(UroToday.com) The 2026 American Urological Association annual meeting featured the International Prostate Forum and a presentation by Dr. Jacqueline Brown discussing doublet versus triplet and who needs additional treatment intensification for metastatic hormone-sensitive prostate cancer (mHSPC). The concept of triplet therapy, defined as chemotherapy + androgen receptor pathway inhibitor + ADT, was first introduced 5 years ago. PEACE-11 and ARASENS2 showed that the addition of an androgen receptor pathway inhibitor to docetaxel and ADT improved overall survival:

However, what these two studies do not tell us is whether all patients need chemotherapy, considering that the control arm was docetaxel + ADT in each trial.
Dr. Brown used a meta-analysis from Riaz et al.3 highlighting 9 prospective doublet and triplet studies as a surrogate for the debate on who really benefits from docetaxel.
The following forest plot shows that the most benefit from chemotherapy is in patients with high-volume disease, defined by the CHAARTED criteria, and patients with de novo synchronous disease:
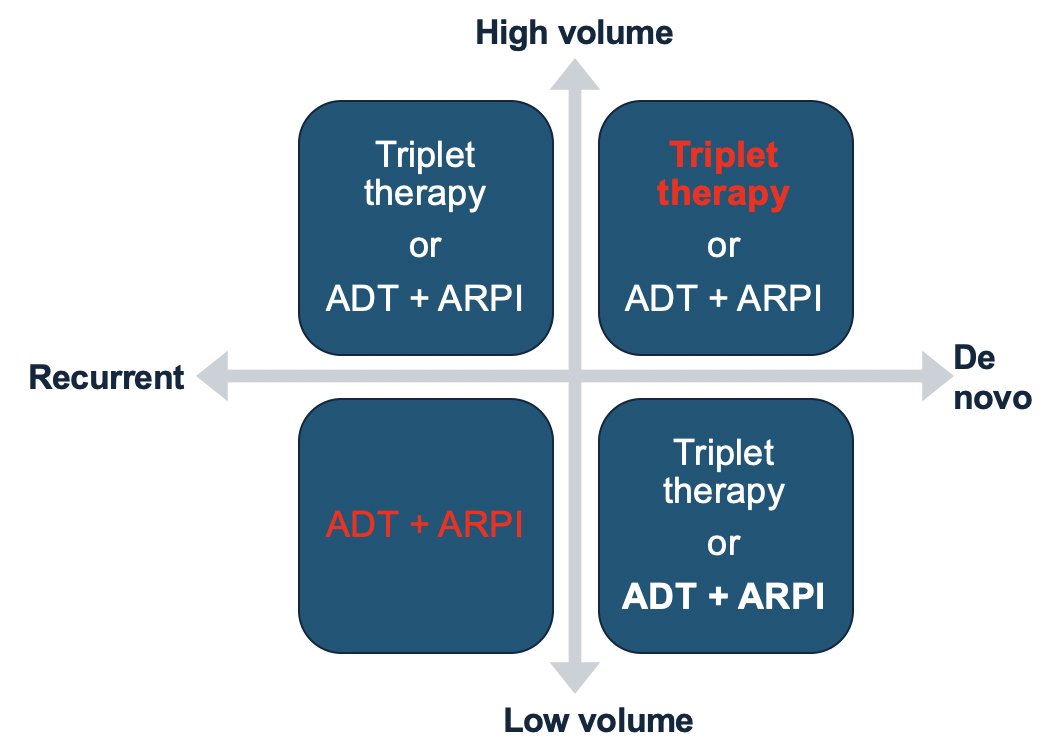
Along the lines of volume and timing, Dr. Brown encourages triplet therapy for patients with high-volume mHSPC, as well as for those with de novo disease, and recommends doublet therapy in recurrent low-volume disease:
Additionally, we should consider chemotherapy for patients who are fitter, younger, with a low PSA, as well as those with visceral disease and patients who are symptomatic at diagnosis. Dr. Brown considers omitting chemotherapy for patients with a SPOP mutation, given that we know this portends sensitivity to hormonal therapy. Of course, if a patient does not want chemotherapy (for whatever reason), our job is to meet the patient where they are at, knowing that we at least have excellent doublet therapy options.
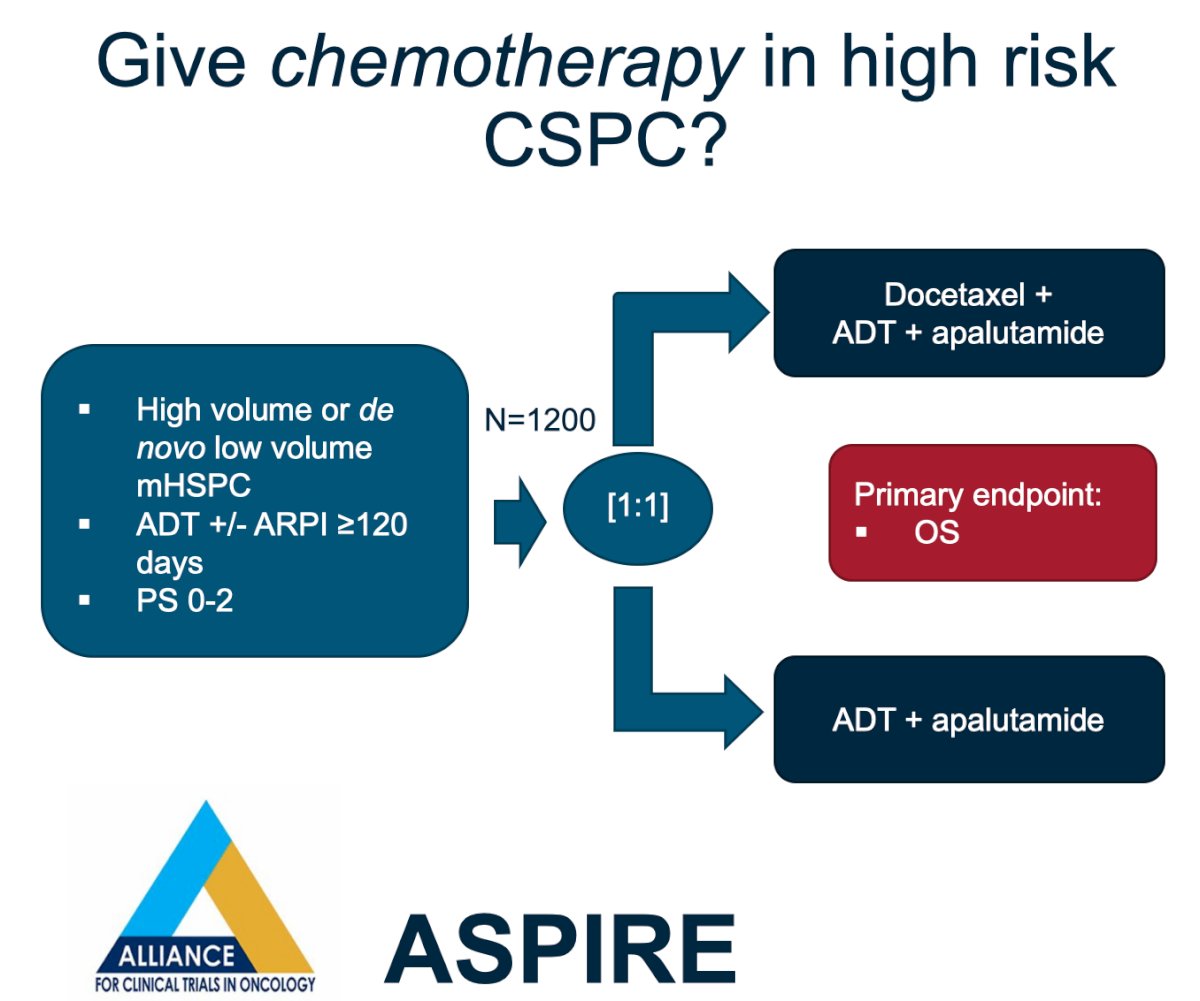
Dr. Brown also highlighted two important studies that will further clarify the role of chemotherapy in mHSPC. The first is the ASPIRE study, in which patients with high volume or low volume de novo disease will be randomized to ADT + apalutamide + docetaxel versus the control arm ADT + apalutamide:
The second trial is the TRIPLE-SWITCH trial, in which patients with mHSPC with a suboptimal PSA response, defined as a PSA > 0.2 ng/mL at 6 months of treatment, will be randomized to 6 cycles of chemotherapy or continuation of their doublet:

Dr. Brown emphasized that it is now officially time to unlink “triplet therapy” and chemotherapy in mHSPC. The four new triplets in mHSPC are:
- ADT + androgen receptor pathway inhibitor + PARP inhibitors
- ADT + androgen receptor pathway inhibitor + 177Lu-PSMA-617 radioligand therapy
- ADT + androgen receptor pathway inhibitor + AKT inhibitor
- ADT + androgen receptor pathway inhibitor + radiotherapy
ADT + androgen receptor pathway inhibitor + PARP inhibitors
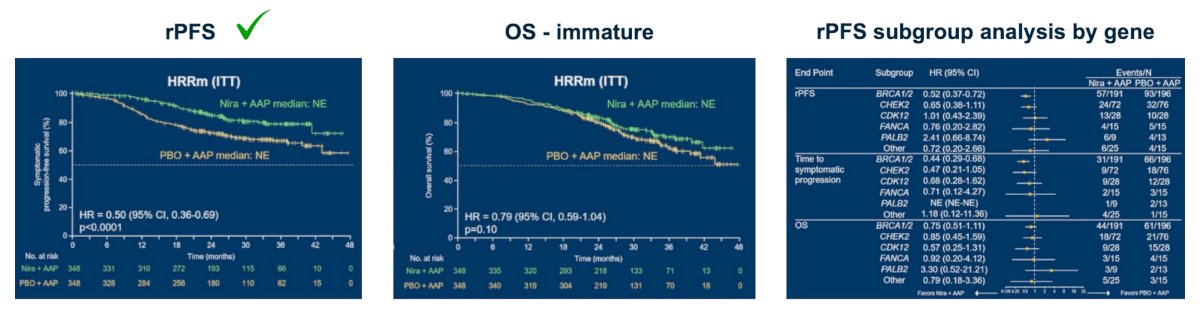
The AMPLITUDE study investigated patients with mHSPC with alterations in a variety of HRR genes, randomizing patients to niraparib + abiraterone + ADT versus abiraterone + ADT, with a primary endpoint of radiographic progression-free survival:4

Adding niraparib to abiraterone improved radiographic progression-free survival by 50% (HR 0.50, 95% CI 0.36-0.69), and there was a trend toward benefit in overall survival in the intention-to-treat population at the time of this interim analysis. When stratified by HRR mutation, the benefit in radiographic progression-free survival was driven by BRCA1 and BRCA2 compared to other mutations:
The results of AMPLITUDE led to the FDA approval of niraparib and abiraterone for BRCA2-mutated mHSPC in December 2025, and that approval is now reflected in NCCN guidelines. Dr. Brown notes that in addition to AMPLITUDE, we await results from TALAPRO-3 and the EvoPAR study, which will further clarify the role for PARP inhibitors in mHSPC:

Remaining questions/concerns regarding PARP inhibitors in mHSPC include:
- What is the role of PARP inhibitors in non-BRCA2 mutation patients?
- Since we do not have mature overall survival data yet, and 36% of patients on the control arm subsequently received PARP inhibitors, we need more time to determine the true benefit in this disease state
- PARP inhibitors carry a side effect profile of cytopenias and gastrointestinal upset, capable of changing the patient experience of mHSPC, a time often characterized by a slower pace of disease and good quality of life
ADT + androgen receptor pathway inhibitor + 177Lu-PSMA-617 radioligand therapy
PSMAddition examined a population of patients with mHSPC with at least one PSMA-positive lesion, randomizing patients to doublet therapy with or without 6 cycles of 177Lu-PSMA-617, with a primary endpoint of radiographic progression-free survival:
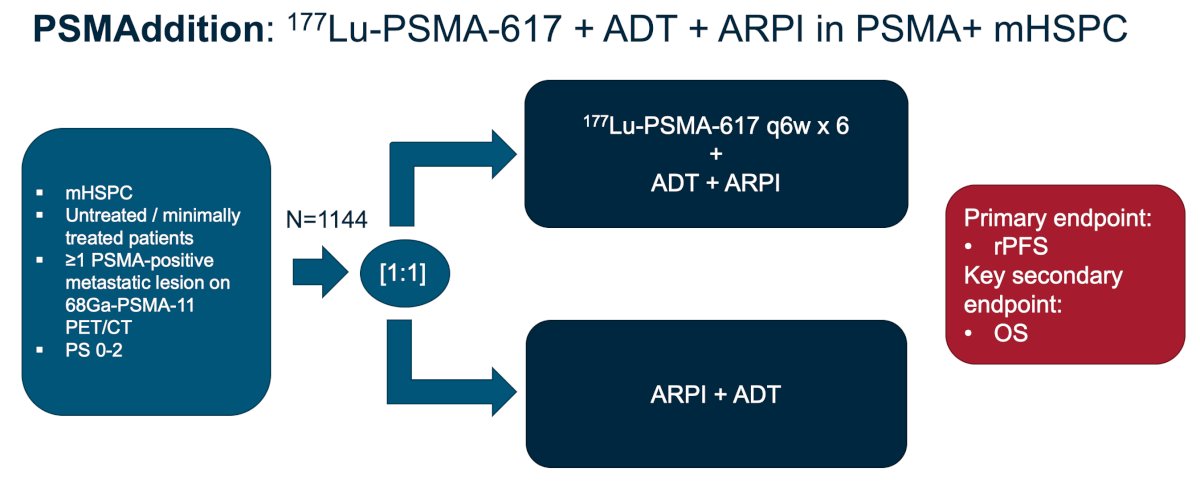
The addition of 177Lu-PSMA-617 reduced the risk of radiographic progression by 28%, and the overall survival data trended toward significance, although this was immature at the time of the primary analysis:

Similar to PARP inhibitors, we remain interested in the sequencing of these therapies when an overall survival benefit is difficult to prove, as patients live for years and receive many additional therapies. The hunt for refining biomarkers of response to PSMA targeted therapy is ongoing, and is greater than just PSMA SUVmean. Additionally, Dr. Brown wonders about the cumulative myelosuppression starting 177Lu-PSMA-617 earlier in the disease course and the impact this will have on later-line treatment options at the time of mCRPC.
ADT + androgen receptor pathway inhibitor + AKT inhibitor
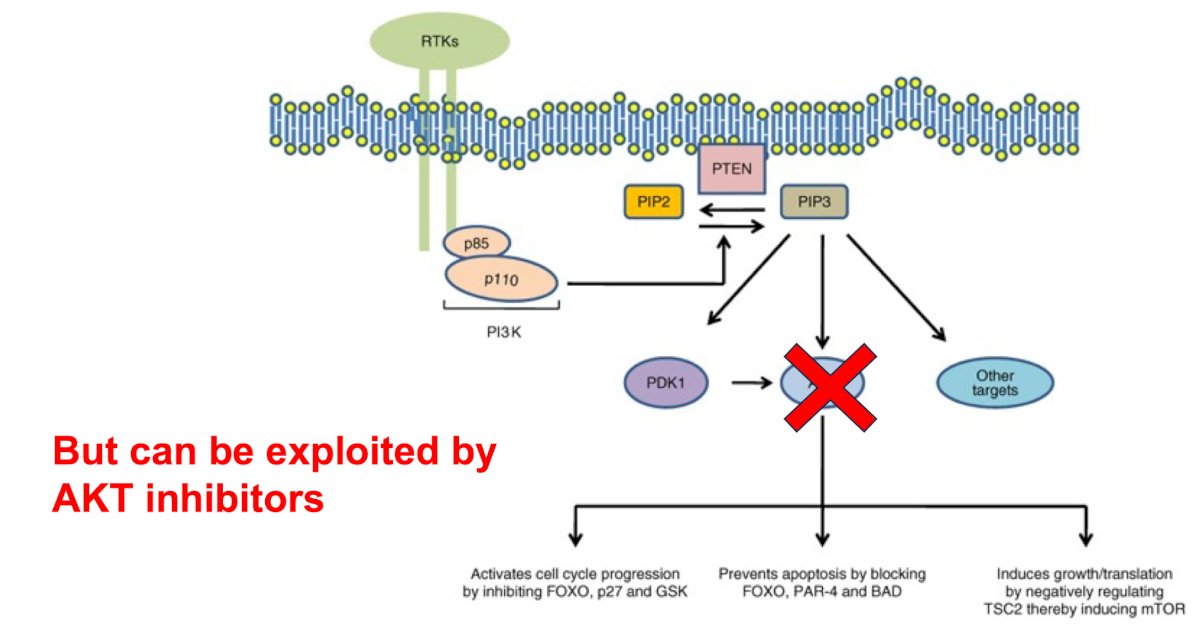
Dr. Brown notes that PTEN deficiency leads to upregulation of cancer growth and worse prognosis in patients with prostate cancer. However, this deficiency can be exploited by AKT inhibitors, which block one of the upregulated downstream growth pathways:
CAPItello-281 investigated capivasertib, an AKT inhibitor, with abiraterone + ADT versus abiraterone + ADT alone in patients with de novo mHSPC and PTEN deficiency. Among ~6,200 patients submitting tumor tissue, 97% had a valid IHC result, and 25% were PTEN deficient:
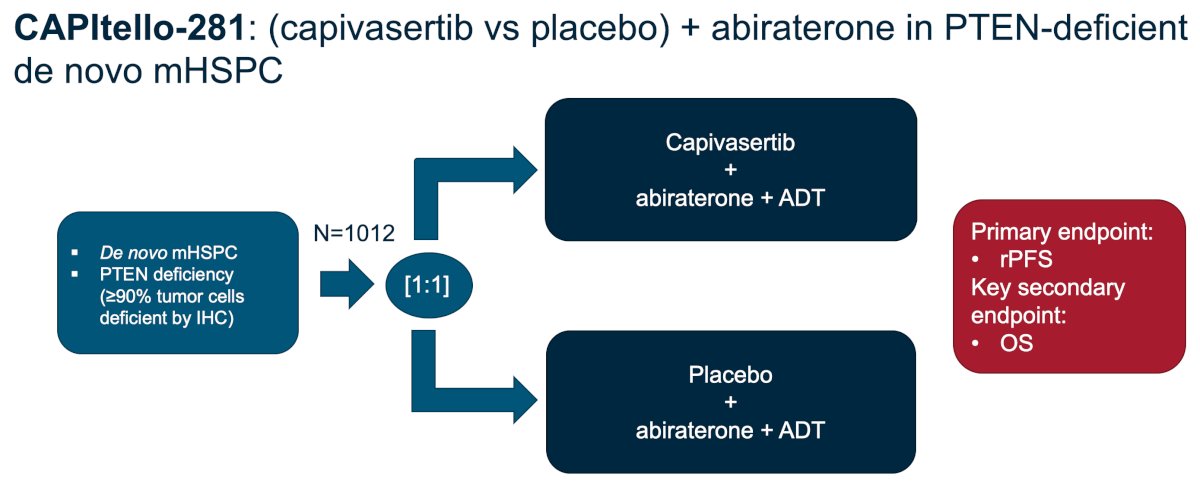
CAPItello-281 showed an improvement in radiographic progression-free survival (HR 0.81, 95% CI 0.66-0.98) for the addition of capivasertib, but did not show a benefit in overall survival; however the data are immature:5
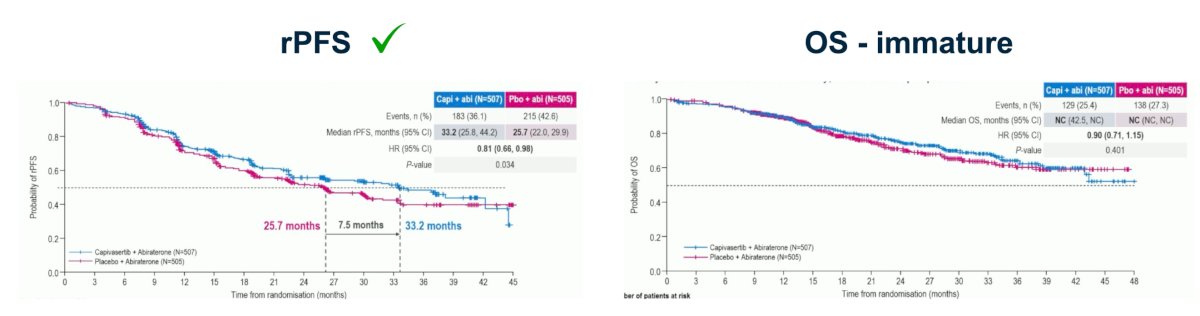
Dr. Brown notes that what is important is that capivasertib introduces a new profile of side effects – diarrhea, rash, and hyperglycemia. As such, we have to balance an efficacy benefit with quality of life in these patients with mHSPC who have a poor prognosis associated with PTEN deficiency, but with the potential to modulate this outcome with AKT inhibitors:

ADT + androgen receptor pathway inhibitor + primary radiotherapy
Previously, the STAMPEDE trial showed us that prostate radiation improved survival in low-volume but not high-volume disease:6

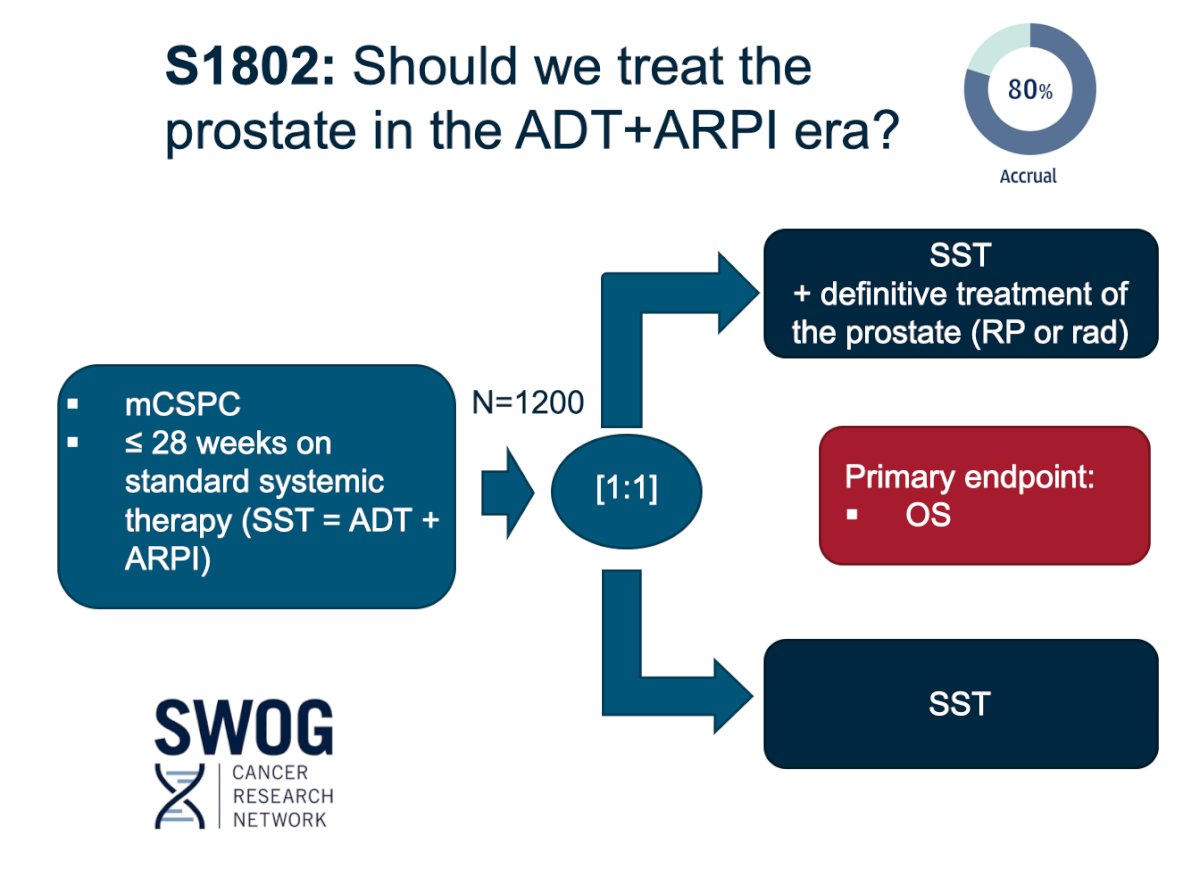
The SWOG S1802 study will help to clarify whether we should treat the prostate in the doublet era and with what modality, as patients randomized to the standard systemic therapy + intervention arm can choose between surgery and radiation therapy:
Dr. Brown provided the current treatment algorithm for mHSPC in the figure below. If the patient has high-volume disease, we can consider triplet therapy (defined by the addition of chemotherapy). If the patient has low volume de novo mHSPC, we can also consider a triplet for selected patients, but this is a group to consider prostate radiotherapy if the S1802 trial is not available. For most patients, we probably do not need to intensify treatment for patients with low volume, recurrent disease. As of December 2025, we have niraparib + abiraterone for patients with BRCA2 mutations, highlighting the importance of upfront genomic testing:

However, the future of treatment intensification may be more complicated and require careful attention to each patient’s imaging, disease course to date, and pathology (both genomics and IHC). For those with high volume or de novo disease, we may still consider docetaxel. But there will be overlap between those patients and the patients in whom we find BRCA2 mutations, where we may opt for niraparib + abiraterone + ADT. Moreover, those who are strongly PSMA positive may benefit from the addition of 177Lu-PSMA-617, or those who are PTEN deficient may benefit from capivasertib:

Dr. Brown concluded her presentation discussing doublet versus triplet and who needs additional treatment intensification for mHSPC with the following take-home points:
- Androgen receptor pathway inhibitor + ADT is the minimum treatment for mHSPC patients
- Biomarker testing is key
- A multidisciplinary alliance between urology and medical oncology, along with our radiation oncology colleagues, is more important than ever
- Ultimately, our patients’ goals and values for this currently incurable illness will lead us as we discuss treatment intensification options with them
Presented by: Jacqueline Brown, MD, Oncologist, Assistant Professor, Department of Hematology and Medical Oncology, Winship Cancer Institute of Emory University, Atlanta, GA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
References:
- Fizazi K, Foulon S, Carles J, Roubaud G, et al. Abiraterone plus prednisone added to androgen deprivation therapy and docetaxel in de novo metastatic castration-sensitive prostate cancer (PEACE-1): A multicentre, open-label, randomized, phase 3 study with a 2 x 2 factorial design. Lancet. 2022 Apr 30;399(10336):1695-1707.
- Smith MR, Hussain M, Saad F, et al. Darolutamide and Survival in Metastatic, Hormone-Sensitive Prostate Cancer. N Engl J Med. 2022 Mar 24;386(12):1132-1142.
- Riaz IB, Naqvi SAA, He H, et al. First-line systemic treatment options for metastatic castration-sensitive prostate cancer: A living systematic review and network meta-analysis. JAMA Oncol. 2023 May 1;9(5):635-645.
- Attard G, Agarwal N, Graff JN, et al. Niraparib and abiraterone acetate plus prednisone for HRR-deficient metastatic castration-sensitive prostate cancer: A randomized phase 3 trial. Nat Med. 2025 Dec;31(12):4109-4118.
- Fizazi K, Clarke NW, De Santis M, et al. Capivasertib plus abiraterone in PTEN-deficient metastatic hormone-sensitive prostate cancer: CAPItello-281 phase III study. Ann Oncol. 2026 Jan;37(1):53-68.
- Parker CC, James ND, Brawley CD, et al. Radiotherapy to the primary tumour for newly diagnosed, metastatic prostate cancer (STAMPEDE): A randomized controlled phase 3 trial. Lancet 2018 Dec 1;392(10162):2353-2366.