(UroToday.com) The American Urological Association's 2026 Annual Meeting, between May 15 – May 18, 2026 in Washington D.C., was host to the Interactive Poster IP38: Prostate Cancer: Advanced I Session. Dr. Benjamin Lowentritt presented an interactive poster, IP38-21: Testosterone suppression and recovery in patients with advanced prostate cancer treated with relugolix: an interim analysis of the OPTYX study.
Dr. Lowentritt began by noting that relugolix is an oral gonadotropin-releasing hormone receptor antagonist approved for the treatment of advanced prostate cancer. He highlighted results from the pivotal phase III HERO trial, in which relugolix achieved sustained testosterone suppression below castrate levels in 96.7% of patients from day 29 through 48 weeks of therapy, with more than half of patients reaching castrate testosterone levels by day 4. Additionally, 54% of patients recovered testosterone levels back into the normal range within 90 days after treatment discontinuation, while rapid PSA responses were also observed, with nearly 80% of patients achieving a greater than 50% PSA decline by day 15.1
Despite these favorable clinical trial findings, Dr. Lowentritt emphasized that there remain limited real-world data evaluating the effectiveness of relugolix for testosterone and PSA suppression, as well as the kinetics and extent of testosterone recovery following treatment discontinuation in routine clinical practice.
The OPTYX study (NCT05467176) is an ongoing prospective, multicenter, long-term observational study evaluating real-world outcomes among US patients with prostate cancer treated with relugolix either as monotherapy or in combination with other systemic therapies. Relugolix monotherapy was defined as treatment without concurrent systemic prostate cancer therapy at enrollment, whereas combination therapy included relugolix administered alongside first- or second-generation androgen receptor pathway inhibitors, chemotherapy, PARP inhibitors, immunotherapy, or other systemic agents; radiation therapy was permitted but was not considered combination systemic therapy.
Patients were followed from enrollment through up to two years after treatment discontinuation or until the study end date in June 2026. Eligible patients were men aged 18 years or older who initiated relugolix within one month prior to enrollment, remained on treatment at study entry, and had an intended treatment duration of at least four months. Testosterone and PSA levels were assessed longitudinally at baseline, during treatment at months 1, 2, 3, and 6, at safety follow-up after relugolix discontinuation, and again at 3 and 6 months following discontinuation. Additional endpoints included rates of castrate (<50 ng/dL) and profound castrate (<20 ng/dL) testosterone suppression, recovery of testosterone to >280 ng/dL after discontinuation, and achievement of PSA suppression below 0.2 ng/mL during and after relugolix therapy.
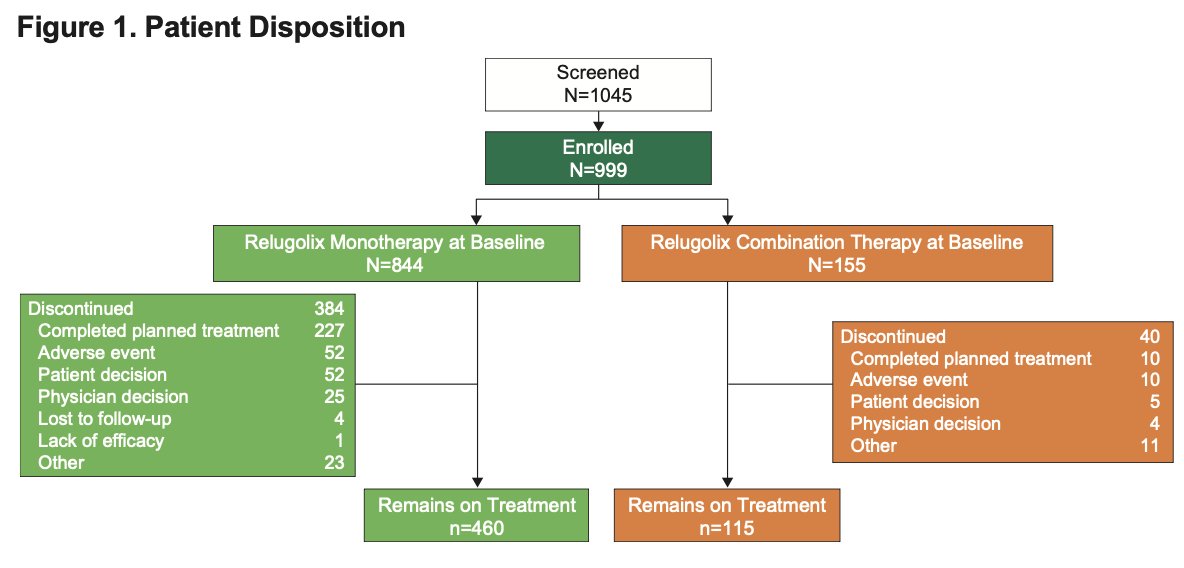
A total of 999 patients were enrolled in the OPTYX study between October 2022 and August 2024 after screening 1,045 patients. Of these, 844 patients (84.5%) initiated relugolix monotherapy, while 155 patients (15.5%) received relugolix combination therapy. At the March 2025 data cutoff, 54.5% of patients receiving monotherapy and 74.2% of those receiving combination therapy remained on relugolix treatment. Among patients who discontinued therapy, the most common reasons were completion of planned treatment, followed by adverse events and patient decision. Discontinuation due to lack of efficacy was rare.
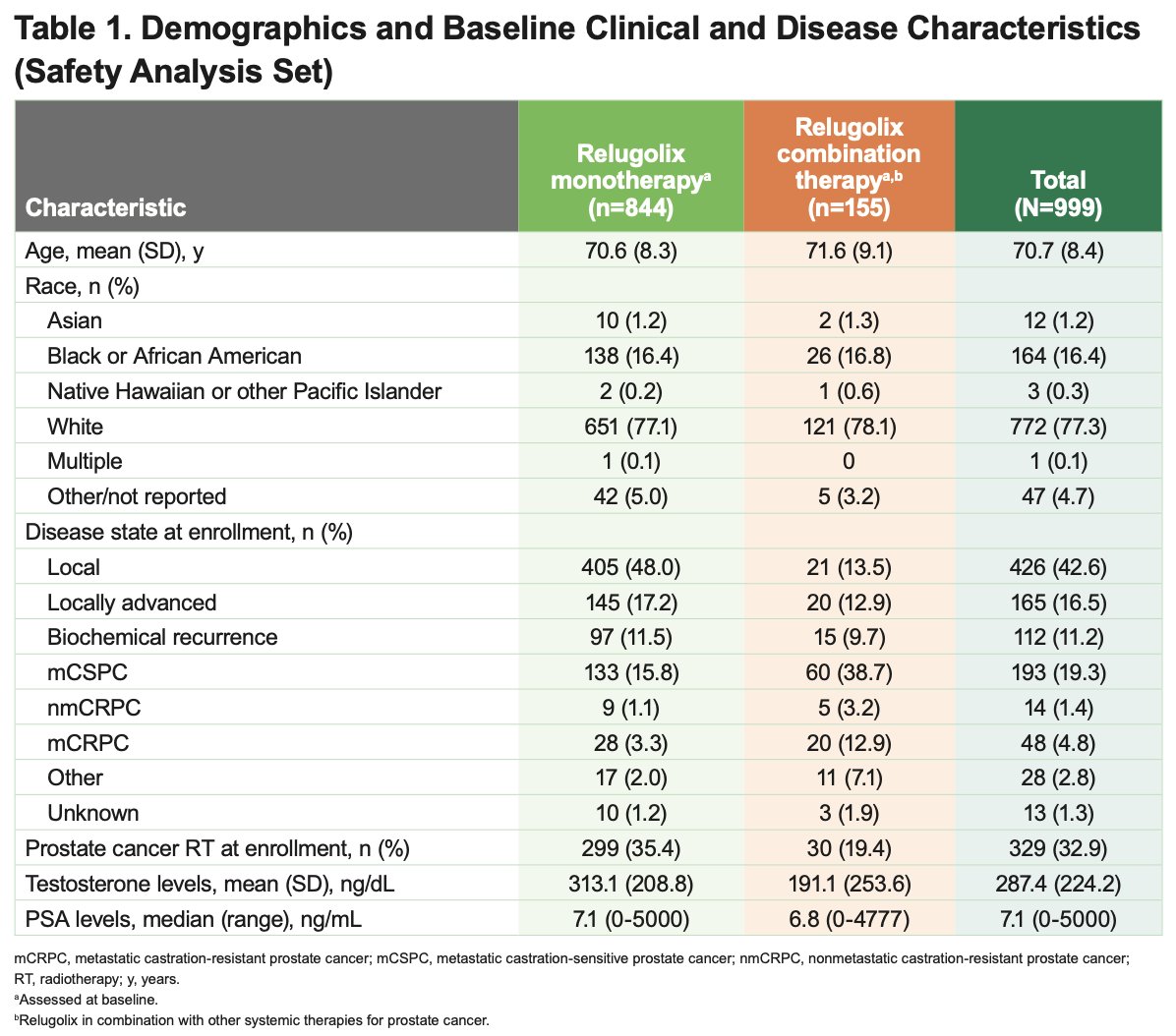
Baseline demographic and disease characteristics are summarized in Table 1 below. The mean age of the overall cohort was 70.7, and the standard deviation (SD) was 8.4 years. Overall, 71.8% of patients had nonmetastatic disease at enrollment, while 24.1% had metastatic disease. Patients receiving relugolix combination therapy were more likely to have advanced disease states, including mCSPC and mCRPC, compared with those receiving monotherapy. Baseline testosterone levels were lower in the combination therapy cohort, whereas PSA levels were generally comparable between groups.
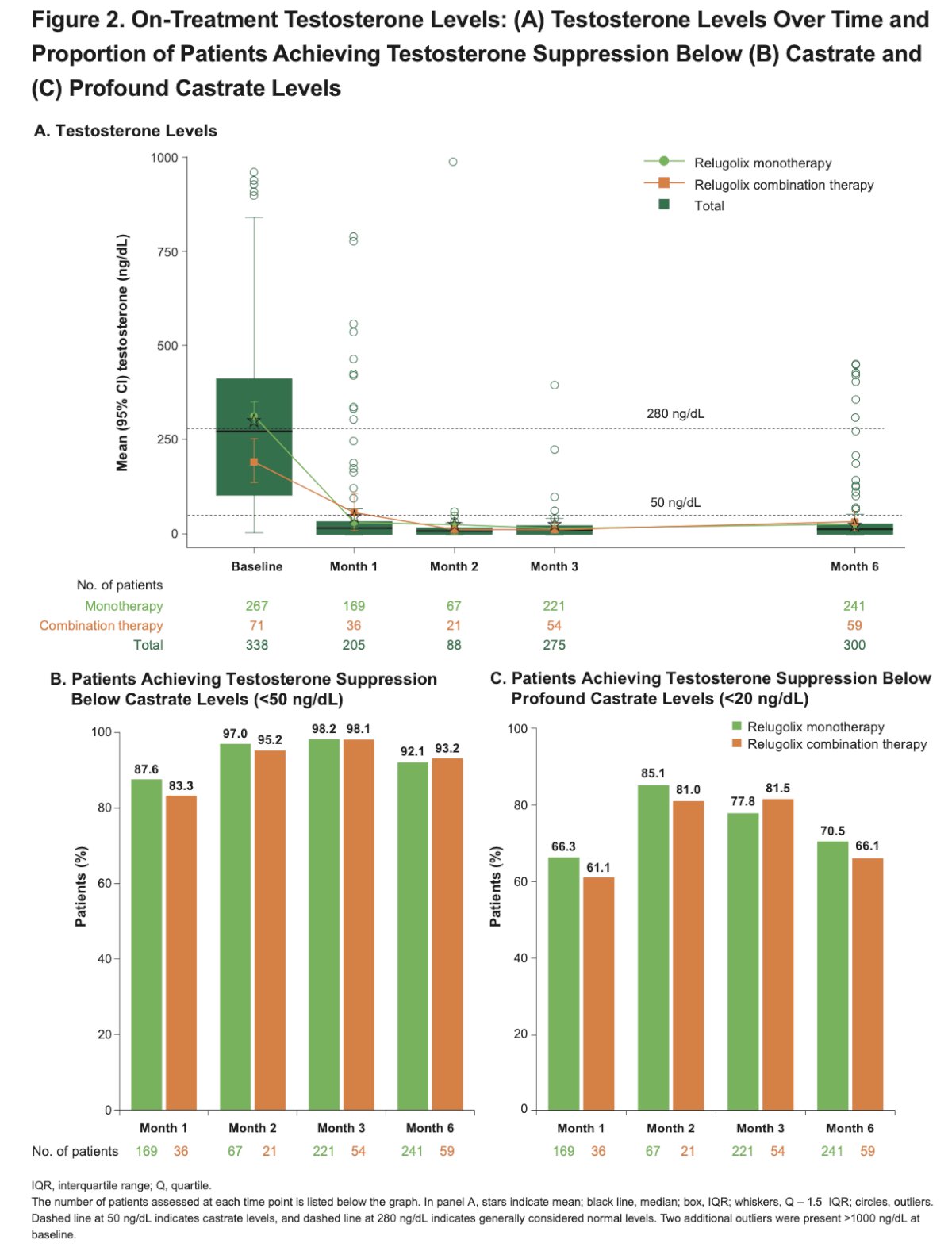
On-treatment testosterone levels declined rapidly and remained suppressed through 6 months in patients receiving both relugolix monotherapy and combination therapy (as shown in Figure 2A below). By Month 6, more than 90% of evaluable patients achieved castrate testosterone levels (<50 ng/dL), while over 66% achieved profound castrate suppression (<20 ng/dL). Rates of testosterone suppression were generally consistent between the monotherapy and combination therapy cohorts throughout treatment.
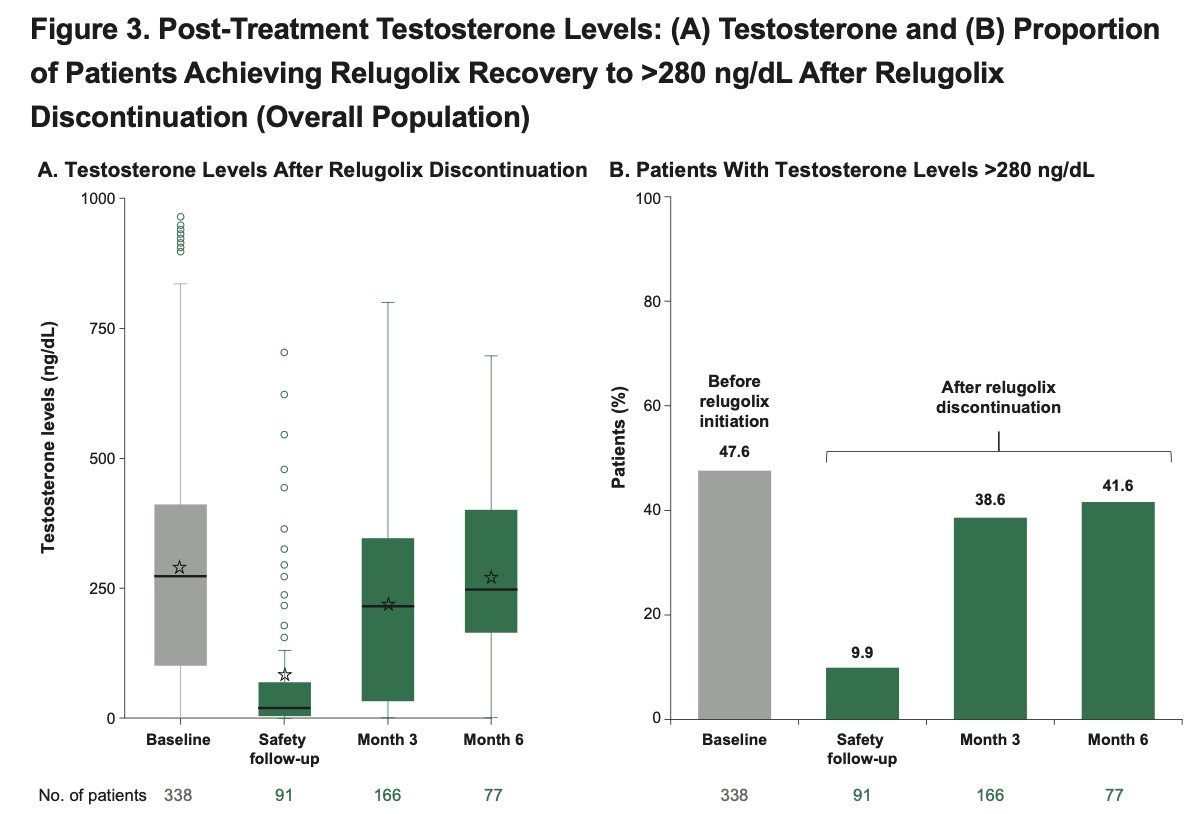
Moreover, among patients who discontinued relugolix and underwent follow-up testosterone assessment, mean testosterone levels began to recover as early as the initial safety follow-up visit after treatment discontinuation, as shown in the figure below. At baseline, prior to relugolix initiation, nearly half of the patients had testosterone levels within the normal range (>280 ng/dL). By 6 months after discontinuation, approximately 42% of evaluable patients had again recovered testosterone levels above 280 ng/dL, supporting relatively rapid hormonal recovery following cessation of therapy in the real-world setting
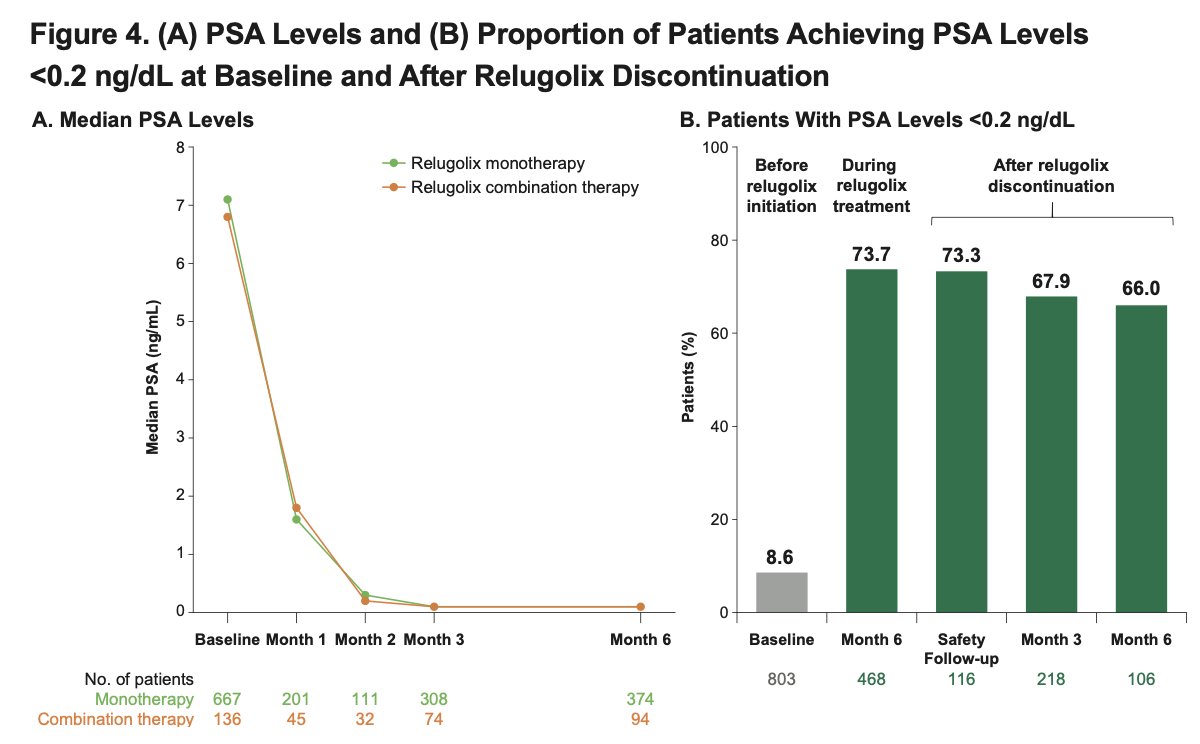
PSA levels also demonstrated sustained suppression during and after relugolix therapy. After 6 months of treatment, median PSA levels had decreased substantially from baseline in both the relugolix monotherapy and combination therapy cohorts. Notably, PSA suppression persisted even after treatment discontinuation, with median PSA levels remaining low through 6 months of follow-up. Additionally, more than 65% of evaluable patients maintained PSA levels below 0.2 ng/mL through 6 months after discontinuing relugolix.
Dr. Lowentritt acknowledged several important limitations of the OPTYX study, including the absence of a comparator arm, the open-label observational design, and incomplete data capture inherent to routine clinical practice. He also noted the potential impact of external confounders such as patient selection bias and variability in treatment settings. In addition, laboratory testing was not mandated by protocol, resulting in inconsistent assessment schedules and smaller or variable sample sizes across different time points and analyses.
Dr. Lowentritt concluded with the following key takeaways:
- Relugolix achieved sustained testosterone suppression during treatment in both the monotherapy and combination therapy cohorts in the real-world setting
- Following treatment discontinuation, many patients experienced recovery of testosterone levels to >280 ng/dL within 3 months, supporting the reversible nature of testosterone suppression with relugolix
- PSA levels declined during therapy and remained stably suppressed through 6 months after treatment discontinuation
- These real-world findings were consistent with outcomes previously observed in the phase III HERO trial, further supporting the clinical effectiveness of relugolix in routine practice
- The OPTYX study remains ongoing, and additional longitudinal outcomes are expected as more follow-up data mature
Presented by: Benjamin Lowentritt, MD, FACS, Medical Director, Prostate Cancer Program, Chesapeake Urology, PA
Written by: Julian Chavarriaga, MD, Clinical Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health @chavarriagaj on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
References:
- Shore ND, Saad F, Cookson MS, George DJ, Saltzstein DR, Tutrone R, Akaza H, Bossi A, van Veenhuyzen DF, Selby B, Fan X, Kang V, Walling J, Tombal B; HERO Study Investigators. Oral Relugolix for Androgen-Deprivation Therapy in Advanced Prostate Cancer. N Engl J Med. 2020 Jun 4;382(23):2187-2196. doi: 10.1056/NEJMoa2004325. Epub 2020 May 29. PMID: 32469183.
- Spratt DE, Dorff T, McKay RR, Lowentritt BH, Fallick M, Gatoulis SC, Flanders SC, Ross AE. Evaluating relugolix for the treatment of prostate cancer in real-world settings of care: the OPTYX study protocol. Future Oncol. 2024 Apr;20(12):727-738. doi: 10.2217/fon-2023-0748. Epub 2024 Mar 15. PMID: 38488039.