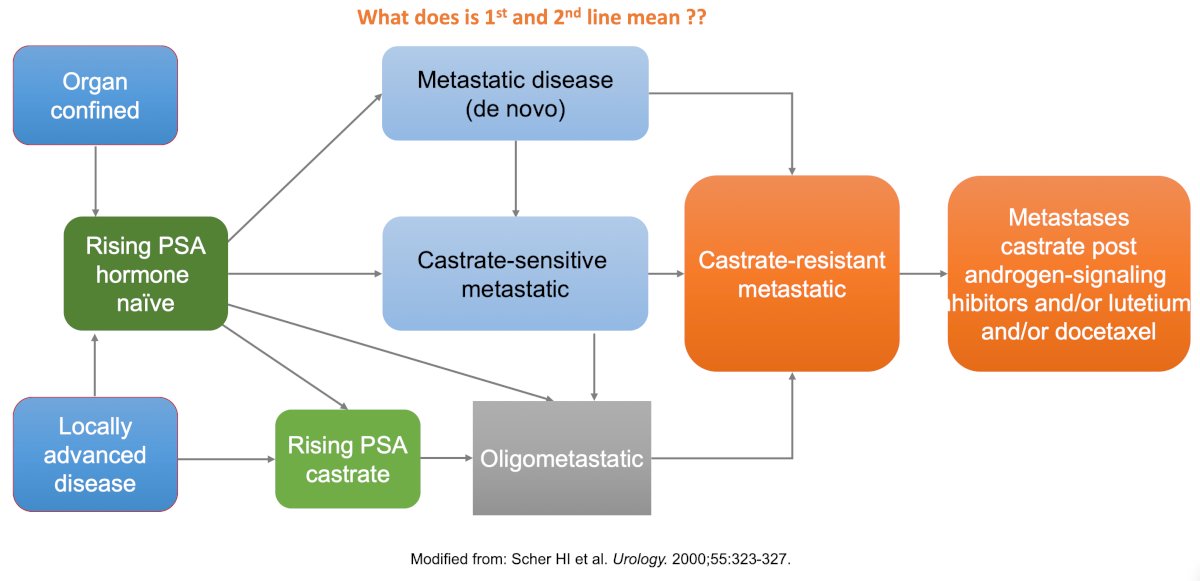
(UroToday.com) The 2026 American Urological Association annual meeting featured the International Prostate Forum and a presentation by Dr. Robert Dreicer discussing what’s next after first and second-line metastatic castration resistant prostate cancer (mCRPC) treatment. Dr. Dreicer started his presentation by noting that the current management of mCRPC comprises disease and clinician heterogeneity + essentially no prospective data regarding the optimal therapy sequence. Moreover, the clinical state of prostate cancer in May 2026 remains essentially unchanged since the year 2000:
Furthermore, during the last several decades, moving from estramustine all the way to 177Lu-PSMA-617, there has been very little improvement in overall survival in the mCRPC disease state: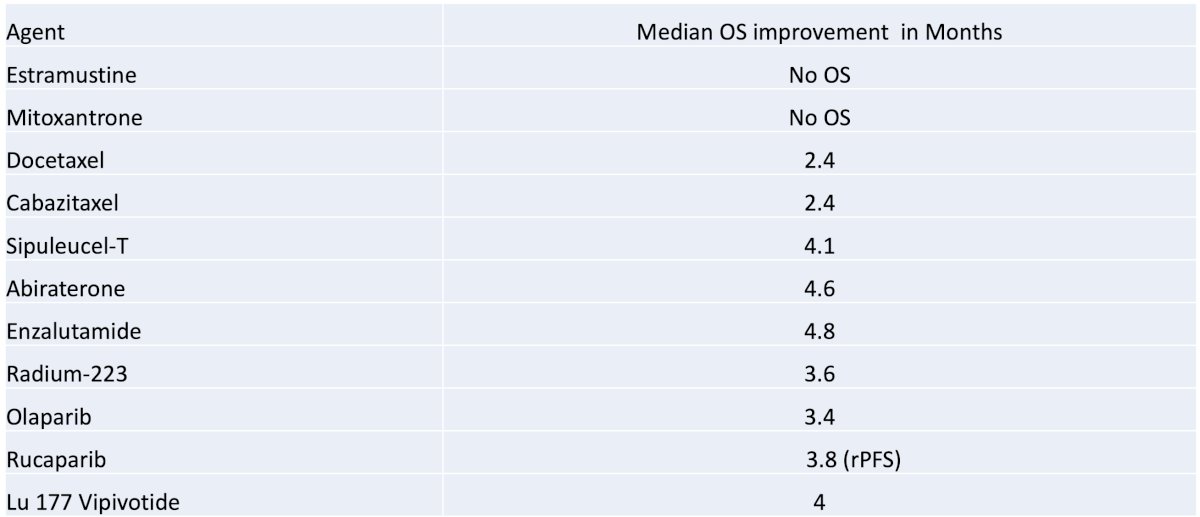
What are the goals of care for an incurable disease like mCRPC? Dr. Dreicer notes the following:
- Improve overall survival
- Maintain quality of life
- Some advocate ensuring that patients receive all active agents as a strategy to obtain maximal survival
- However, individual patient disease biology at times allows periods of expectant management
- What we want for the future are agents that can lead to a “shoulder on the survival curve” with the potential for treatment-free intervals
- This will likely require some form of an immunomodulatory approach
With regards to immune checkpoint inhibitors, Dr. Dreicer emphasizes that we have tried, tried again, tried in combination with every drug we can think of, but the bottom line is these agents do not work in mCRPC, with the exception of patients with MSI-H/dMMR or TMB-H (pembrolizumab). For the remainder of his presentation, Dr. Dreicer highlighted next-generation immunomodulatory/cellular therapeutic agents in mCRPC (selected agents). The first group is the bispecific T-cell engagers:
- Xaluritamig (AMG 509): STEAP1 x CD3 XmAb 2+1 bispecific that is in an ongoing phase III trial
- Acapatamab (AMG 160): PSMA targeted
- REGN5678: PSMA targeted
- VIR-5500: PSMA-targeted dual-masked T-cell engager
Second, there is CAR-T (chimeric antigen receptor) cell therapy:
- P-PSMA-101
- AZD0754: STEAP 2 targeted
- CART-PSMA-TGFBetaRdn
- PSCA-CAR T: prostate stem cell antigen targeted
In a phase I study, the STEAP-1 targeting bi-specific T cell engager, Xaluritamig (AMG 509), was evaluated in heavily pre-treated mCRPC patients who had progressed on a prior androgen receptor pathway inhibitor and a taxane.1 Notably, there were 53% of patients who had visceral metastases, including 37% with liver metastases. A PSA50 response was observed in 49% of patients, and a PSA90 response was observed in 30%.
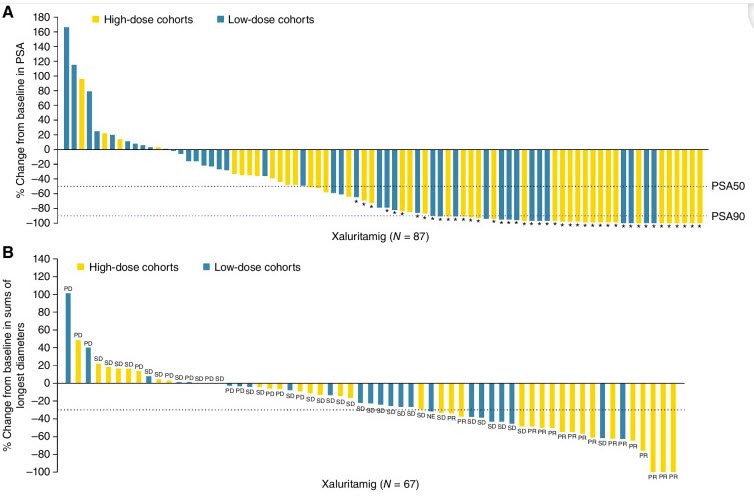
From a safety standpoint, cytokine release syndrome was present in ~70% of patients. However, only 3% of patients discontinued this drug because of cytokine release syndrome.
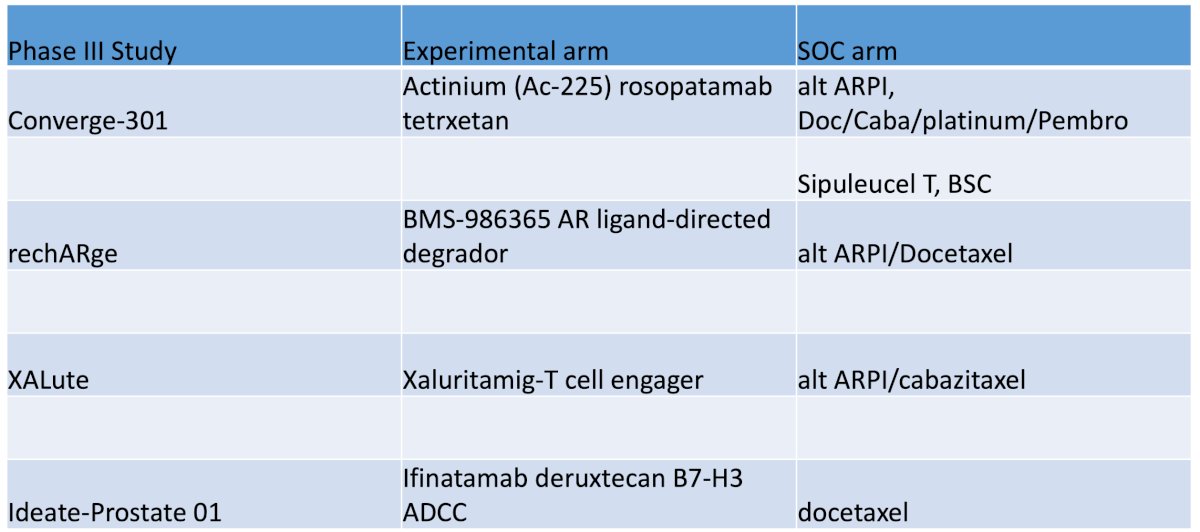
There are several challenges for novel cellular therapeutics in mCRPC, including established efficacy, cytokine release syndrome (the difference between a broadly applicable therapy versus a referral center-only approach), and cost. Dr. Dreicer finished his presentation with the following table showing trials with active control arms in this disease space:
Dr. Dreicer concluded his presentation discussing what’s next after first and second line mCRPC treatment with the following take-home points:
- The mCRPC space is increasingly appropriately impacted by earlier movement of next-generation androgen receptor-directed therapies
- Known pathways resulting in androgen receptor resistance limit the utility of crossover of current agents
- NGS testing is mandatory but infrequently done
- Clinical factors
- Symptoms yes/no
- Biochemical or overt radiographic progression
- Prior therapies
- Durability of initial ADT response
- We need adequately powered trials with active control arms to establish treatment paradigms, at least at a high level
Presented by: Robert Dreicer, MD, University of Virginia Cancer Center, Charlottesville, VA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
Reference:
- Kelly WK, Danila DC, Lin CC, et al. Xaluritamig, a STEAP1 x CD3 XmAb 2+1 Immune Therapy for Metastatic Castration-Resistant Prostate Cancer: Results from a Dose Exploration in a First-in-Human Study. Cancer Discov. 2024 Jan 12;14(1):76-89.