectively.
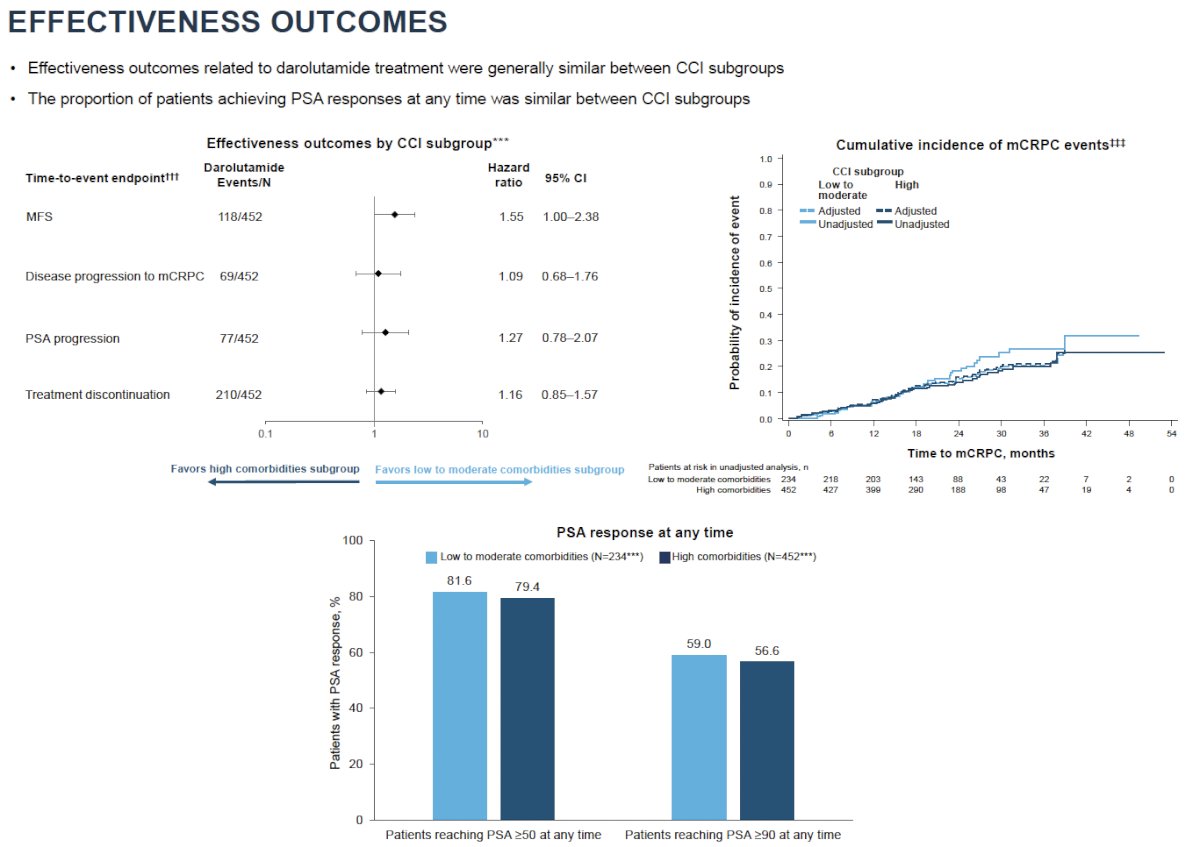
The forest plot of inverse probability of treatment weighted (IPTW) analyses demonstrated no meaningful differences in most time-to-event outcomes. Hazard ratios comparing high versus low to moderate comorbidity groups were 1.09 (95% CI 0.68–1.76) for progression to metastatic CRPC, 1.27 (95% CI 0.78–2.07) for PSA progression, and 1.16 (95% CI 0.85–1.57) for treatment discontinuation. Metastasis-free survival numerically favored patients with lower comorbidity burdens (HR 1.55, 95% CI 1.00–2.38), although the overall pattern suggested broadly comparable effectiveness across groups.
The cumulative incidence curves for progression to metastatic CRPC overlapped closely between subgroups, further supporting similar disease control regardless of comorbidity status.
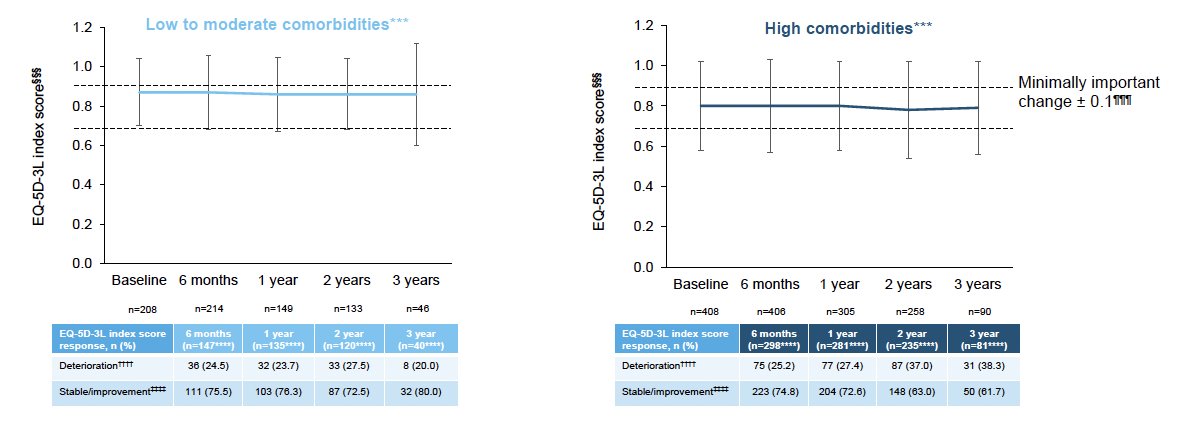
HRQoL was assessed using the EQ-5D-3L index score. Baseline scores were generally favorable, approximately 0.8 in both groups, indicating minimal limitations in mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. As shown in the longitudinal HRQoL plots, scores remained stable over three years of treatment and stayed well within the minimally important change threshold of ±0.1. At 6 months, stable or improved EQ-5D-3L scores were observed in 75.5% of patients with low to moderate comorbidities and 74.8% of those with high comorbidities. Even at 3 years, 80.0% and 61.7% of patients, respectively, maintained stable or improved HRQoL, though patient numbers were smaller at later time points.
The investigators concluded that darolutamide is effective and well-tolerated in real-world patients with nmCRPC, including those with substantial comorbidity burdens and extensive concomitant medication use. Although patients with higher comorbidity burdens experienced more adverse events, these were predominantly low-grade; a few patients discontinued treatment, and treatment effectiveness and quality of life were generally maintained.
These findings reinforce that, in routine clinical practice, darolutamide can be considered a standard-of-care treatment option for patients with nmCRPC regardless of comorbidity status.
Presented by: Murilo de Almeida Luz, MD, Hospital Erasto Gaertner, Curitiba, Brazil
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
Reference: