(UroToday.com) The 2026 American Urological Association (AUA) Annual Meeting featured a poster presentation by Dr. Neal Shore and colleagues evaluating the impact of anemia and anemia-directed management strategies on patient-reported health-related quality of life (HRQoL) among patients with metastatic castration-resistant prostate cancer (mCRPC) treated with talazoparib plus enzalutamide (TALA+ENZA) in the phase 3 TALAPRO-2 trial.
TALAPRO-2 established talazoparib plus enzalutamide as an effective first-line treatment option for patients with mCRPC, demonstrating clinically meaningful and statistically significant improvements in radiographic progression-free survival compared with enzalutamide alone.1,2 Importantly, overall HRQoL was maintained with the combination, with no clinically meaningful differences compared with placebo plus enzalutamide. However, anemia is among the most common treatment-emergent adverse events associated with talazoparib, frequently necessitating dose modification and/or blood transfusion. The current analysis sought to better understand how anemia and its management influence patient-reported outcomes during therapy.
The study focused on patients in the talazoparib plus enzalutamide arm who experienced ≥1 episode of grade 3 or 4 anemia and had baseline plus ≥1 post-baseline patient-reported outcome (PRO) assessment. Subgroup analyses evaluated patients who underwent talazoparib dose modification and/or received red blood cell transfusions as strategies to manage anemia.
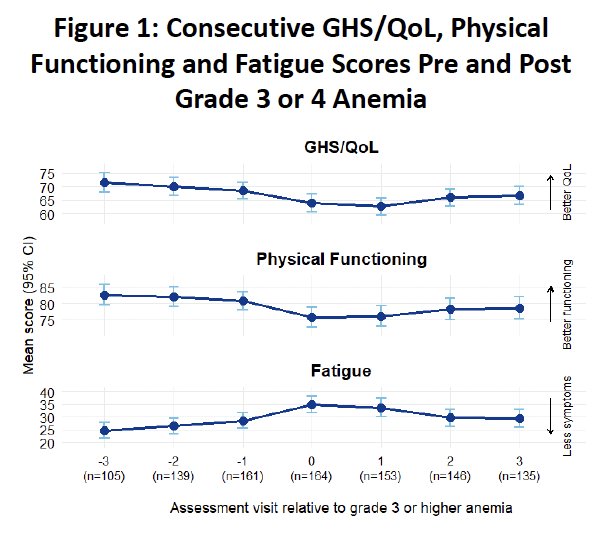
HRQoL was assessed using the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30). Three domains were selected for detailed analysis:
- Global Health Status/Quality of Life (GHS/QoL)
- Physical functioning
- Fatigue
For each clinical event, the investigators examined three consecutive PRO assessments before and three after the event. Time zero was defined as the first PRO assessment following the event, with negative values representing visits before the event and positive values representing subsequent visits.

In the TALAPRO-2 unselected cohort receiving talazoparib plus enzalutamide (n=398), nearly half of patients (49%; 195/398) had baseline grade 1 or 2 anemia. After treatment initiation:
- 68% (270/398) developed anemia of any grade
- 49% (195/398) experienced grade 3 or 4 anemia
Per protocol and investigator discretion, 42% (168/398) received red blood cell transfusions and 45% (177/398) underwent dose modification because of anemia. Among the 398 treated patients, 395 had both baseline and at least one post-baseline PRO assessment.
The first figure evaluated 164 patients who experienced grade 3 or 4 anemia. Across all three domains, HRQoL scores declined progressively in the visits leading up to the onset of severe anemia. Global health status and physical functioning reached their lowest levels immediately after the event, while fatigue worsened in parallel. Following the onset of anemia, all three measures gradually improved over subsequent assessments, suggesting that the adverse impact of severe anemia on HRQoL is at least partially reversible.
The second figure focused on 137 patients receiving their first blood transfusion for anemia. A nearly identical pattern was observed: worsening GHS/QoL and physical functioning and increasing fatigue in the visits preceding transfusion, followed by improvement after transfusion. These data support the clinical utility of transfusion as an effective intervention to mitigate symptomatic consequences of anemia.

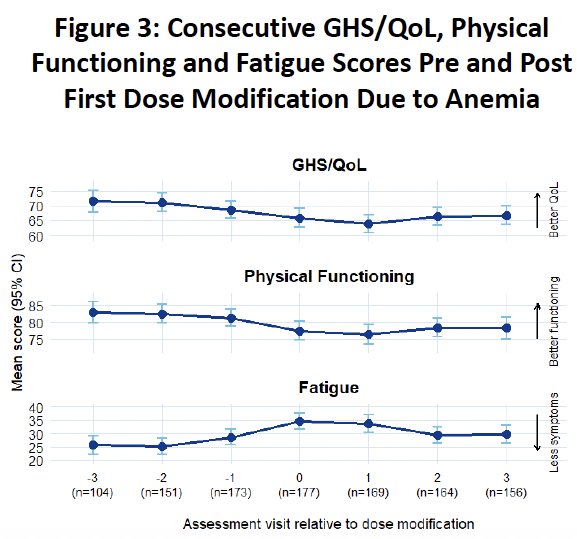
The third figure evaluated 177 patients undergoing their first talazoparib dose modification due to anemia. Again, patient-reported outcomes deteriorated prior to dose adjustment and then gradually improved during subsequent assessments. Together, these parallel trajectories suggest that both transfusion and dose modification are associated with recovery in quality of life and physical functioning after anemia develops.
The investigators concluded that the impact of anemia on HRQoL in patients with mCRPC treated with talazoparib plus enzalutamide can be effectively managed with appropriate blood transfusion and dose modification. They noted that further analyses are needed to address limitations, including baseline anemia status, overlapping treatment-emergent adverse events, simultaneous use of multiple anemia-management strategies, and evaluation of broader PRO domains.
These findings are clinically important because anemia is a common and expected toxicity of PARP inhibitor-based therapy. The present analysis provides reassuring evidence that declines in quality of life associated with anemia are transient and can be ameliorated with timely supportive care and treatment modification, allowing patients to continue benefiting from talazoparib plus enzalutamide.
Presented by: Neal Shore, MD, FACS, Urologist, Director, CPI, Carolina Urologic Research Center, Atlantic Urology Clinics, Myrtle Beach, SC
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
References:
- Agarwal N, Azad AA, Carles J, et al. Talazoparib plus enzalutamide in men with metastatic castration-resistant prostate cancer: Final overall survival results from the randomised, placebo-controlled, phase 3 TALAPRO-2 trial. Lancet. 2025;406(10502):447–460.
- Matsubara N, Azad AA, Agarwal N, et al. First-line talazoparib plus enzalutamide versus placebo plus enzalutamide for metastatic castration-resistant prostate cancer: Patient-reported outcomes from the randomised, double-blind, placebo-controlled, phase 3 TALAPRO-2 trial. Lancet Oncol. 2025;26(4):470–480.