(UroToday.com) The American Urological Association's 2026 Annual Meeting, between May 15 – May 18, 2026 in Washington D.C., was host to the Interactive Poster IP38: Prostate Cancer: Advanced I Session. Dr. Takuma Kato presented interactive poster IP38-15: Real-World Treatment Sequence and Completion Outcomes of Radium-223 With Enzalutamide in Metastatic Castration-Resistant Prostate Cancer
Dr. Kato began by highlighting that the phase III PEACE-3 trial demonstrated improved radiographic progression-free survival with the combination of radium-223 plus enzalutamide compared with enzalutamide alone in patients with metastatic castration-resistant prostate cancer. Building upon these findings, the investigators sought to evaluate real-world treatment completion patterns and clinical outcomes associated with Ra-223–based therapy in routine practice settings.
For this retrospective multicenter study, the investigators analyzed patients with mCRPC treated with radium-223 across 84 Japanese institutions between 2020 and 2023. Patients received radium-223 in combination with ADT plus enzalutamide or ADT alone, while other concurrent systemic therapies were excluded. To minimize baseline imbalances between treatment groups, propensity score matching was performed. The primary endpoints included completion of all six planned cycles of radium-223 and treatment sequencing patterns, while secondary endpoints included progression outcomes, overall survival, and safety.
For statistical analyses, the investigators compared continuous variables using either the Mann–Whitney U test or Student’s t-test, as appropriate, while categorical variables were evaluated using chi-square testing. Overall survival and cancer-specific survival were estimated using Kaplan-Meier methodology.
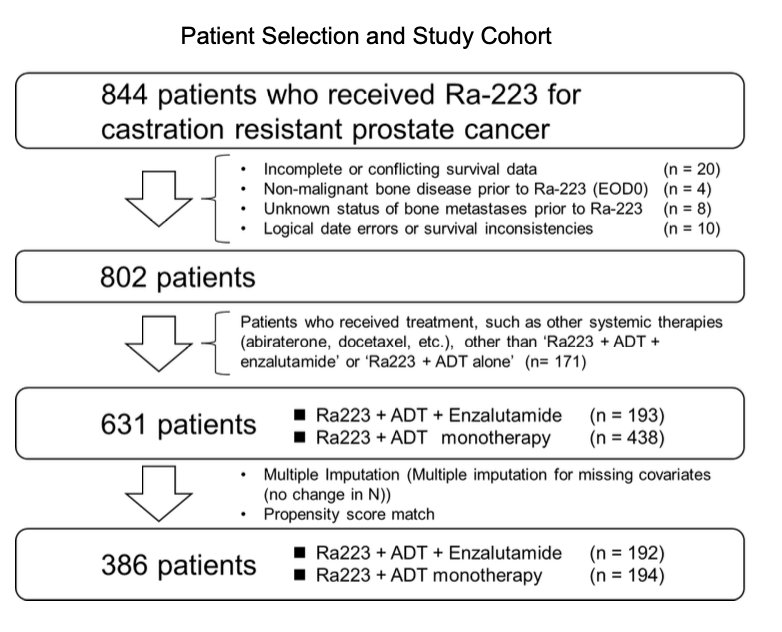
A total of 844 patients who received radium-223 for castration-resistant prostate cancer were initially identified. After exclusion of patients with incomplete survival data, non-malignant bone disease, unknown metastatic status, or data inconsistencies, 802 evaluable patients remained. The investigators then excluded patients receiving additional systemic therapies beyond the predefined study regimens, resulting in a final cohort of 631 patients treated with either radium-223 plus ADT and enzalutamide (n=193) or radium-223 plus ADT alone (n=438). Following multiple imputation for missing covariates and propensity score matching, the final matched analysis included 386 patients, with 192 patients in the radium-223 plus enzalutamide group and 194 patients in the ADT-alone group.
Dr. Kato highlighted that after propensity score matching, baseline characteristics between the treatment groups were well balanced. Median age was 74 years in both cohorts, and laboratory parameters, including PSA, ALP, LDH, CRP, albumin, and hemoglobin, were overall comparable between groups. Disease burden and functional status were also similar, with most patients demonstrating ECOG performance status 0–1 and extensive bone metastatic involvement across EOD classifications. Prior treatment exposure reflected a heavily pretreated mCRPC population, with widespread prior use of ARSI therapy and prior chemotherapy exposure, including docetaxel and cabazitaxel. Patient characteristics after propensity score matching are shown below.

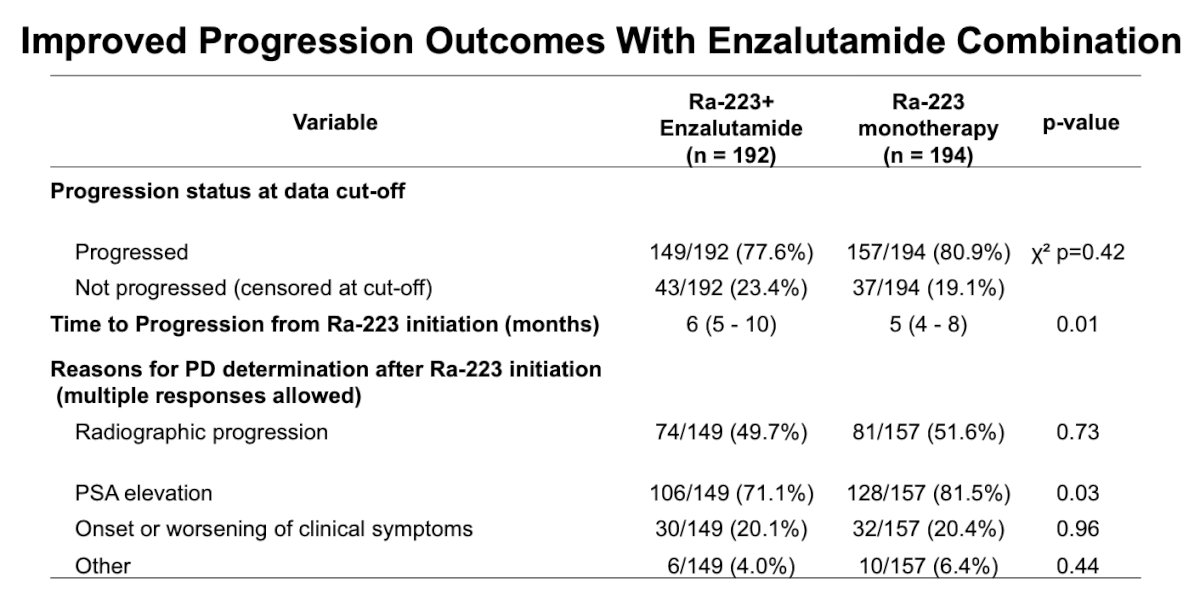
They highlighted that completion of all six planned cycles of radium-223 was high in both treatment groups, with no statistically significant difference between patients receiving ADT plus enzalutamide (77.6%) and those receiving ADT alone (72.7%). However, PSA kinetics favored the combination approach, as patients treated with ADT plus enzalutamide demonstrated significantly more favorable PSA changes compared with the ADT monotherapy cohort (p<0.0001).

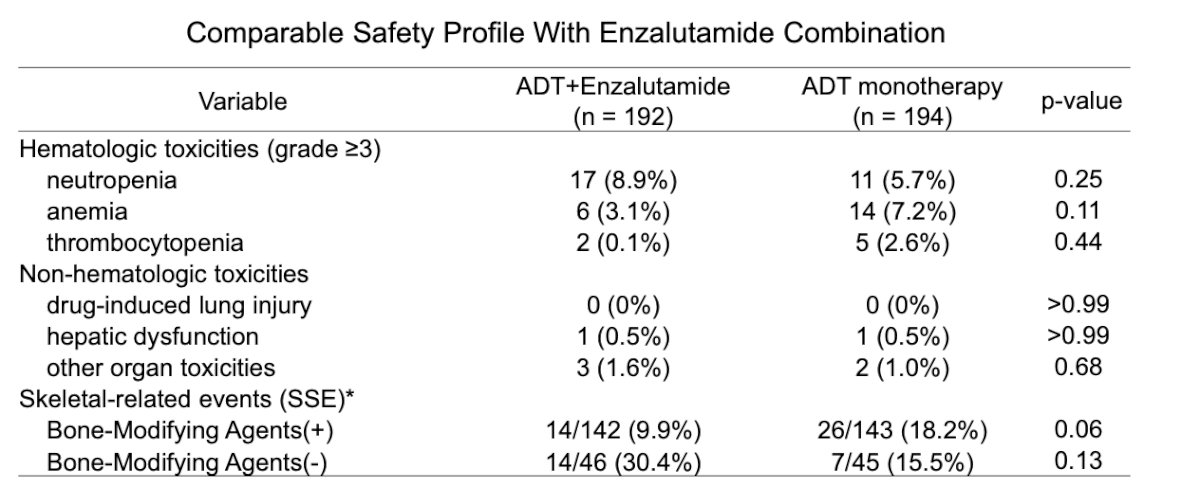
Notably, the safety profile was comparable between treatment groups, with no significant increase in grade ≥3 hematologic or non-hematologic toxicities observed with the addition of enzalutamide. Rates of neutropenia, anemia, thrombocytopenia, hepatic dysfunction, and other organ toxicities were overall similar across cohorts. Skeletal-related events were numerically lower among patients receiving bone-modifying agents in the combination arm, although these differences did not reach statistical significance.
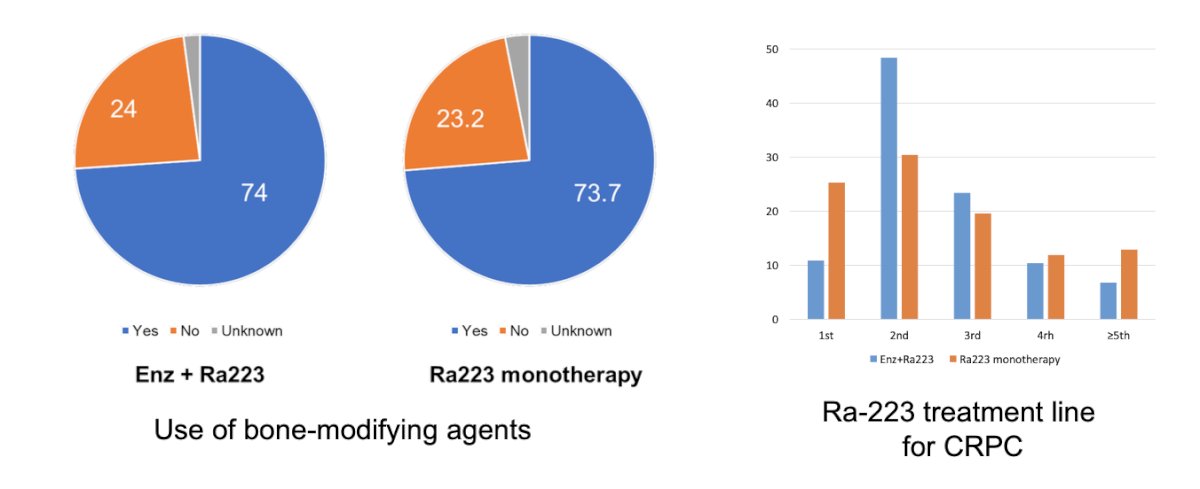
Dr. Kato highlighted that the use of bone-modifying agents was common and generally comparable between treatment groups, with approximately three-quarters of patients in both cohorts receiving concomitant bone-protective therapy during radium-223 treatment. They also noted differences in treatment sequencing, as radium-223 plus enzalutamide was more commonly administered earlier in the CRPC disease course, particularly as second-line therapy, whereas radium-223 monotherapy was more frequently used in later-line settings.
Lastly, Dr. Kato highlighted the impact of bone-modifying agents on symptomatic skeletal events. In the enzalutamide plus radium-223 cohort, patients receiving bone-modifying agents experienced significantly fewer skeletal-related events compared with those who did not receive them (9.9% vs 30.4%, p=0.0015). In contrast, no significant difference was observed in the radium-223 monotherapy group.
He also presented overall survival outcomes among patients who completed all six cycles of radium-223. Median overall survival was numerically longer in the enzalutamide combination cohort at 52 months compared with 36 months in the monotherapy cohort, although this difference did not reach statistical significance (p=0.58; HR 1.10, 95% CI 0.77–1.58).

Dr. Kato concluded with the following key messages:
- Radium-223 plus enzalutamide demonstrated high treatment completion rates and favorable tolerability in real-world clinical practice
• The combination approach improved disease control outcomes without increasing clinically significant toxicity
• These findings support the feasibility of combining radium-223 with enzalutamide in patients with mCRPC treated in routine practice settings
Presented by: Takuma Kato, MD, PhD, Assistant Professor, Department of Urology, Faculty of Medicine, Kagawa University Hospital, Miki, Kagawa, Japan
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
Reference: