(UroToday.com) The American Urological Association's 2026 Annual Meeting, between May 15 – May 18, 2026 in Washington D.C., was host to the Interactive Poster IP38: Prostate Cancer: Advanced I Session. Dr. Jason Hafron presented interactive poster IP38-17: Implementation of a Multidisciplinary Quality Initiative to Mitigate and Reduce the Side Effects of Androgen Deprivation Therapy (ADT) in Prostate Cancer Patients Based on the Prostate Cancer 360 (PC360) Working Group Recommendations.
Dr. Hafron began by noting that androgen deprivation therapy remains a cornerstone of prostate cancer treatment but is associated with substantial treatment-related morbidity. Although the cardiometabolic, skeletal, sexual, and psychological adverse effects of ADT are well recognized, these complications are frequently under-recognized and inconsistently managed in routine clinical practice.
He highlighted that this gap largely reflects the lack of practical and integrated care frameworks to guide comprehensive ADT management across specialties. To address this unmet need, the Prostate Cancer 360 (PC360) Working Group convened a multidisciplinary panel to develop structured, consensus-driven recommendations focused on proactive monitoring, prevention, risk mitigation, and longitudinal management of ADT-associated toxicities throughout the continuum of care.
The PC360 Working Group convened 14 multidisciplinary experts in prostate cancer and ADT management to systematically identify current gaps and challenges in recognizing and managing ADT-related adverse effects. Using a structured consensus-driven process, the panel developed practical, prescriber-focused recommendations intended to support routine clinical implementation. The expert panel included specialists from urology, medical oncology, cardiology, endocrinology, primary care, and survivorship care.

Dr. Hafron explained that PC360 was designed as a structured multidisciplinary care framework aimed at standardizing monitoring and management of ADT-associated toxicities across five core health domains. These domains informed broader recommendations supporting development of a Chronic Care Management model for patients receiving ADT, emphasizing coordinated multidisciplinary management of chronic comorbidities rather than a narrower Principal Care Management approach focused primarily on prostate cancer-directed therapy.
The five core health domains are incorporated within the PC360 framework for patients receiving ADT. These included cardiovascular health, emphasizing baseline and ongoing risk assessment, early statin consideration, and multidisciplinary collaboration with primary care and cardiology; bone health, with recommendations for DEXA scanning, fracture risk assessment, vitamin D/calcium supplementation, and antiresorptive therapy when appropriate; psychological health, including routine screening for depression, anxiety, emotional lability, and cognitive changes using validated tools such as PHQ-2/9 and GAD-2/7; sexual health, focusing on expectation-setting, partner involvement, and reframing discussions beyond erectile function alone; and metabolic/body composition changes, with strong emphasis placed on physical activity, nutrition, and behavioral modification as foundational interventions during ADT.
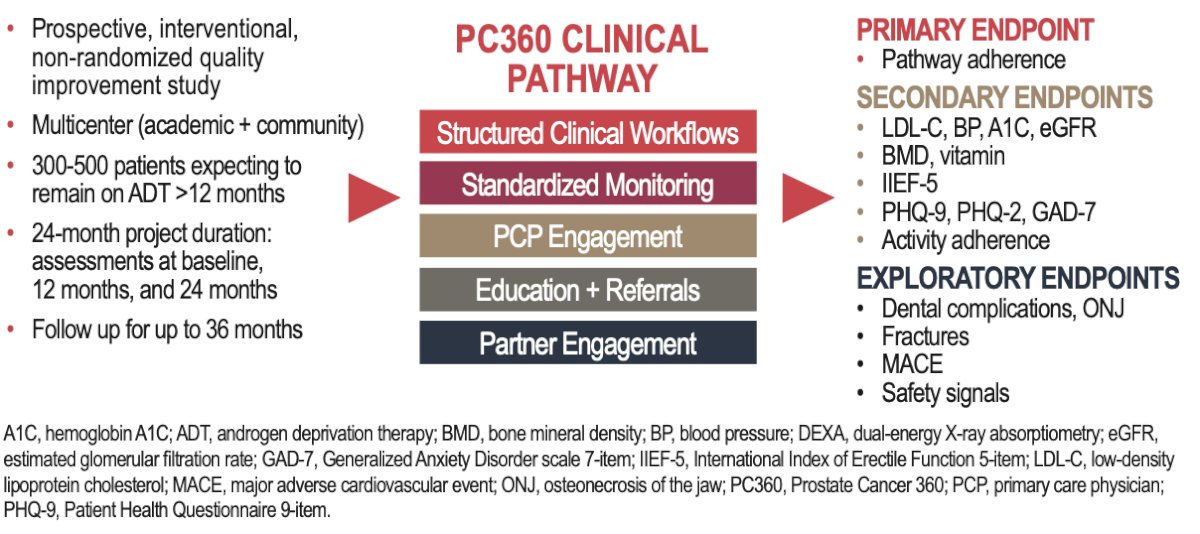
This study was a prospective, interventional, non-randomized quality improvement study evaluating the implementation of the PC360 recommendations across both academic and community practices. Patients receiving ADT who were expected to remain on therapy for more than 12 months were enrolled in a Chronic Care Management program incorporating multidisciplinary monitoring across five predefined health domains.
The planned enrollment included approximately 300–500 patients, with assessments performed at baseline, 12 months, and 24 months, and follow-up extending up to 36 months. The PC360 clinical pathway incorporated structured clinical workflows, standardized monitoring, primary care physician engagement, education and referral strategies, and partner engagement.
The primary endpoint was adherence to the PC360 care pathway. Secondary endpoints included cardiometabolic, skeletal, sexual, psychological, and lifestyle-related measures such as LDL cholesterol, blood pressure, hemoglobin A1c, eGFR, bone mineral density, vitamin D levels, IIEF-5, PHQ-9, PHQ-2, GAD-7, and physical activity adherence. Exploratory endpoints included dental complications, osteonecrosis of the jaw, fractures, major adverse cardiovascular events, and additional safety signals.
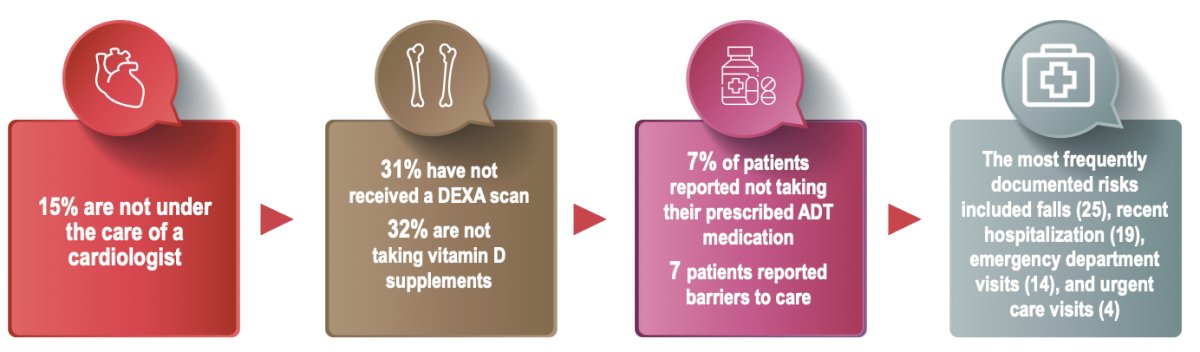
To date, 270 men have been enrolled in the PC360 program, with preliminary implementation results demonstrating successful integration of multidisciplinary care pathways, high patient engagement, and improved coordination across specialties. Early findings suggested improved monitoring of cardiometabolic risk factors and bone health, although longitudinal outcomes remain ongoing. Despite these advances, several gaps in supportive care were identified, including 15% of patients not being under the care of a cardiologist, 31% not having undergone DEXA scanning, and 32% not taking vitamin D supplementation. Additionally, 7% of patients reported not taking prescribed ADT medications, while barriers to care were identified in several patients. Commonly documented clinical risks included falls, recent hospitalizations, emergency department visits, and urgent care utilization.
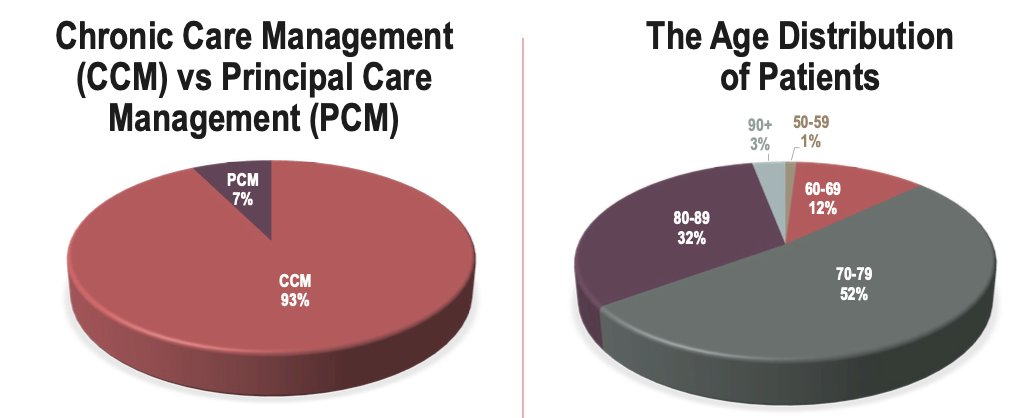
The investigators also highlighted that the vast majority of enrolled patients were managed using the Chronic Care Management framework rather than a traditional Principal Care Management approach, reflecting broad adoption of multidisciplinary longitudinal care strategies within the program. In terms of patient demographics, most participants were older adults, with 52% between 70–79 years of age and 32% between 80–89 years, emphasizing the importance of comprehensive supportive care in an aging prostate cancer population receiving ADT.
Moreover, the investigators developed an actionable clinical dashboard designed to longitudinally track patient outcomes across the five PC360 health domains, facilitate communication among multidisciplinary providers, and identify gaps in care delivery in real time, thereby supporting more coordinated and proactive management of ADT-associated toxicities.

Lastly, Dr. Hafron emphasized that chronic care management for patients receiving ADT should be centered around a multidisciplinary, patient-focused model integrating urologists, oncologists, primary care physicians, cardiologists, psychologists, rehabilitation specialists, dietitians, social workers, and other allied health professionals. He stressed the importance of ensuring patients have an engaged primary care physician, performing comprehensive baseline assessments for cardiometabolic, bone, sexual, and psychological health, and proactively intervening to mitigate cardiovascular and metabolic risks, including consideration of statin therapy when appropriate. He also highlighted the value of incorporating family members and caregivers into treatment discussions, referring patients with uncontrolled risk factors for specialized evaluation, and utilizing trained clinical staff to provide counseling and longitudinal supportive care across health domains impacted by ADT.
Dr. Hafron concluded with the following key messages:
- Implementation of the PC360 multidisciplinary care model appears feasible in routine clinical practice and provides a structured framework for proactive monitoring and management of ADT-associated morbidity
- Early findings suggest improved care coordination across specialties and enhanced identification of cardiometabolic, skeletal, and psychosocial risk factors in patients receiving ADT
- The PC360 model emphasizes longitudinal, multidisciplinary chronic care management rather than prostate cancer treatment alone
- Ongoing follow-up will further evaluate long-term clinical outcomes, adherence to care pathways, and the impact of structured supportive care interventions
- The presented results remain preliminary and reflect data from the initial enrollment phase of this ongoing study
Presented by: Jason Hafron, MD, CMO, Oncologist, Chief Medical Officer and Medical Director of Clinical Research, Michigan Institute of Urology, Solaris Health, MI
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
Related content: Implementation of the PC360 Algorithm to Manage Cardiovascular and Bone Health Risks on ADT - Jason Hafron