(UroToday.com) The 2026 American Urologic Association (AUA) Annual Meeting was host to an advanced prostate cancer poster session. Dr. Yosuke Yasuda presented the results of a propensity-weighted and Bayesian restricted mean survival time (RMST) analysis of the prospective YUSHIMA Registry evaluating real-world outcomes of triplet intensification in high-volume, metastatic hormone-sensitive prostate cancer (mHSPC) in Japanese patients.
Triplet therapy with androgen deprivation therapy (ADT), docetaxel, and an androgen receptor pathway inhibitor (ARPI) has emerged as a standard treatment option for fit patients with de novo high-volume mHSPC following the positive results of ARASENS and PEACE-1.1,2 However, direct comparative evidence versus ARPI-based doublet therapy remains limited, particularly in Asian populations that may differ in treatment patterns, comorbidity profiles, and tolerability.
The objective of this study was to compare triplet therapy with ARPI-based doublet therapy for time to castration-resistant prostate cancer (CRPC) and to explore whether the incorporation of external phase III trial data through Bayesian borrowing would alter estimates of treatment effect.
The investigators analyzed 140 patients with CHAARTED-defined high-volume mHSPC from the multicenter, prospective YUSHIMA registry in Japan who were treated between 2021 and 2024. To account for treatment-selection bias, the primary analysis used overlap weighting, a propensity score–based approach that emphasizes patients with characteristics compatible with either treatment strategy. Treatment effects were evaluated using RMST, which estimates the average event-free survival time over a fixed time horizon and can provide a clinically intuitive measure when proportional hazards assumptions may not hold.
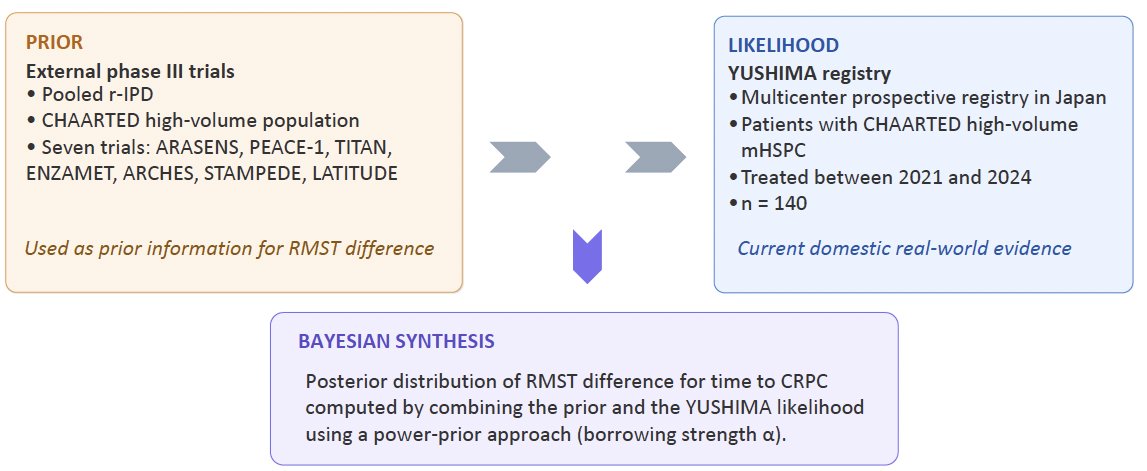
A distinctive feature of this study was the Bayesian synthesis framework illustrated in the central methods figure. External evidence from seven phase III trials—ARASENS, PEACE-1, TITAN, ENZAMET, ARCHES, STAMPEDE, and LATITUDE—was reconstructed into individual patient-level data and used as prior information. These prior data were then combined with the observed YUSHIMA registry likelihood using a power-prior approach, in which the parameter α governed the degree of borrowing from external evidence: α=0 indicated no borrowing, α=0.5 moderate borrowing, and α=1 full borrowing.

The unadjusted and overlap-weighted Kaplan–Meier curves (Figures A and B) demonstrated no statistically significant difference in time to CRPC between triplet and ARPI-based doublet therapy, both before and after propensity adjustment. These findings suggest that, within this Japanese real-world cohort, triplet intensification did not clearly outperform doublet therapy using conventional comparative methods.

The Bayesian analyses provided additional insight. Posterior distributions of the RMST difference at 12 months (Figure C) and 24 months (Figure D) shifted progressively toward favoring triplet therapy as greater weight was assigned to external phase III data. At the same time, the posterior distributions became narrower, indicating improved precision of the estimated treatment effect.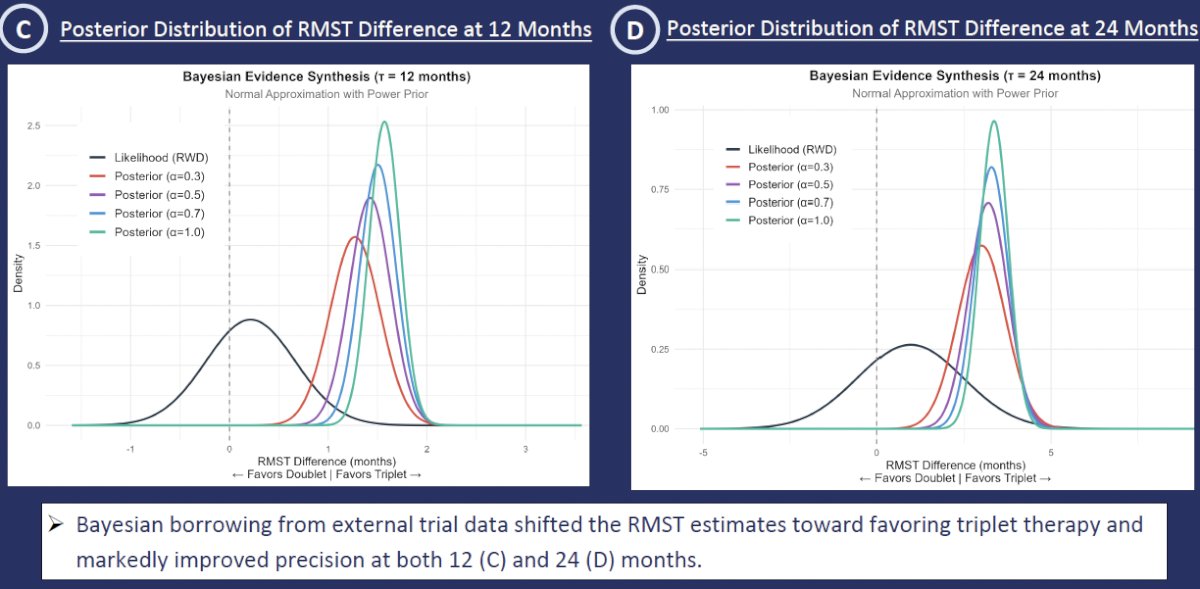
Under moderate borrowing (α=0.5), the posterior estimates suggested a CRPC-free RMST benefit of approximately 1.4 months at 12 months (Figure E) and 3.2 months at 24 months (Figure F) in favor of triplet therapy.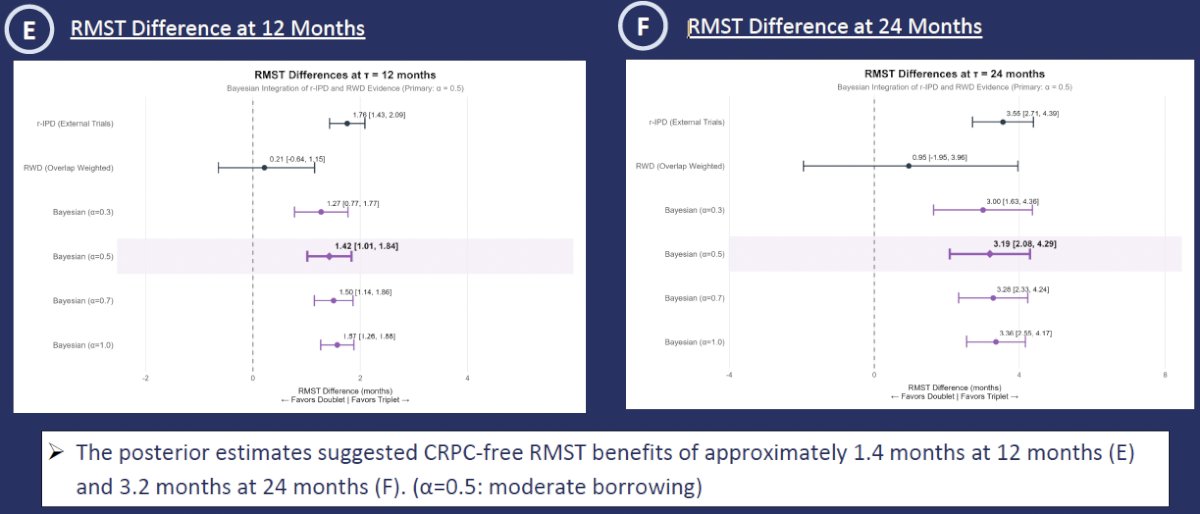
The sensitivity analysis shown in Figure G confirmed that increasing the degree of borrowing resulted in slightly larger estimated RMST benefits and tighter credible intervals, underscoring that the magnitude and certainty of benefit were substantially influenced by the strength of external evidence incorporated into the model.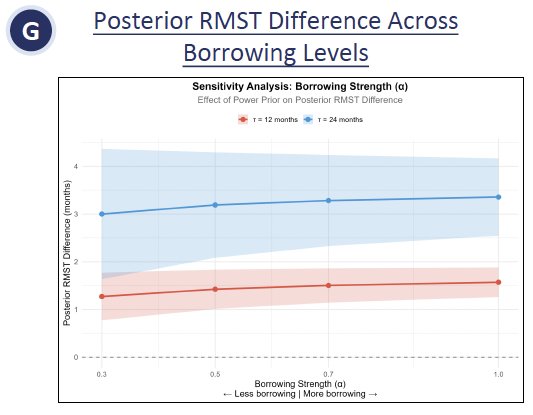
The investigators concluded that, in this propensity-weighted prospective registry analysis, triplet therapy was not clearly superior to ARPI-based doublet therapy for delaying progression to CRPC in Japanese patients with high-volume mHSPC. Exploratory Bayesian borrowing from external randomized trials suggested a modest CRPC-free benefit with triplet therapy, but this finding was highly dependent on prior information rather than the domestic real-world data alone.
These results highlight both the potential and the limitations of translating global phase III evidence into regional practice settings. They also illustrate how Bayesian borrowing may serve as a powerful analytic tool to contextualize real-world outcomes, particularly when local sample sizes are limited.
Presented by: Yosuke Yasuda, MD, Department of Urology, Institute of Science Tokyo, Tokyo, Japan
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
References:
- Smith MR, Hussain M, Saad F, et al. Darolutamide and survival in metastatic, hormone-sensitive prostate cancer. N Engl J Med. 2022;386(12):1132–1142.
- Fizazi K, Foulon S, Carles J, et al. Abiraterone plus prednisone added to androgen deprivation therapy and docetaxel in de novo metastatic castration-sensitive prostate cancer (PEACE-1): A multicentre, open-label, randomised, phase 3 study with a 2 × 2 factorial design. Lancet. 2022;399(10336):1695–1707.